
 PDF下载 ( 21847 KB)
PDF下载 ( 21847 KB)

不可切除肝细胞癌患者应用钇-90选择性体内放射疗法的效果分析
DOI: 10.12449/JCH260415
Efficacy of yttrium-90 selective internal radiotherapy in treatment of patients with unresectable hepatocellular carcinoma
-
摘要:
目的 评估不可切除肝细胞癌患者接受选择性体内放射疗法(SIRT)的疗效,为临床治疗方案选择提供参考。 方法 回顾性分析2023年5月1日—2024年9月1日在上海东方肝胆外科医院接受钇-90微球SIRT的73例不可切除肝细胞癌患者的临床资料。基于患者的肿瘤特征、体能状态、肝脏储备功能和实验室检查等结果,将SIRT治疗策略分为放射性切除组(n=9)、转化治疗组(n=47)和姑息治疗组(n=17)。根据术后随访结果,使用实体瘤局部反应评价标准对放射影像进行回顾和评价。符合正态分布的计量资料3组间比较采用单因素方差分析;计数资料3组间比较采用χ2检验,多因素分析采用Logistic回归模型。 结果 放射性切除组、转化治疗组和姑息治疗组的术后疗效差异有统计学意义(χ2=30.060,P<0.001);3组的疾病控制率分别为100.0%(9/9)、83.0%(39/47)和29.4%(5/17),组间差异有统计学意义(χ2=19.575,P<0.001);3组患者的客观缓解率差异亦有统计学意义(χ2=17.749,P<0.001)。多因素Logistic回归分析提示,肿瘤个数(比值比=0.085,95%置信区间:0.008~0.906,P=0.041)和联合靶向免疫治疗(比值比=18.808,95%置信区间:1.704~207.616,P=0.017)是肿瘤获得完全缓解的独立影响因素。 结论 肿瘤个数是影响SIRT疗效的独立危险因素,是不同治疗目标选择的重要依据, SIRT联合靶向免疫治疗可能取得更优疗效。 -
关键词:
- 肝细胞癌 /
- 钇-90选择性体内放射疗法 /
- 治疗结果
Abstract:Objective To investigate the efficacy of selective internal radiation therapy (SIRT) in patients with unresectable hepatocellular carcinoma, and to provide a reference for the selection of clinical treatment regimens. Methods A retrospective analysis was performed for the clinical data of 73 patients with unresectable hepatocellular carcinoma who received yttrium-90 microsphere SIRT in Eastern Hepatobiliary Surgery Hospital from May 1, 2023 to September 1, 2024. According to tumor characteristics, physical status, liver reserve function, laboratory tests, and SIRT treatment strategy, the patients were divided into radiation segmentectomy group with 9 patients, conversion therapy group with 47 patients, and palliative treatment group with 17 patients. Based on the results of postoperative follow-up, modified Response Evaluation Criteria in Solid Tumors were used to assess radiographic