
 PDF下载 ( 1457 KB)
PDF下载 ( 1457 KB)

甘油三酯-葡萄糖指数、甘油三酯-葡萄糖-体重指数对胰体尾切除术后新发糖尿病的预测价值
DOI: 10.12449/JCH260619
Association of triglyceride-glucose index and triglyceride-glucose-body mass index with new-onset diabetes mellitus after distal pancreatectomy
-
摘要:
目的 探讨甘油三酯-葡萄糖指数(TyG)及甘油三酯-葡萄糖-体重指数(TyG-BMI)与胰体尾切除术(DP)后新发糖尿病(NODM)的关系,并评价其临床应用价值。 方法 回顾性收集2020年1月—2024年12月于新疆医科大学第一附属医院接受DP且术前无糖尿病的161例患者资料。根据术后是否发生NODM将其分为NODM组(n=43)与非NODM组(n=118),比较其基线临床资料。采用多因素Logistic回归分析TyG及TyG-BMI与NODM的关系,并通过限制性立方样条模型分析TyG及TyG-BMI与NODM风险的剂量-反应关系。采用受试者操作特征曲线(ROC曲线)评估TyG及TyG-BMI对NODM的预测效能。 结果 161例患者中,术后NODM发生率为26.7%(43/161)。NODM组患者的TyG[(8.89±0.57) vs (8.54±0.56),P<0.001]及TyG-BMI[232.18(195.31~249.68) vs 195.39(178.92~221.38),P<0.001]均显著高于非NODM组。多因素Logistic回归分析结果显示,在调整年龄、性别及糖化血红蛋白后,TyG[比值比(OR)=2.78,95%置信区间(CI):1.43~5.39,P=0.003)及TyG-BMI(OR=1.02,95%CI:1.01~1.04,P<0.001)仍为DP术后NODM发生的独立危险因素。限制性立方样条分析提示,TyG及TyG-BMI与NODM发生风险均呈近似线性正相关。ROC曲线分析表明,TyG与TyG-BMI预测DP术后NODM的曲线下面积分别为0.725(95%CI:0.683~0.867)和0.719(95%CI:0.610~0.810),表现出中等的预测价值。 结论 TyG与TyG-BMI是DP术后发生NODM的独立预测因子,二者对NODM的诊断具有一定的预测效能。提示这两种简便的代谢指标有望成为临床早期识别DP术后NODM高危人群的辅助工具。 -
关键词:
- 胰体尾切除术 /
- 糖尿病 /
- 甘油三酯-葡萄糖指数 /
- 体重指数
Abstract:Objective To investigate the value of triglyceride-glucose index (TyG) and triglyceride-glucose-body mass index (TyG-BMI) in predicting new-onset diabetes mellitus (NODM) after distal pancreatectomy (DP). Methods A retrospective analysis was performed for the clinical data of 161 patients without diabetes before surgery who underwent DP in The First Affiliated Hospital of Xinjiang Medical University from January 2020 to December 2024, and according to the presence or absence of NODM after surgery, they were divided into NODM group and non-NODM group. Baseline clinical data were compared between groups. A multivariate logistic regression analysis was used to investigate the association of TyG and TyG-BMI with NODM, and the restricted cubic spline model was used to analyze the dose-response relationship between TyG/TyG-BMI and the risk of NODM. The receiver operating characteristic (ROC) curve was used to assess the performance of TyG and TyG-BMI in predicting NODM. Results Among the 161 patients included in the analysis, 43 (26.7%) developed NODM after DP. Compared with the non-NODM group, the NODM group had