Department of Infectious Diseases, Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing 210008, China
Research funding:
Research funding: National Natural Science Foundation of China(81702011);
Research Project of Modern Hospital Management and Development Institute of Nanjing University and Medical Development and Medical Assistance Fund of Nanjing Drum Tower Hospital(NDYG2021016)
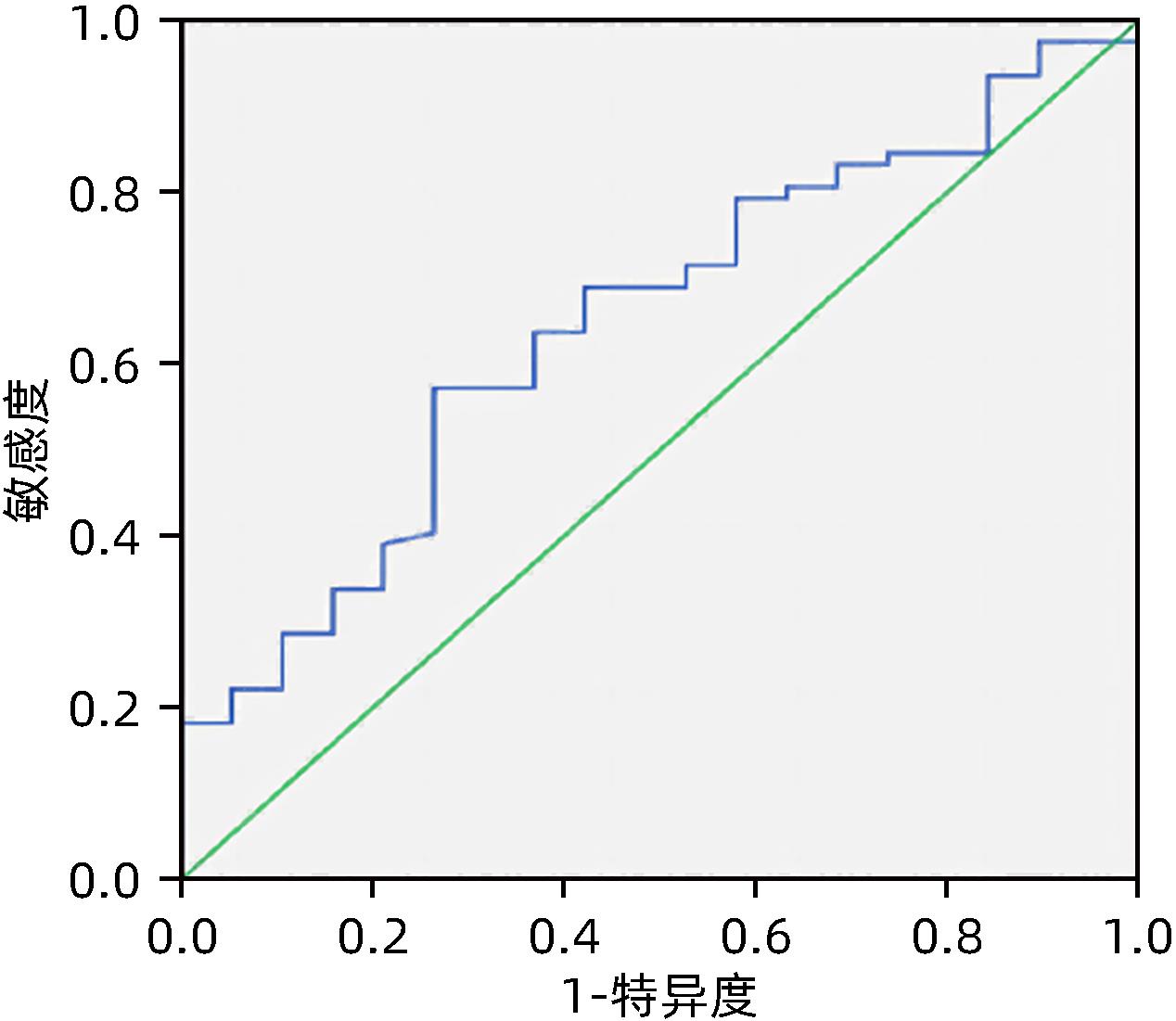
Objective To investigate the value of a risk assessment model in predicting venous thromboembolism (VTE) in patients with liver failure after artificial liver support therapy. Methods A retrospective analysis was performed for the clinical data of 124 patients with liver failure who received artificial liver support therapy in Affiliated Drum Tower Hospital of Nanjing University Medical School from March 2019 to December 2021, among whom there were 41 patients with VTE (observation group) and 143 patients without VTE (control group). Related clinical data were compared between the two groups, and the Caprini risk assessment model was used for scoring and risk classification of the patients in both groups. The t-test was used for comparison of continuous data between two groups; the chi-square test was used for comparison of categorical data between two groups; the Mann-Whitney U rank sum test was used for comparison of ranked data between two groups. The logistic regression analysis was used to investigate the independent risk factors for VTE in patients with liver failure after artificial liver support therapy. The receiver operating characteristic (ROC) curve was used to investigate the value of Caprini score and the multivariate predictive model used alone or in combination in predicting VTE.Results The observation group had a significantly higher Caprini score than the control group (4.39±1.10 vs 3.12±1.04, t=6.805, P < 0.001). There was a significant difference between the two groups in risk classification based on Caprini scale (P < 0.05), and the patients with high risk or extremely high risk accounted for a higher proportion among the patients with VTE. The univariate analysis showed that there were significant differences between the two groups in age (t=6.400, P < 0.001), catheterization method (χ2=14.413, P < 0.001), number of times of artificial liver support therapy (Z=-4.720, P < 0.001), activity (Z=-6.282, P < 0.001), infection (χ2=33.071, P < 0.001), D-dimer (t=8.746, P < 0.001), 28-day mortality rate (χ2=5.524, P=0.022). The multivariate analysis showed that number of times of artificial liver support therapy (X1) (odds ratio [OR]=0.251, 95% confidence interval [CI]: 0.111-0.566, P=0.001), activity (X2) (OR=0.122, 95%CI: 