images. A one-way analysis of variance was used for comparison of normally distributed continuous data between three groups, and the chi-square test was used for comparison of categorical data between three groups; the Logistic regression model was used to perform the multivariate analysis. Results There was a significant difference in postoperative outcome between the radiation segmentectomy group, the conversion therapy group, and the palliative treatment group (χ2 =30.060, P<0.001). The disease control rate was 100.0% (9/9) in the radiation segmentectomy group, 83.0% (39/47) in the conversion therapy group, and 29.4% (5/17) in the palliative treatment group, with a significant difference between the three groups (χ2 =19.575, P<0.001), and there was also a significant difference in objective response rate between the three groups (χ2 =17.749, P<0.001). The multivariate Logistic regression analysis showed that the number of tumors (odds ratio [OR]=0.085, 95% confidence interval [CI]: 0.008 — 0.906, P=0.041) and combined targeted immunotherapy (OR=18.808, 95%CI: 1.704 — 207.616, P=0.017) were independent influencing factors for achieving complete response. Conclusion The number of tumors is an independent influencing factor for the efficacy of SIRT and is an important basis for selecting different treatment goals. SIRT combined with targeted immunotherapy may achieve better efficacy. -
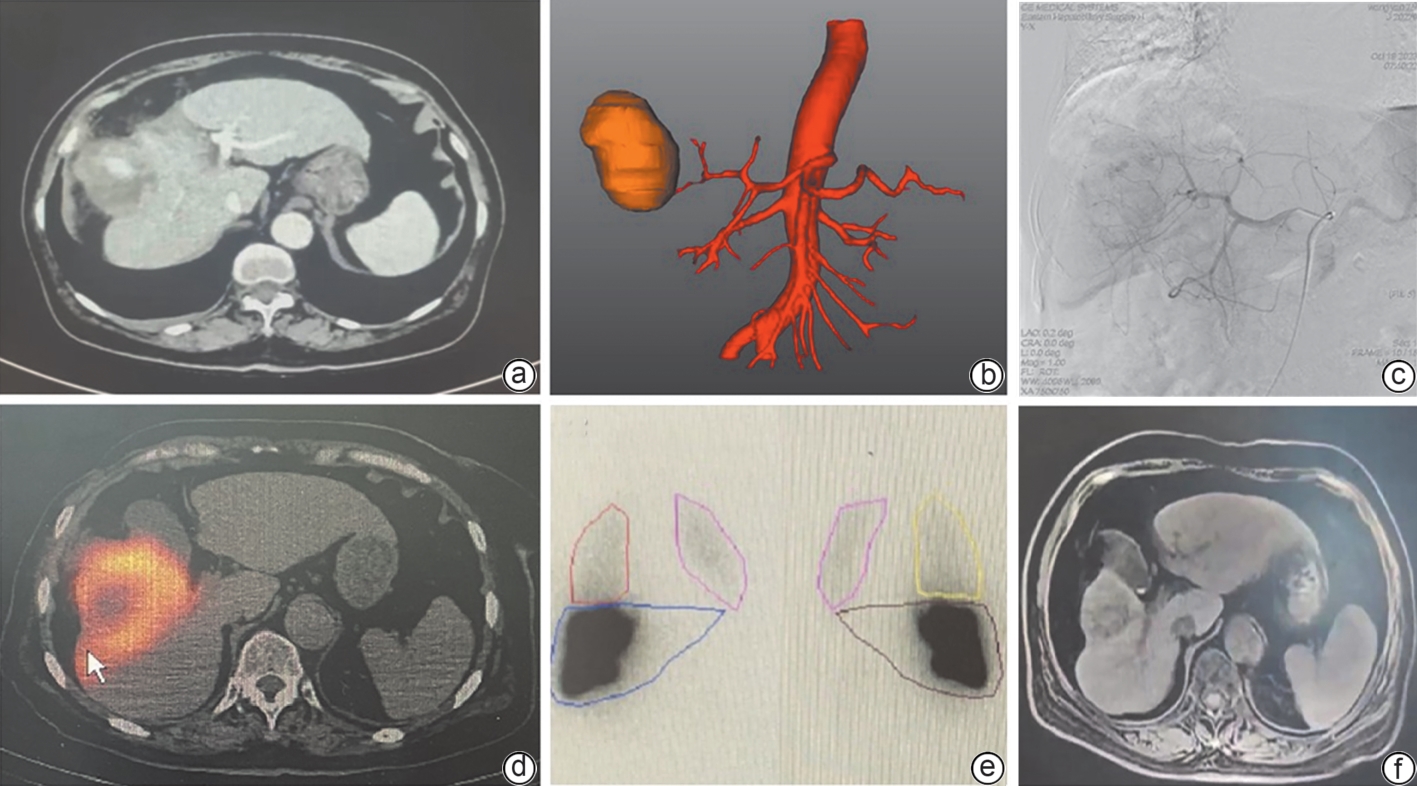
注: a,术前MRI,肝右叶占位,大小约5.6 cm×4.8 cm,患者年龄75岁,合并基础疾病不能耐受手术,诊疗目的为放射性肝段切除;b,术前三维成,计算肿瘤体积,肿瘤供血血管分布;c,血管造影/CBCT检查,评估肿瘤供血程度、选择治疗靶区和供血血管,靶血管注入锝-99m标记的大颗粒聚合白蛋白;d,评估正常肝/肿瘤灌注体积(箭头所示高亮区为锝-99m覆盖区);e,SPECT-CT扫描,评估肝外和肺分流比例;f,术后1个月MRI评估,肿瘤明显缩小,完全缓解。MRI,磁共振成像;CBCT,锥形束计算机体层成像;SPECT-CT,单光子发射计算机体层成像。
图 1 放射性肝段切除病例
Figure 1. Case of radiation segmentectomy
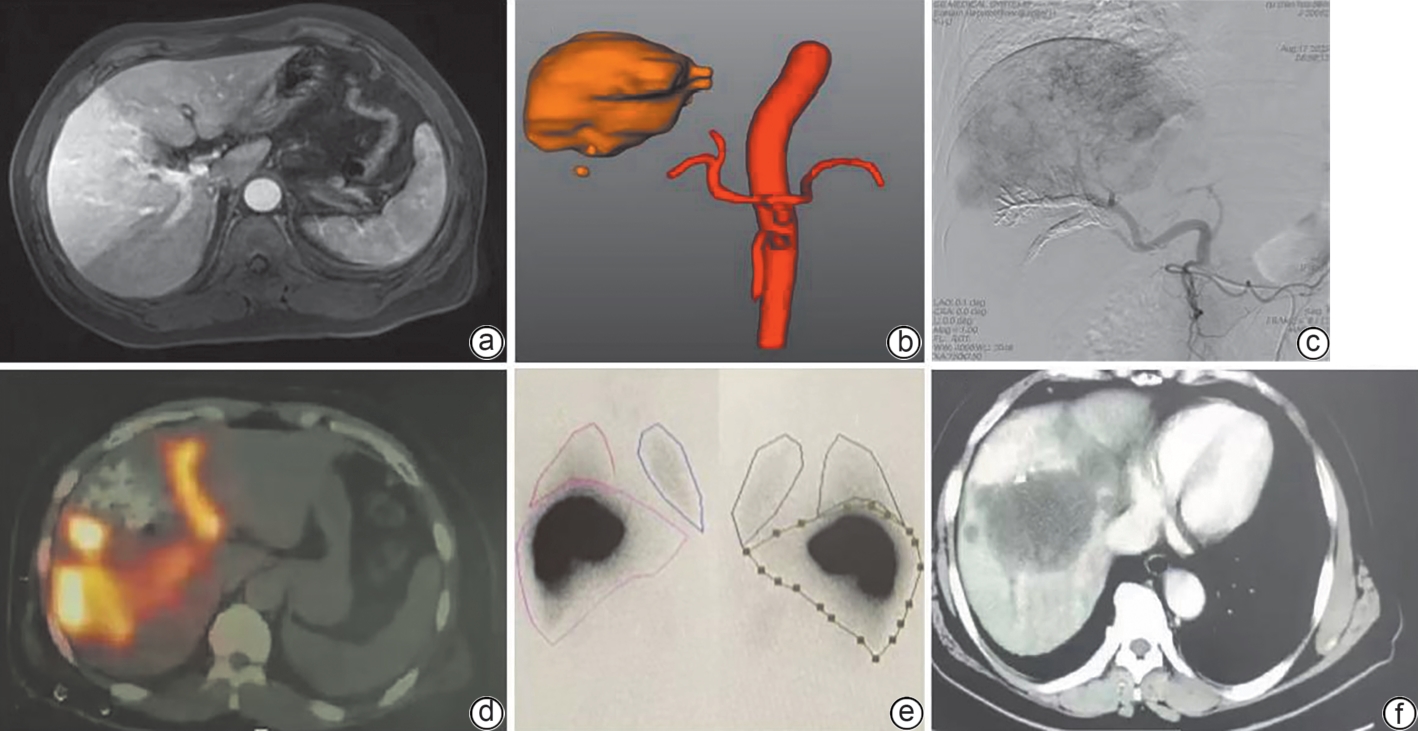
注: a,术前MRI,肝右叶近膈顶处肿瘤,大小约8.8 cm×7.3 cm,门静脉右前支受侵,病灶周围肝实质异常血流灌注,诊疗目的为转化治疗;b,术前三维成像,计算肿瘤体积,肿瘤供血血管分布;c,血管造影/CBCT检查,靶血管注入锝-99m标记的大颗粒聚合白蛋白;d,评估正常肝/肿瘤灌注体积;e,SPECT-CT扫描,评估肝外和肺分流比例;f,术后1月MRI评估,肿瘤明显缩小,成功转化并于3个月后手术切除。MRI,磁共振成像;CBCT,锥形束计算机体层成像;SPECT-CT,单光子发射计算机体层成像。
图 2 转化治疗病例
Figure 2. Case of transformation therapy
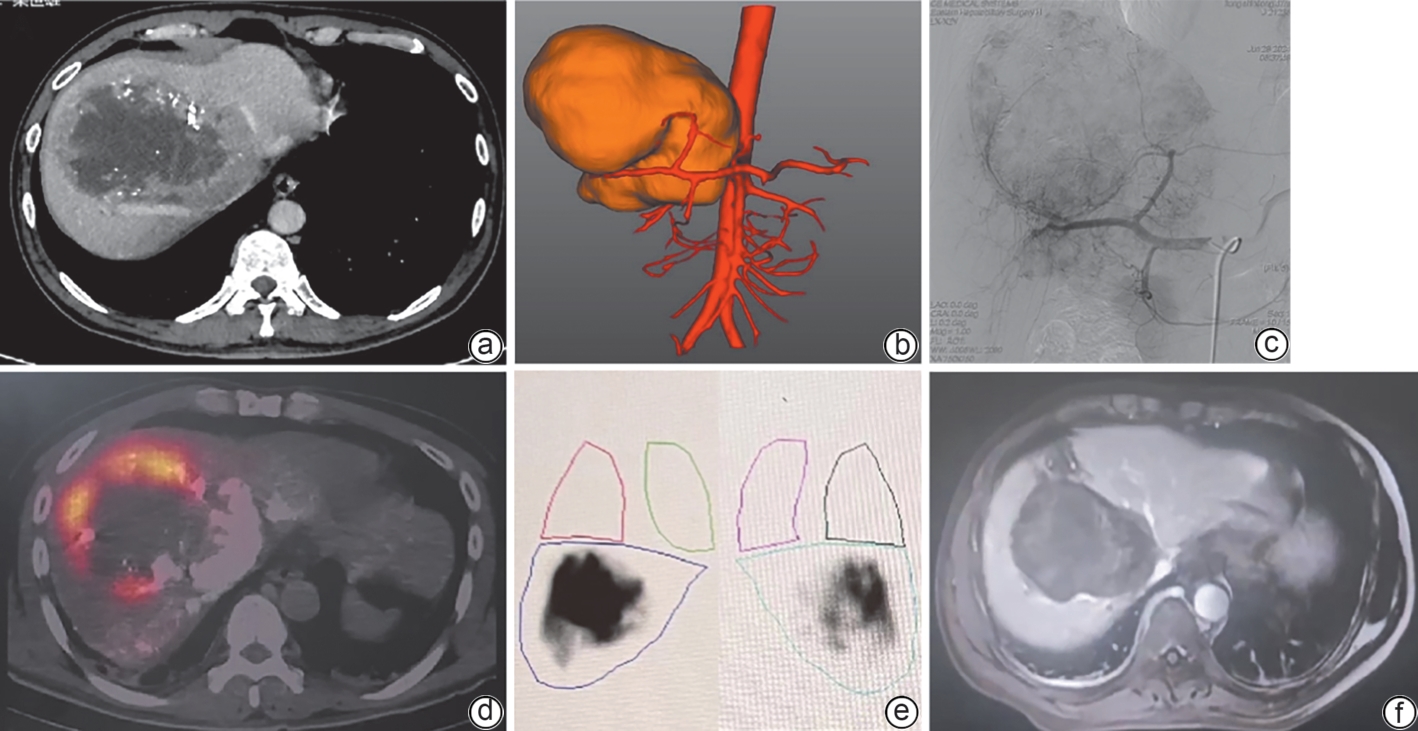
注: a,术前MRI,肝右叶巨块型肿瘤,伴有门静脉、肝静脉和下腔静脉肝段癌栓,难以转化,行SIRT减少肿瘤负荷,诊疗目的为姑息治疗;b,术前三维成像,计算肿瘤体积,肿瘤供血血管分布;c,血管造影/CBCT检查,靶血管注入锝-99m标记的大颗粒聚合白蛋白;d,评估正常肝/肿瘤灌注体积;e,SPECT-CT扫描,评估肝外和肺分流比例;f,术后1个月MRI评估,肿瘤活性区域明显缩小。MRI,磁共振成像;SIRT,选择性内放射治疗;CBCT,锥形束计算机体层成像;SPECT-CT,单光子发射计算机体层成像。
图 3 姑息治疗病例
Figure 3. Case of palliative treatment
表 1 3组患者临床资料的基线特征
Table 1. Baseline characteristics of clinical data of the three groups of patients
指标 放射性切除组(n=9) 转化治疗组(n=47) 姑息治疗组(n=17) 统计值 P值 年龄(岁) 66.8±12.1 57.0±13.9 57.7±14.7 F=1.911 0.156 性别[例(%)] χ2=3.483 0.146 男 7(77.8) 45(95.7) 16(94.1) 女 2(22.2) 2(4.3) 1(5.9) 乙型肝炎[例(%)] χ2=2.446 0.303 有 6(66.7) 33(70.2) 15(88.2) 无 3(33.3) 14(29.8) 2(11.8) Child-Pugh评分[例(%)] χ2=1.042 0.459 A 9(100.0) 40(85.1) 15(88.2) B 0(0.0) 7(14.9) 2(11.8) 肿瘤最大直径(cm) 5.4±1.6 10.0±3.9 8.8±3.8 F=6.105 <0.010 肿瘤大小[例(%)] χ2=6.747 0.021 <5 cm 4(44.4) 4(8.5) 3(17.6) ≥5 cm 5(55.6) 43(91.5) 14(82.4) 肿瘤个数[例(%)] χ2=8.923 0.012 单发 9(100.0) 30(63.8) 7(41.2) 多发 0(0.0) 17(36.2) 10(58.8) 甲胎蛋白[例(%)] χ2=1.414 0.449 <400 ng/mL 8(88.9) 32(68.1) 12(70.6) ≥400 ng/mL 1(11.1) 15(31.9) 5(29.4) 异常凝血酶原[例(%)] χ2=4.133 0.143 <40 mAU/mL 3(33.3) 13(27.7) 1(5.9) ≥40 mAU/mL 6(66.7) 34(72.3) 16(94.1) 门静脉癌栓[例(%)] χ2=4.607 0.090 有 2(22.2) 25(53.2) 12(70.6) 无 7(77.8) 22(46.8) 5(29.4) 靶向免疫治疗[例(%)] χ2=3.225 0.213 有 5(55.6) 31(66.0) 7(41.2) 无 4(44.4) 16(34.0) 10(58.8) 术前手术治疗[例(%)] χ2=8.245 0.014 有 2(22.2) 3(6.4) 6(35.3) 无 7(77.8) 44(93.6) 11(64.7) 术前TACE治疗[例(%)] χ2=6.276 0.028 有 1(11.1) 8(17.0) 8(47.1) 无 8(88.9) 39(83.0) 9(52.9) 钇-90剂量[例(%)] χ2=0.970 0.578 <3.0 Gbq 7(77.8) 29(61.7) 12(70.6) ≥3.0 Gbq 2(22.2) 18(38.3) 5(29.4) 肺分流[例(%)] χ2=0.642 0.702 <20% 7(77.8) 34(72.3) 14(82.4) ≥20% 2(22.2) 13(27.7) 3(17.6) 治疗后手术切除[例(%)] χ2=7.984 0.014 是 4(44.4) 8(17.0) 0(0.0) 否 5(55.6) 39(83.0) 17(100.0) 注:TACE,经导管动脉化疗栓塞术。
 下载: 导出CSV
下载: 导出CSV
表 2 3组患者SIRT的疗效评估
Table 2. Efficacy evaluation of SIRT in three groups of patients
疗效 放射性切除组(n=9) 转化治疗组(n=47) 姑息治疗组(n=17) χ2值 P值 术后疗效[例(%)] 30.060 <0.001 CR 6(66.7) 6(12.8) 0(0.0) PR 2(22.2) 11(23.4) 1(5.9) SD 1(11.1) 22(46.8) 4(23.5) PD 0(0.0) 8(17.0) 12(70.6) ORR[例(%)] 17.749 <0.001 CR+PR 8(88.9) 17(36.2) 1(5.9) SD+PD 1(11.1) 30(63.8) 16(94.1) DCR[例(%)] 19.575 <0.001 CR+PR+SD 9(100.0) 39(83.0) 5(29.4) PD 0(0.0) 8(17.0) 12(70.6) 注:SIRT,选择性内放射治疗;CR,完全缓解;PR,部分缓解;SD,疾病稳定;PD,疾病进展;ORR,客观缓解率;DCR,疾病控制率。
下载: 导出CSV
表 3 不可切除HCC患者接受SIRT治疗后完全缓解影响因素的Logistic回归分析
Table 3. Logistic regression analysis of predictors for complete response following SIRT in unresectable hepatocellular carcinoma
自变量 β值 SE Wald OR(95%CI) P值 肿瘤大小 -0.526 1.230 0.183 0.591(0.053~6.581) 0.669 门静脉癌栓 -1.077 0.793 1.843 0.341(0.072~1.613) 0.175 肿瘤个数 -2.465 1.208 4.167 0.085(0.008~0.906) 0.041 术前手术治疗 0.329 1.433 0.053 1.389(0.084~23.031) 0.818 术前TACE治疗 -1.465 1.347 1.183 0.231(0.016~3.239) 0.277 是否联合靶向免疫治疗 2.934 1.225 5.736 18.808(1.704~207.616) 0.017 注:HCC,肝细胞癌;SIRT,选择性内放射治疗;TACE,经导管动脉化疗栓塞术;OR,比值比;CI,置信区间。自变量赋值方式如下,肿瘤大小:<5 cm =0,≥5 cm=1;门静脉癌栓:无=0,有=1;肿瘤个数:单发=0,多发=1;术前手术治疗:无=0,有=1;术前TACE治疗:无=0,有=1;联合靶向免疫治疗:无=0,有=1。
下载: 导出CSV
-
[1] European Association for the Study of the Liver. EASL clinical practice guidelines on the management of hepatocellular carcinoma[J]. J Hepatol, 2025, 82( 2): 315- 374. DOI: 10.1016/j.jhep.2024.08.028. [2] SUNG H, FERLAY J, SIEGEL RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71( 