significantly higher TyG (8.89±0.57 vs 8.54±0.56, P<0.001) and TyG-BMI [232.18 (195.31 — 249.68) vs 195.39 (178.92 — 221.38), P<0.001]. The multivariate logistic regression analysis showed that after adjustment for age, sex, and hemoglobin A1c, both TyG (odds ratio [OR]=2.78, 95% confidence interval [CI]: 1.43 — 5.39, P=0.003) and TyG-BMI (OR=1.02, 95%CI: 1.01 — 1.04, P<0.001) remained independent risk factors for NODM after DP. The restricted cubic spline analysis showed an approximately linear positive correlation between TyG/TyG-BMI and the risk of NODM. The ROC curve analysis showed that TyG and TyG-BMI had a moderate predictive value for NODM after DP, with an area under the ROC curve of 0.725 (95%CI: 0.683 — 0.867) and 0.719 (95%CI: 0.610 — 0.810), respectively. Conclusion TyG and TyG-BMI are independent predictive factors for the onset of NODM after DP, with a certain predictive value in the diagnosis of NODM. These two simple metabolic indicators may become helpful tools for the early identification of patients at a high risk of NODM after DP. -
Key words:
- Distal Pancreatectomy /
- Diabetes Mellitus /
- Triglyceride-Glucose Index /
- Body Mass Index
-
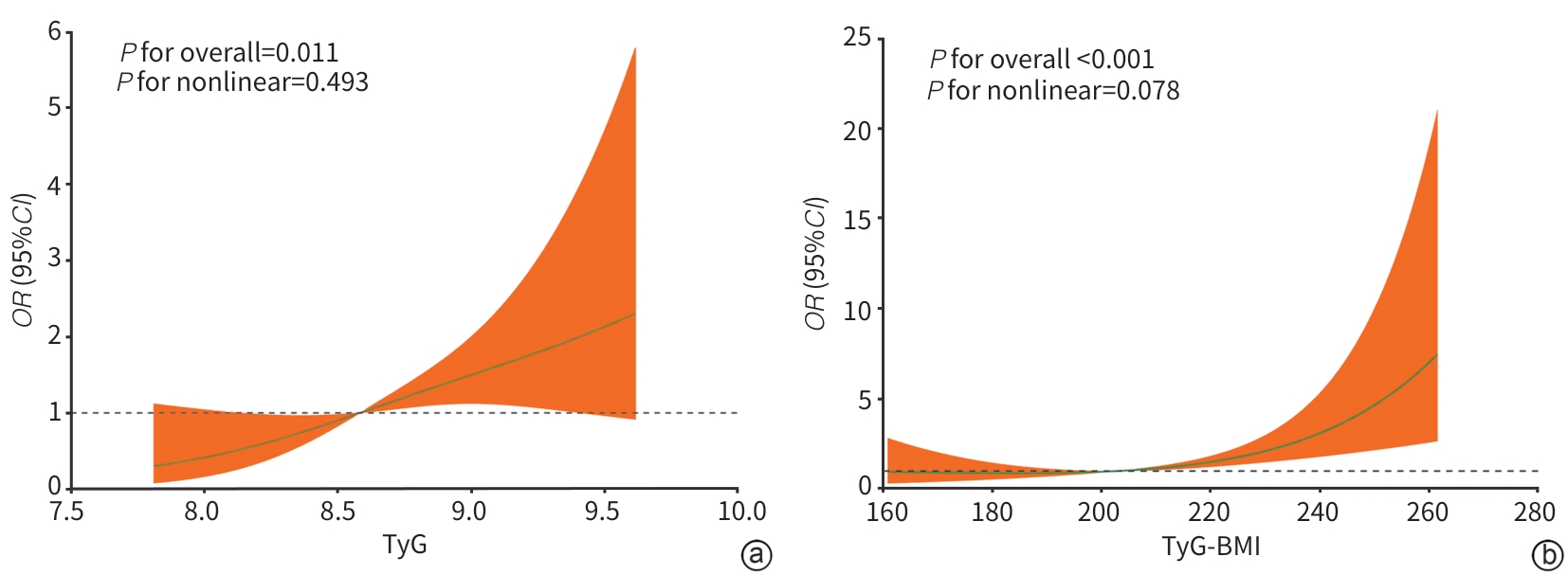
注: a,TyG与NODM发生风险;b,TyG-BMI与NODM发生风险。NODM,新发糖尿病;TyG,甘油三酯-葡萄糖指数;TyG-BMI,甘油三酯-葡萄糖-体重指数;OR,比值比;CI,置信区间。
图 1 TyG、TyG-BMI与NODM风险的限制性立方样条曲线
Figure 1. Restricted cubic spline curves for the association between TyG, TyG-BMI, and the risk of NODM
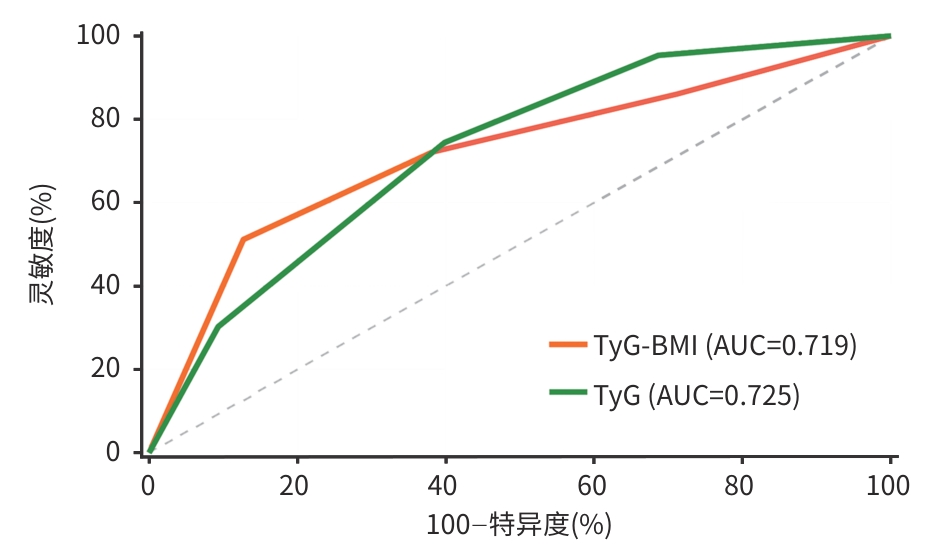
注: AUC,曲线下面积;NODM,新发糖尿病;TyG,甘油三酯-葡萄糖指数;TyG-BMI,甘油三酯-葡萄糖-体重指数;DP,胰体尾切除术。
图 2 TyG、TyG-BMI预测DP术后NODM的ROC曲线
Figure 2. ROC curves of TyG and TyG-BMI for predicting NODM after DP
表 1 NODM和非NODM组基线资料比较
Table 1. Comparison of baseline characteristics between the NODM group and non-NODM group
变量 非NODM组(n=118) NODM组(n=43) 统计值 P值 年龄(岁) 50.69±14.59 56.16±14.73 t=-2.10 0.037 低密度脂蛋白(mmol/L) 2.55±0.83 2.61±0.72 t=-0.39 0.697 TyG 8.54±0.56 8.89±0.57 t=-3.49 <0.001 BMI(kg/m2) 23.00(21.00~26.00) 25.00(21.00~28.00) Z=-1.60 0.110 白细胞(×109/L) 5.62(4.50~7.03) 5.69(4.77~7.49) Z=-0.88 0.380 中性粒细胞(×109/L) 3.34(2.72~4.49) 3.54(2.91~4.58) Z=-0.83 0.408 血红蛋白(g/L) 132.50(123.00~142.75) 131.00(116.50~141.50) Z=-0.61 0.540 总胆红素(µmmol/L) 14.23(10.99~18.47) 14.38(11.62~19.33) Z=-0.29 0.770 白蛋白(g/L) 41.95(39.19~43.90) 