0.056-0.264, P < 0.001), D-dimer (X3) (OR=2.921, 95%CI: 1.114-7.662, P=0.029) were independent risk factors for VTE in patients with liver failure after artificial liver support therapy. The equation for individual predicted probability was P=1/[1+e-(7.425-1.384X1-2.103X2+1.072X3)]. The ROC curve analysis showed that Caprini score had an area under the ROC curve of 0.802 (95%CI: 0.721-0.882, P < 0.001), and the multivariate model had an area under the ROC curve of 0.768 (95%CI: 0.685-0.851, P < 0.001), while the combination of Caprini score and the multivariate model had an area under the ROC curve of 0.957 (95%CI: 0.930-0.984, P < 0.001).Conclusion The Caprini risk assessment model has a high predictive efficiency for the risk of VTE in patients with liver failure after artificial liver support therapy, and its combination with the multivariate predictive model can significantly improve the prediction of VTE.
RAPP CM, SHIELDS EJ, WIATER BP, et al. Venous thromboembolism after shoulder arthoplasty and arthroscopy[J]. J Am Acad Orthop Surg, 2019, 27(8): 265-274. DOI: 10.5435/JAAOS-D-17-00763.
[2]
WANG Q, DING J, YANG R. The venous thromboembolism prophylaxis in patients receiving thoracic surgery: A systematic review[J]. Asia Pac J Clin Oncol, 2021, 17(5): e142-e152. DOI: 10.1111/ajco.13386.
[3]
SI N, LIU F, LIU L, et al. Effect of platelet level and platelet parameters on the prognosis of patients with acute-on-chronic liver failure[J]. J Clin Hepatol, 2022, 38(2): 381-386. DOI: 10.3969/j.issn.1001-5256.2022.02.023.
ZHOU L, CHEN Y. Model selection and curative effect judgment criteria for artificial liver in the treatment of liver failure[J]. Chin J Hepatol, 2022, 30(2): 127-130. DOI: 10.3760/cma.j.cn501113-20220108-00008.
WANG L, XU WX, ZHU Z, et al. Influence of artificial liver support system therapy on platelet in treatment of hepatitis B virus-related acute-on-chronic liver failure[J]. J Clin Hepatol, 2022, 38(5): 1053-1058. DOI: 10.3969/j.issn.1001-5256.2022.05.015.
Liver failure and artificial liver group of infectious diseases branch of Chinese Medical Association, severe liver disease and artificial liver group of Hepatology branch of Chinese Medical Association. Diagnostic and treatment guidelines for liver failure (2012 version)[J]. Chin J Clin Infect Dis, 2012, 5(6): 321-327. DOI: 10.3760/cma.j.issn.1674-2397.2012.06.001.
WU B, DU LY, MA YJ, et al. Effects of different combinations of artificial liver support system on efficacy and inflammatory indexes of patients with hepatitis B virus-related acute-on-chronic liver failure in early and middle stages[J/CD]. Chin J Liver Dis (Electronic Version), 2021, 13(1): 32-38. DOI: 10.3969/j.issn.1674-7380.2021.01.006.