3): 209- 249. DOI: 10.3322/caac.21660. [3] GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: A systematic analysis for the Global Burden of Disease Study 2015[J]. Lancet, 2016, 388( 10053): 1459- 1544. DOI: 10.1016/S0140-6736(16)31012-1. [4] WEBER SM, RIBERO D, O'REILLY EM, et al. Intrahepatic cholangiocarcinoma: Expert consensus statement[J]. HPB, 2015, 17( 8): 669- 680. DOI: 10.1111/hpb.12441. [5] LLOVET JM, DE BAERE T, KULIK L, et al. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma[J]. Nat Rev Gastroenterol Hepatol, 2021, 18( 5): 293- 313. DOI: 10.1038/s41575-020-00395-0. [6] LEWANDOWSKI RJ, GABR A, ABOUCHALEH N, et al. Radiation segmentectomy: Potential curative therapy for early hepatocellular carcinoma[J]. Radiology, 2018, 287( 3): 1050- 1058. DOI: 10.1148/radiol.2018171768. [7] LIU YY, LAI JX, LIU XX. Yttrium 90 microspheres in the management of hepatocellular carcinoma[J]. J Clin Hepatol, 2011, 27( 4): 348- 350. DOI: 10.3969/j.issn.1001-5256.2011.04.005.刘允怡, 赖俊雄, 刘晓欣. 钇90微球治疗原发性肝癌[J]. 临床肝胆病杂志, 2011, 27( 4): 348- 350. DOI: 10.3969/j.issn.1001-5256.2011.04.005. [8] RIAZ A, GATES VL, ATASSI B, et al. Radiation segmentectomy: A novel approach to increase safety and efficacy of radioembolization[J]. Int J Radiat Oncol Biol Phys, 2011, 79( 1): 163- 171. DOI: 10.1016/j.ijrobp.2009.10.062. [9] RHEE TK, OMARY RA, GATES V, et al. The effect of catheter-directed CT angiography on yttrium-90 radioembolization treatment of hepatocellular carcinoma[J]. J Vasc Interv Radiol, 2005, 16( 8): 1085- 1091. DOI: 10.1097/01.RVI.0000177063.92678.21. [10] KIM E, SHER A, ABBOUD G, et al. Radiation segmentectomy for curative intent of unresectable very early to early stage hepatocellular carcinoma(RASER): A single-centre, single-arm study[J]. Lancet Gastroenterol Hepatol, 2022, 7( 9): 843- 850. DOI: 10.1016/S2468-1253(22)00091-7. [11] TITANO J, NOOR A, KIM E. Transarterial chemoembolization and radioembolization across Barcelona clinic liver cancer stages[J]. Semin Intervent Radiol, 2017, 34( 2): 109- 115. DOI: 10.1055/s-0037-1602709. [12] LIVRAGHI T, SOLBIATI L, MELONI MF, et al. Treatment of focal liver tumors with percutaneous radio-frequency ablation: Complications encountered in a multicenter study[J]. Radiology, 2003, 226( 2): 441- 451. DOI: 10.1148/radiol.2262012198. [13] REIG M, FORNER A, RIMOLA J, et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update[J]. J Hepatol, 2022, 76( 3): 681- 693. DOI: 10.1016/j.jhep.2021.11.018. [14] SALEM R, JOHNSON GE, KIM E, et al. Yttrium-90 radioembolization for the treatment of solitary, unresectable HCC: The LEGACY study[J]. Hepatology, 2021, 74( 5): 2342- 2352. DOI: 10.1002/hep.31819. [15] SALEM R, PADIA SA, TOSKICH BB, et al. Radiation segmentectomy for early hepatocellular carcinoma is curative[J]. J Hepatol, 2025, 82( 6): 1125- 1132. DOI: 10.1016/j.jhep.2025.01.005. [16] ZHANG H, FU Y, TAN BB, et al. Clinical application and progress of yttrium 90 microsphere selective internal radiation therapy in primary hepatic cancer[J]. Chin J Dig Surg, 2024, 23( 2): 242- 247. DOI: 10.3760/cma.j.cn115610-20231208-00242.张辉, 付颖, 谭斌彬, 等. 钇⁃90微球选择性内放射治疗在原发性肝癌中的临床应用及进展[J]. 中华消化外科杂志, 2024, 23( 2): 242- 247. DOI: 10.3760/cma.j.cn115610-20231208-00242. [17] SANGRO B, SALEM R, KENNEDY A, et al. Radioembolization for hepatocellular carcinoma: A review of the evidence and treatment recommendations[J]. Am J Clin Oncol, 2011, 34( 4): 422- 431. DOI: 10.1097/COC.0b013e3181df0a50. [18] LEWANDOWSKI RJ, KULIK LM, RIAZ A, et al. A comparative analysis of transarterial downstaging for hepatocellular carcinoma: Chemoembolization versus radioembolization[J]. Am J