41.84(37.21~45.20) Z=-0.09 0.928 天冬氨酸氨基转移酶(U/L) 26.11(22.27~33.97) 24.03(20.73~27.70) Z=-2.10 0.036 丙氨酸氨基转移酶(U/L) 22.97(17.79~32.40) 21.08(17.98~29.29) Z=-0.92 0.355 空腹血浆葡萄糖(mmol/L) 4.88(4.50~5.57) 5.22(4.91~6.62) Z=-3.21 0.001 糖化血红蛋白(%) 5.70(5.12~5.90) 5.70(5.35~6.12) Z=-1.02 0.308 甘油三酯(mmol/L) 1.14(0.88~1.70) 1.38(0.98~1.97) Z=-1.30 0.193 总胆固醇(mmol/L) 4.18(3.45~4.96) 4.32(3.59~5.18) Z=-0.86 0.391 高密度脂蛋白(mmol/L) 1.01(0.79~1.21) 0.94(0.74~1.23) Z=-0.29 0.773 手术时间(h) 6.12(4.67~8.40) 6.25(5.28~7.82) Z=-0.85 0.397 术中出血量(mL) 500.0(300.0~775.0) 500.0(400.0~750.0) Z=-0.26 0.796 TyG-BMI 195.39(178.92~221.38) 232.18(195.31~249.68) Z=-4.07 <0.001 性别[例(%)] χ2=0.22 0.639 女 68(57.63) 23(53.49) 男 50(42.37) 20(46.51) 糖尿病家族史[例(%)] 14(11.86) 15(34.88) χ2=0.47 0.467 吸烟史[例(%)] 30(25.42) 10(23.26) χ2=0.08 0.778 饮酒史[例(%)] 27(22.88) 8(18.60) χ2=0.34 0.561 胰管扩张[例(%)] 26(22.03) 13(30.23) χ2=1.15 0.283 脾切除[例(%)] 40(33.90) 19(44.19) χ2=1.44 0.231 肿瘤类型[例(%)] χ2=0.52 0.470 恶性肿瘤 29(24.58) 13(30.23) 其他 89(75.42) 30(69.77) 肿瘤大小[例(%)] χ2=0.03 0.872 ≤5 cm 73(61.86) 26(60.47) >5 cm 45(38.14) 17(39.53) 切除胰腺占比[例(%)] χ2=1.76 0.185 ≤50% 109(92.37) 36(83.72) >50% 9(7.63) 7(16.28) TyG四分位数[例(%)] χ2=20.98 <0.001 Q1组 37(31.36) 2(4.65) Q2组 34(28.81) 9(20.93) Q3组 36(30.51) 19(44.19) Q4组 11(9.32) 13(30.23) TyG-BMI四分位数[例(%)] χ2=27.45 <0.001 Q1组 34(28.81) 6(13.95) Q2组 39(33.05) 6(13.95) Q3组 30(25.42) 9(20.93) Q4组 15(12.71) 22(51.16) 注:NODM,新发糖尿病;TyG,甘油三酯-葡萄糖指数;TyG-BMI,甘油三酯-葡萄糖-体重指数;BMI,体重指数。
 下载: 导出CSV
下载: 导出CSV
表 2 TyG、TyG-BMI与NODM关系的Logistic回归分析
Table 2. Logistic regression analysis of TyG and TyG-BMI with NODM
变量 模型1 模型2 模型3 OR(95%CI) P值 OR(95%CI) P值 OR(95%CI) P值 TyG 2.85(1.51~5.37) <0.001 2.70(1.41~5.18) 0.003 2.78(1.43~5.39) 0.003 TyG四分位数 Q1组 Ref Ref Ref Q2组 2.90(0.99~4.29) 0.052 2.32(0.86~4.69) 0.076 2.46(0.88~4.48) 0.070 Q3组 3.76(2.12~4.98) 0.003 3.10(1.96~4.32) 0.005 3.70(2.06~5.66) 0.004 Q4组 2.86(1.27~5.01) <0.001 2.12(1.85~6.02) <0.001 2.61(1.07~4.80) <0.001 TyG-BMI 1.02(1.01~1.04) <0.001 1.02(1.01~1.04) <0.001 1.02(1.01~1.04) <0.001 TyG-BMI四分位数 Q1组 Ref Ref Ref Q2组 0.87(0.26~2.96) 0.826 0.87(0.25~3.01) 0.832 0.87(0.25~2.99) 0.821 Q3组 1.70(0.54~5.34) 0.363 1.72(0.54~5.51) 0.360 1.72(0.54~5.51) 0.363 Q4组 4.31(2.80~8.67) <0.001 4.56(2.82~7.96) <0.001 4.61(2.83~6.15) <0.001 注:模型1,未调整;模型2,调整性别、年龄;模型3,调整性别、年龄和糖化血红蛋白。NODM,新发糖尿病;TyG,甘油三酯-葡萄糖指数;TyG-BMI,甘油三酯-葡萄糖-体重指数;OR,比值比;CI,置信区间。
下载: 导出CSV
-
[1] ARYA S, VENTIN M, ZHANG LT, et al. Long-term outcomes of spleen-preserving distal pancreatectomy with or without preservation of splenic vessels: A bi-institutional experience[J]. Ann Surg, 2025. DOI: 10.1097/SLA.0000000000006992.[ Epub ahead of print] [2] LU WH, LIAO TK, SU PJ, et al. A simple five-factor risk model for predicting new-onset diabetes after distal pancreatectomy[J]. Am J Surg, 2026, 251: 116715. DOI: 10.1016/j.amjsurg.2025.116715. [3] HART PA, BELLIN MD, ANDERSEN DK, et al. Type 3c(pancreatogenic) diabetes mellitus secondary to chronic pancreatitis and pancreatic cancer[J]. Lancet Gastroenterol Hepatol, 2016, 1( 3): 226- 237. DOI: 10.1016/S2468-1253(16)30106-6. [4] DUGGAN SN, EWALD N, KELLEHER L, et al. The nutritional management of type 3c(pancreatogenic) diabetes in chronic pancreatitis[J]. Eur J Clin Nutr, 2017, 71( 1): 3- 8. DOI: 10.1038/ejcn.2016.127. [5] WAILI A, RUZIMAIMAITI M, JIA YZ, et al. New-onset diabetes mellitus after distal pancreatectomy research status, trends, and risk factors[J]. Int J Surg, 2025. DOI: 10.1097/JS9.0000000000004229.[ Epub ahead of print] [6] SAMUEL VT, SHULMAN GI. Mechanisms for insulin resistance: Common threads and missing links[J]. Cell, 2012, 148( 5): 852- 871. DOI: 10.1016/j.cell.2012.02.017. [7] PERRY RJ, SAMUEL VT, PETERSEN KF, et al. The role of hepatic lipids in hepatic insulin resistance and type 2 diabetes[J]. Nature, 2014, 510( 7503): 84- 91. DOI: 10.1038/nature13478. [8] CHEN LP, QIN GH, LIU YH, et al. Label-free optical metabolic imaging of adipose tissues for prediabetes diagnosis[J]. Theranostics, 2023, 13( 11): 3550- 3567. DOI: 10.7150/thno.82697. [9] HAMEDI-SHAHRAKI S, KLISIC A, AMIRKHIZI F, et al. Association of the triglyceride-glucose index with inflammatory markers and dysregulation of adipokines in patients with metabolic syndrome[J]. BMC Endocr Disord, 2026, 26( 1): 44. DOI: 10.1186/s12902-025-02142-5. [10] JOG KS, EAGAPPAN S, SANTHARAM RK, et al. Comparison of novel biomarkers of insulin resistance with homeostasis model assessment of insulin resistance, its correlation to metabolic syndrome in south Indian population and proposition of population specific cutoffs for these indices[J]. Cureus, 2023, 15( 1): e33653. DOI: 10.7759/cureus.33653. [11] GUERRERO-ROMERO F, VILLALOBOS-MOLINA R, JIMÉNEZ-FLORES JR, et al. Fasting triglycerides and glucose index as a diagnostic test for insulin resistance in young adults[J]. Arch Med Res, 2016, 47( 5): 382- 387. DOI: 10.1016/j.arcmed.2016.08.012. [12] TAHAPARY DL, PRATISTHITA LB, FITRI NA, et al. Challenges in the diagnosis of insulin resistance: Focusing on the role of HOMA-IR and Tryglyceride/glucose index[J]. Diabetes Metab Syndr, 2022, 16( 8): 102581. DOI: 10.1016/j.dsx.2022.102581. [13] MARATHE PH, GAO HX, CLOSE KL. American diabetes association standards of medical care in diabetes 2017[J]. J Diabetes, 2017, 9( 4): 320- 324. DOI: 10.1111/1753-0407.12524. [14] LEE JS, SOHN M, KIM K, et al. Glucose regulation after partial pancreatectomy: A comparison of pancreaticoduodenectomy and distal pancreatectomy in the short and long term[J]. Diabetes Metab J, 2023, 47( 5): 703- 714. DOI: 10.4093/dmj.2022.0205. [15] JIANG JJ, WEI DL, REN HB, et al. Safety and efficacy of total pancreatectomy for pancreatic cancer and literature review[J/OL]. Chin J Hepat Surg(Electronic Edition), 2025, 14( 2): 281- 289. DOI: 10.3877/cma.j.issn.2095-3232.2025036蒋佳君, 韦德令, 任洪冰, 等. 全胰腺切除术治疗胰腺癌安全性和疗效分析并文献复习[J/OL]. 中华肝脏外科手术学电子杂志, 2025, 14( 2): 281- 289. DOI: 10.3877/cma.j.issn.2095-3232.2025036 [16] DAI MH, XING C, SHI N, et al. Risk factors for new-onset diabetes mellitus after distal pancreatectomy[J]. BMJ Open Diabetes Res Care, 2020, 8( 2): e001778. DOI: 10.1136/bmjdrc-2020-001778. [17] BELYAEV O, HERZOG T, CHROMIK AM, et al. Early and late postoperative changes in the quality of life after pancreatic surgery[J]. Langenbecks Arch Surg, 2013, 398( 4): 547- 555. DOI: 10.1007/s00423-013-1076-3. [18] SIMENTAL-MENDÍA LE, RODRÍGUEZ-MORÁN M, GUERRERO-ROMERO F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects[J]. Metab Syndr Relat Disord, 2008, 6( 4): 299- 304. DOI: 10.1089/met.2008.0034. [19] GUERRERO-ROMERO F, SIMENTAL-MENDÍA LE, GONZÁLEZ-ORTIZ M, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp[J]. J Clin Endocrinol Metab, 2010, 95( 7): 3347- 3351. DOI: 10.1210/jc.2010-0288. [20] ZHENG DZ, CAI JM, XU SF, et al. The association of triglyceride-glucose index and combined obesity indicators