NANCHAL R, SUBRAMANIAN R, KARVELLAS CJ, et al. Guidelines for the management of adult acute and acute-on-chronic liver failure in the ICU: Cardiovascular, endocrine, hematologic, pulmonary, and renal considerations[J]. Crit Care Med, 2020, 48(3): e173-e191. DOI: 10.1097/CCM.0000000000004192.
[9]
MAP YQ, ZHOU XS, WANG X, et al. Study on the correlation between antithrombin Ⅲ activity and short-term prognosis of acute-on-chronic liver failure patients treated with artificial liver support system[J]. Chin Hepatol, 2021, 26(7): 770-775. DOI: 10.3969/j.issn.1008-1704.2021.07.016.
PENG H, XU FF, WAN XQ, et al. Clinical efficacy of artificial liver plasma exchange in treatment of patients with severe hepatitis and influencing factors for prognosis[J]. Clin Misdiagn Misther, 2021, 34(5): 90-95. DOI: 10.3969/j.issn.1002-3429.2021.05.018.
WANG DG, TAN CL, WANG HY, et al. Predictive value of thromboelastogram for postoperative venous thromboembolism in breast cancer patients[J]. Chin J Curr Adv Gen Surg, 2022, 25(1): 23-26, 48. DOI: 10.3969/j.issn.1009-9905.2022.01.005.
ZHANG L, HE JX, FAN XS, et al. Prognostic value of antithrombin Ⅲ activity combined with CLIF-C OFs score in patients with HBV related chronic plus acute liver failure[J]. Chin J Difficult Comp Cases, 2022, 21(1): 36-40, 45. DOI: 10.3969/j.issn.1671-6450.2022.01.007.
YANG P, XIAO LR, YANG N, et al. The evaluation value of procalcitonin and prothrombin activity in the prognosis of liver failure complicated by infection[J]. Chin J Nosocomiol, 2022, 32(4): 531-534. DOI: 10.11816/cn.ni.2022-210509.
WU XJ, ZHAO WL, SU ZZ, et al. Application value of antithrombin Ⅲ in evaluating the disease progression and 28-day mortality of patients with HBV-associated acute-on-chronic liver failure[J]. Chin J Clin Lab Sci, 2020, 38(6): 458-463. DOI: 10.13602/j.cnki.jcls.2020.06.18.
LIN Y, ZENG Z, LIN R, et al. The Caprini thrombosis risk model predicts the risk of peripherally inserted central catheter-related upper extremity venous thrombosis in patients with cancer[J]. J Vasc Surg Venous Lymphat Disord, 2021, 9(5): 1151-1158. DOI: 10.1016/j.jvsv.2020.12.075.
[16]
ZHOU J, WANG QY, QIN CL. Analysis of risk factors for venous thromboembolism after operation of primary liver cancer and application of Caprini risk prediction model[J]. Mod Oncol, 2022, 30(12): 2214-2218. DOI: 10.3969/j.issn.1672-4992.2022.12.021.
MENG R, MA CY. Practice and effect of Caprini risk assessment model in prevention of deep venous thrombosis in ICU patients[J]. Chin J Thromb Hemost, 2017, 23(6): 1054-1056. DOI: 10.3969/j.issn.1009-6213.2017.06.057.
QIAO Y, GUO P, WANG L. Validityan alysis of Caprini thrombosis assessment scale in assessing the risk of venous thromboembolism in liver failure patients treated with artificial liver[J]. Acta Acad Med Bengbu, 2020, 45(1): 120-123. DOI: 10.13898/j.cnki.issn.1000-2200.2020.01.031.
MA LX, WEI XH, CAO ZH, et al. Association between serum endothelial cell-specific molecule 1 and cirrhotic cardiomyopathy[J]. J Clin Hepatol, 2024, 40(6):1156-1161. DOI: 10.12449/JCH240614.
MA LX, WEI XH, CAO ZH, et al. Association between serum endothelial cell-specific molecule 1 and cirrhotic cardiomyopathy[J]. J Clin Hepatol, 2024, 40(6):1156-1161. DOI: 10.12449/JCH240614.
Figure 1. ROC curve analysis of the predictive value of Caprini score, multifactor model and their combination on the occurrence of VTE in patients with liver failure undergoing artificial liver therapy

 下载:
下载:






 DownLoad:
DownLoad: