2024, 40(12): 2441-2449.
DOI: 10.12449/JCH241214
Abstract:
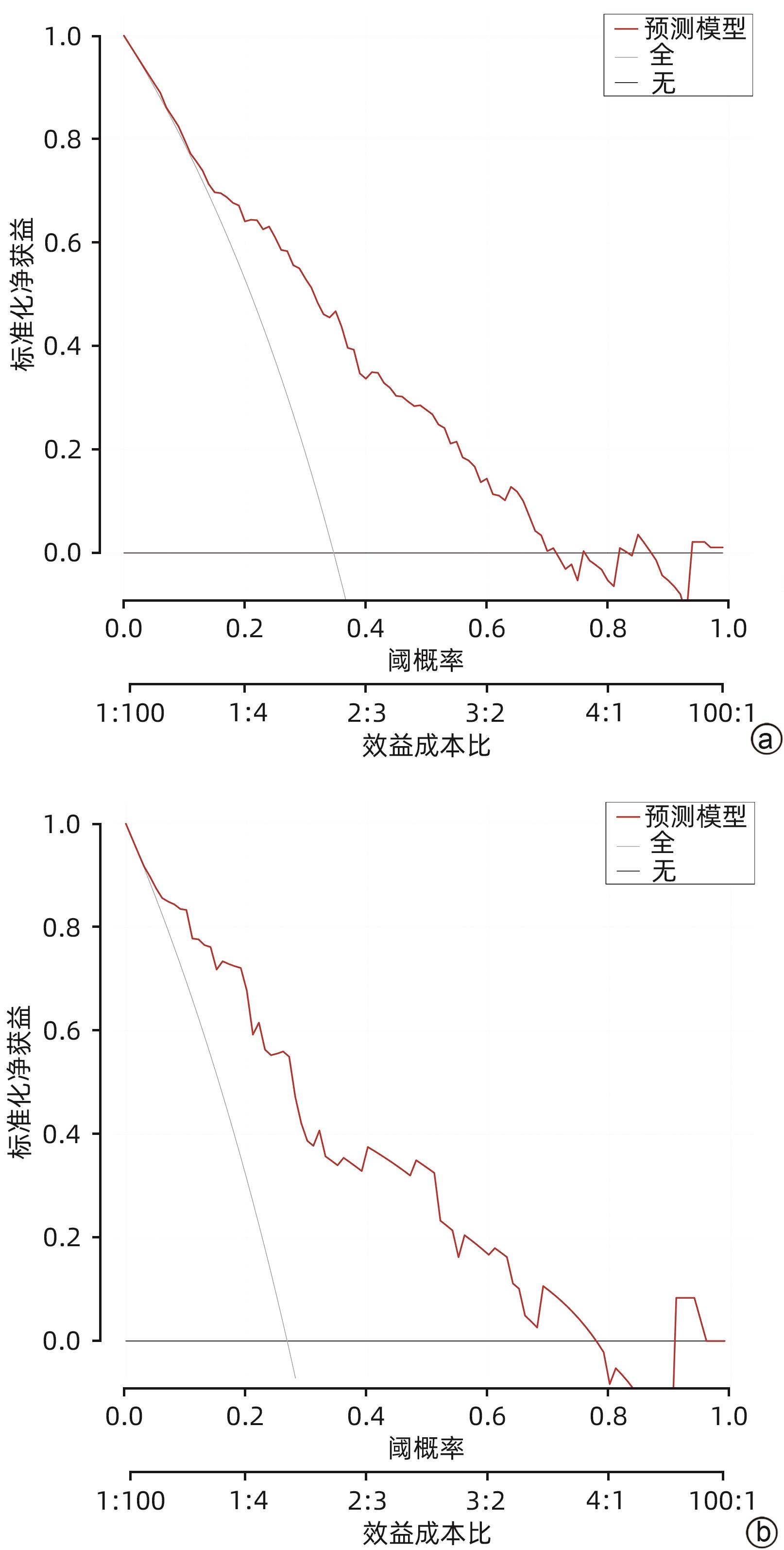
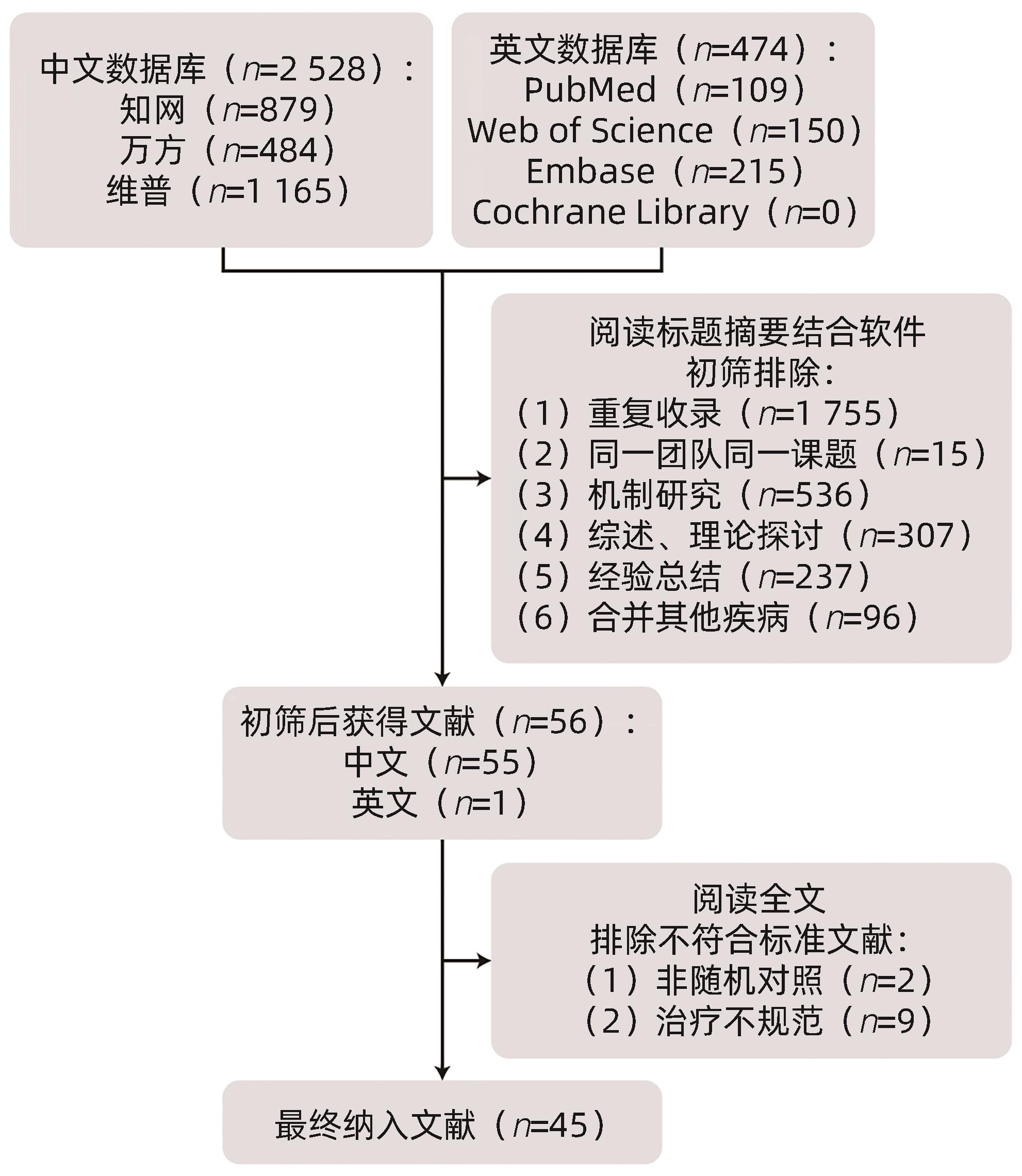
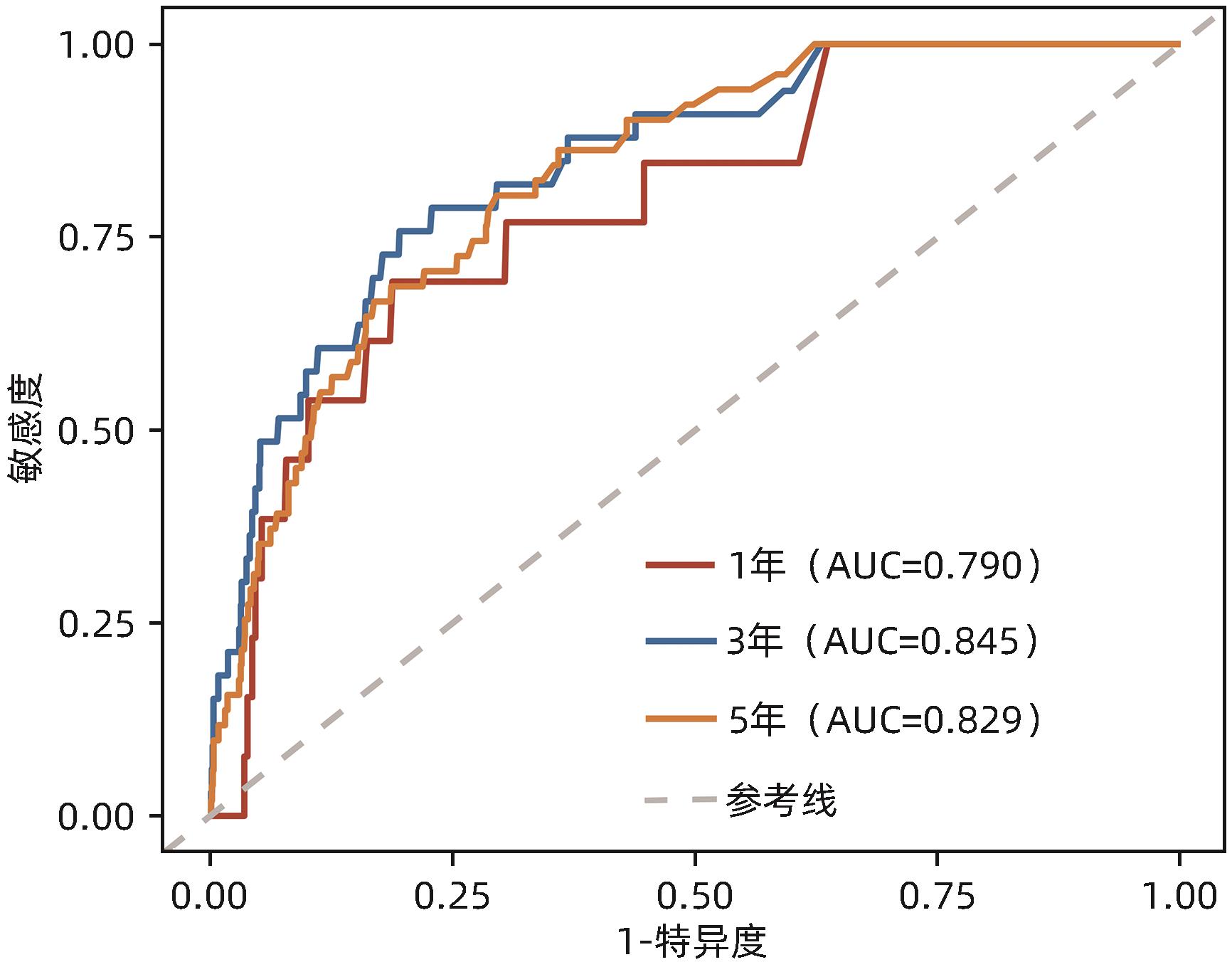
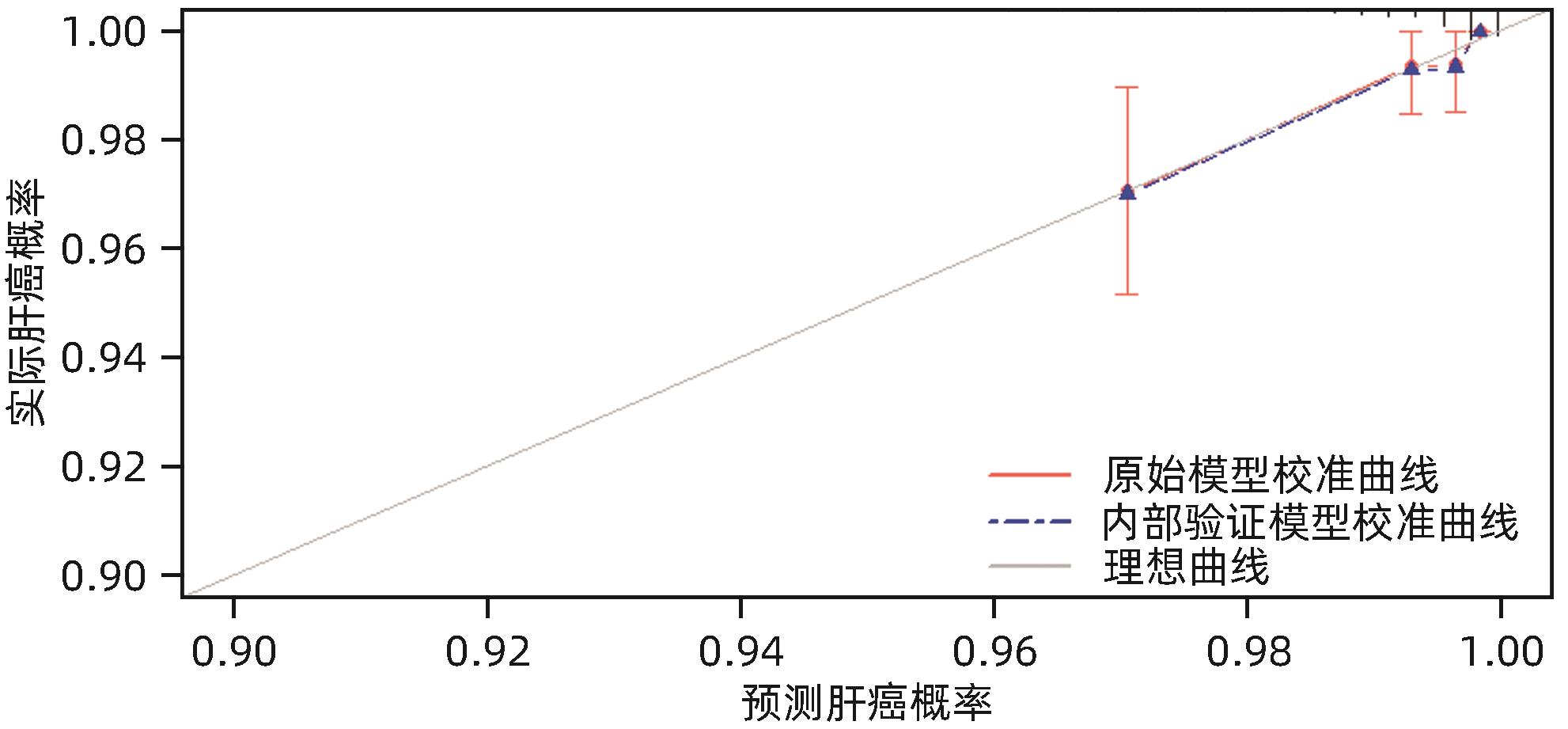
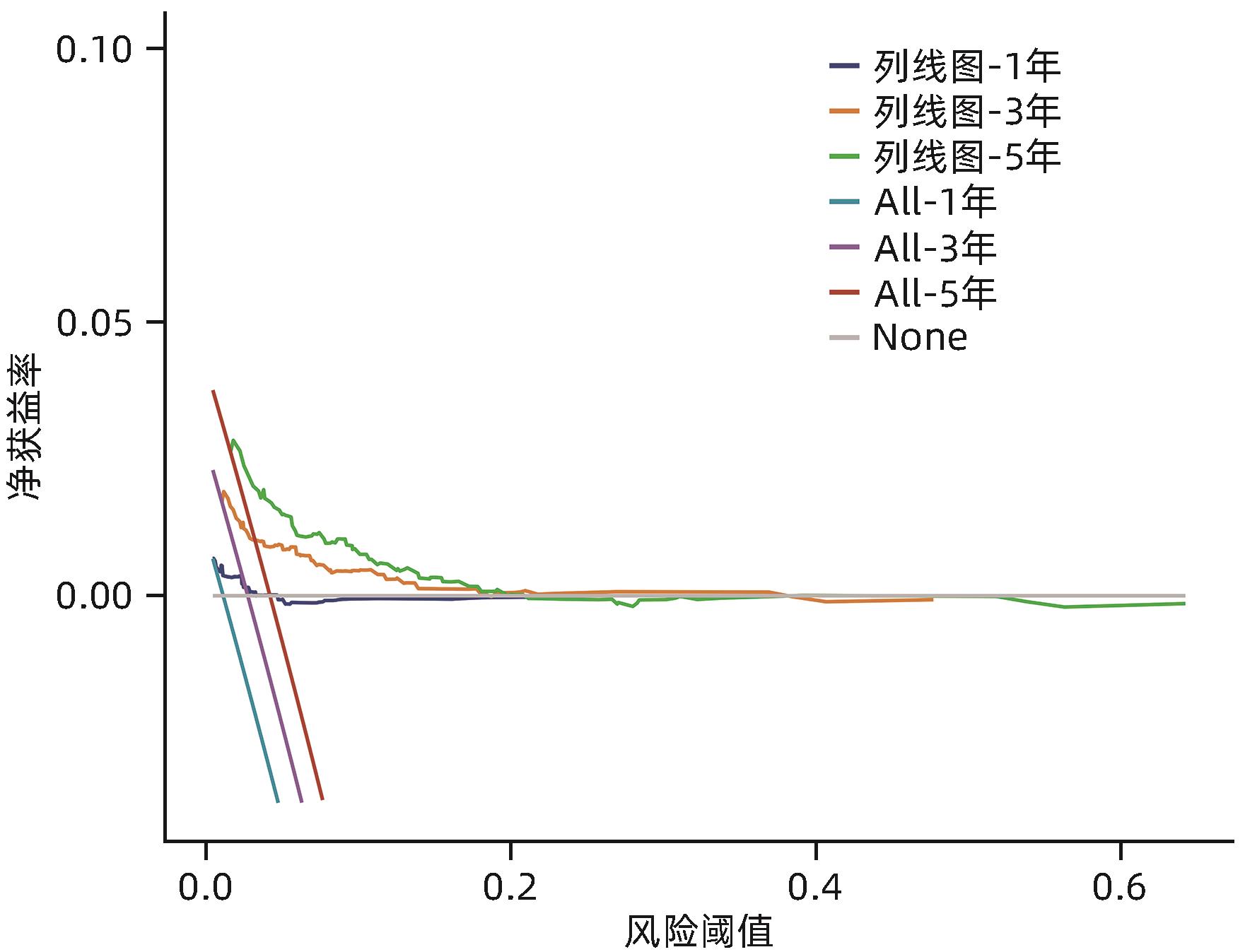
Objective To investigate the risk factors for liver cancer in patients with chronic hepatitis B (CHB) in the Qidong Chronic Hepatitis B cohort, and to construct a nomogram model for predicting the risk of liver cancer in CHB patients. Methods A structured questionnaire survey was conducted among the CHB patients, aged ≥18 years, who attended the outpatient service of Qidong Third People’s Hospital from January 1 to December 31, 2016. The onset of liver cancer was defined as the primary outcome, and the outcomes of the cohort were obtained from Qidong Cancer Registry. Baseline clinical features were compared;between the liver cancer group and the non-liver cancer group. The independent-samples t test or the Mann-Whitney U test was used for comparison of continuous data between two groups, and the chi-square test or the Fisher’s exact test was used for comparison of categorical data between groups. The Cox regression model was used to analyze the risk factors for liver cancer in CHB patients and calculate their hazard ratio (HR) and 95% confidence interval (CI); the variables with statistical significance in the univariate Cox regression analysis were included in the LASSO regression analysis, and then the variables obtained were included in the multivariate Cox regression analysis to establish a predictive model. The nomogram was used to visualize the complex model. The receiver operating characteristic (ROC) curve, index of concordance (C-index), and the calibration curve were used to assess the predictive efficacy of the model, and the decision curve was used to evaluate the clinical practicability of the nomogram. Results A total of 1 479 CHB patients were selected, among whom 58 patients with a confirmed diagnosis of liver cancer, 15 with missing data on testing indicators, and 164 with missing data on important information in the questionnaire were excluded, and finally 1 242 subjects were included in the study. Up to December 31, 2023, there were 67 new cases of liver cancer after a median follow-up time of 7.71 years, and the incidence density of liver cancer was 729.78/100,000 person-years. There were significant differences between the liver cancer group and the non-liver cancer group in age, sex, educational level, liver cirrhosis, duration of liver cirrhosis, history of diabetes mellitus, albumin, total bilirubin (TBil), direct bilirubin, aspartate aminotransferase, aspartate aminotransferase, gamma-glutamyl transpeptidase (GGT), and alkaline phosphatase (all P<0.05). The multivariate Cox regression analysis showed that the increase in age (HR=1.07, 95%CI: 1.05 — 1.10, P<0.001), a relatively high level of TBil (HR=1.98, 95%CI: 1.15 — 3.42, P=0.014), a relatively high level of GGT (HR=2.41, 95%CI: 1.43 — 4.08, P=0.001), and a long duration of liver cirrhosis (HR=1.09, 95%CI: 1.02 — 1.15, P=0.009) were independent risk factors for liver cancer in CHB patients. A nomogram prediction model was constructed based on the above four indicators, with an area under the ROC curve of 0.790, 0.845, and 0.829, respectively, in predicting the risk of liver cancer in CHB patients at 1, 3, and 5 years, and the bootstrap resampling method was used for internal validation and showed a C-index of 0. 778. The calibration curve showed that the prediction model had good stability, and the decision curve showed that it had certain clinical practicability. Conclusion The increase in age, relatively high levels of TBil and GGT, and a long duration of liver cirrhosis are independent risk factors for liver cancer in CHB patients, and the nomogram model constructed based on these factors has a good predictive value and can be used in clinical practice to help develop strategies for the long-term monitoring of liver cancer.
ZHU YC, SHA CX, FAN CS, et al. Risk factors for liver cancer in chronic hepatitis B patients and construction of a nomogram prediction model[J]. J Clin Hepatol, 2024, 40(12): 2441-2449.. doi: 10.12449/JCH241214.

 Abstract
Abstract HTML
HTML PDF (612KB)
PDF (612KB)