with chest pain and risk of cardiovascular disease in American population with pre-diabetes or diabetes[J]. Front Endocrinol, 2024, 15: 1471535. DOI: 10.3389/fendo.2024.1471535. [21] DANG KK, WANG XY, HU JX, et al. The association between triglyceride-glucose index and its combination with obesity indicators and cardiovascular disease: NHANES 2003-2018[J]. Cardiovasc Diabetol, 2024, 23( 1): 8. DOI: 10.1186/s12933-023-02115-9. [22] SHEN RH, LIN L, BIN ZX, et al. The U-shape relationship between insulin resistance-related indexes and chronic kidney disease: A retrospective cohort study from National Health and Nutrition Examination Survey 2007-2016[J]. Diabetol Metab Syndr, 2024, 16( 1): 168. DOI: 10.1186/s13098-024-01408-7. [23] XIAO SC, ZHANG Q, YANG HY, et al. The association between triglyceride glucose-body mass index and all-cause and cardiovascular mortality in diabetes patients: A retrospective study from NHANES database[J]. Sci Rep, 2024, 14( 1): 13884. DOI: 10.1038/s41598-024-63886-z. [24] CAMPOS MUÑIZ C, LEÓN-GARCÍA PE, SERRATO DIAZ A, et al. Diabetes mellitus prediction based on the triglyceride and glucose index[J]. Med Clin, 2023, 160( 6): 231- 236. DOI: 10.1016/j.medcli.2022.07.003. [25] ADAMS-HUET B, JIALAL I. An increasing triglyceride-glucose index is associated with a pro-inflammatory and pro-oxidant phenotype[J]. J Clin Med, 2024, 13( 13): 3941. DOI: 10.3390/jcm13133941. [26] TIAN X, CHEN SH, WANG PL, et al. Insulin resistance mediates obesity-related risk of cardiovascular disease: A prospective cohort study[J]. Cardiovasc Diabetol, 2022, 21( 1): 289. DOI: 10.1186/s12933-022-01729-9. [27] VARRA FN, VARRAS M, VARRA VK, et al. Molecular and pathophysiological relationship between obesity and chronic inflammation in the manifestation of metabolic dysfunctions and their inflammation-mediating treatment options(Review)[J]. Mol Med Rep, 2024, 29( 6): 95. DOI: 10.3892/mmr.2024.13219. [28] KOJTA I, CHACIŃSKA M, BŁACHNIO-ZABIELSKA A. Obesity, bioactive lipids, and adipose tissue inflammation in insulin resistance[J]. Nutrients, 2020, 12( 5): 1305. DOI: 10.3390/nu12051305. [29] GURIA S, HOORY A, DAS S, et al. Adipose tissue macrophages and their role in obesity-associated insulin resistance: An overview of the complex dynamics at play[J]. Biosci Rep, 2023, 43( 3): BSR20220200. DOI: 10.1042/BSR20220200. [30] LU X, XIE QX, PAN XH, et al. Type 2 diabetes mellitus in adults: Pathogenesis, prevention and therapy[J]. Signal Transduct Target Ther, 2024, 9( 1): 262. DOI: 10.1038/s41392-024-01951-9. [31] GAO J, DONG XW, SHI XL, et al. The association between pancreatic diseases and pancreatic fat content: A cross-sectional study from the UK Biobank[J]. Front Endocrinol, 2025, 16: 1591652. DOI: 10.3389/fendo.2025.1591652. [32] DONG XW, ZHU QT, YUAN CC, et al. Associations of intrapancreatic fat deposition with incident diseases of the exocrine and endocrine pancreas: A UK biobank prospective cohort study[J]. Am J Gastroenterol, 2024, 119( 6): 1158- 1166. DOI: 10.14309/ajg.0000000000002792. [33] CALDART F, de PRETIS N, LUCHINI C, et al. Pancreatic steatosis and metabolic pancreatic disease: A new entity?[J]. Intern Emerg Med, 2023, 18( 8): 2199- 2208. DOI: 10.1007/s11739-023-03364-y. [34] WANG JJ, CAI ZH, LI HS, et al. The nomogram model based on the insulin resistance metabolic index and the triglyceride-glucose index for predicting diabetes after acute pancreatitis[J]. Clin J Med Offic, 2026, 54( 2): 190- 193. DOI: 10.16680/j.1671-3826.2026.02.20.王菁菁, 蔡兆辉, 李海山, 等. 基于胰岛素抵抗代谢指数、甘油三酯-葡萄糖指数列线图模型对急性胰腺炎后糖尿病预测价值[J]. 临床军医杂志, 2026, 54( 2): 190- 193. DOI: 10.16680/j.1671-3826.2026.02.20. [35] PETROV MS, TAYLOR R. Intra-pancreatic fat deposition: Bringing hidden fat to the fore[J]. Nat Rev Gastroenterol Hepatol, 2022, 19( 3): 153- 168. DOI: 10.1038/s41575-021-00551-0. [36] WAGNER R, JAGHUTRIZ BA, GERST F, et al. Pancreatic steatosis associates with impaired insulin secretion in genetically predisposed individuals[J]. J Clin Endocrinol Metab, 2020, 105( 11): 3518- 3525. DOI: 10.1210/clinem/dgaa435. [37] LIU YT, KIMITA W, SHAMAITIJIANG X, et al. Intra-pancreatic fat is associated with continuous glucose monitoring metrics[J]. Diabetes Obes Metab, 2024, 26( 6): 2359- 2367. DOI: 10.1111/dom.15550. [38] KO J, SKUDDER-HILL L, TARRANT C, et al. Intra-pancreatic fat deposition as a modifier of the relationship between habitual dietary fat intake and insulin resistance[J]. Clin Nutr, 2021, 40( 7): 4730- 4737. DOI: 10.1016/j.clnu.2021.06.017. -

 本文二维码
本文二维码
计量
- 文章访问数: 9
- HTML全文浏览量: 1
- PDF下载量: 1
- 被引次数: 0