Transplant, 2009, 9( 8): 1920- 1928. DOI: 10.1111/j.1600-6143.2009.02695.x. [19] BIEDERMAN DM, TITANO JJ, BISHAY VL, et al. Radiation segmentectomy versus TACE combined with microwave ablation for unresectable solitary hepatocellular carcinoma up to 3 cm: A propensity score matching study[J]. Radiology, 2017, 283( 3): 895- 905. DOI: 10.1148/radiol.2016160718. [20] BIEDERMAN DM, TITANO JJ, KORFF RA, et al. Radiation segmentectomy versus selective chemoembolization in the treatment of early-stage hepatocellular carcinoma[J]. J Vasc Interv Radiol, 2018, 29( 1): 30- 37.e2. DOI: 10.1016/j.jvir.2017.08.026. [21] SALEM R, LEWANDOWSKI RJ, MULCAHY MF, et al. Radioembolization for hepatocellular carcinoma using Yttrium-90 microspheres: A comprehensive report of long-term outcomes[J]. Gastroenterology, 2010, 138( 1): 52- 64. DOI: 10.1053/j.gastro.2009.09.006. [22] LENCIONI R, DELLA PINA C, BARTOLOZZI C. Percutaneous image-guided radiofrequency ablation in the therapeutic management of hepatocellular carcinoma[J]. Abdom Imaging, 2005, 30( 4): 401- 408. DOI: 10.1007/s00261-004-0254-8. [23] POMPILI M, SAVIANO A, DE MATTHAEIS N, et al. Long-term effectiveness of resection and radiofrequency ablation for single hepatocellular carcinoma ≤3 cm. Results of a multicenter Italian survey[J]. J Hepatol, 2013, 59( 1): 89- 97. DOI: 10.1016/j.jhep.2013.03.009. [24] LIVRAGHI T, MELONI F, DI STASI M, et al. Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: Is resection still the treatment of choice?[J]. Hepatology, 2008, 47( 1): 82- 89. DOI: 10.1002/hep.21933. [25] VOUCHE M, HABIB A, WARD TJ, et al. Unresectable solitary hepatocellular carcinoma not amenable to radiofrequency ablation: Multicenter radiology-pathology correlation and survival of radiation segmentectomy[J]. Hepatology, 2014, 60( 1): 192- 201. DOI: 10.1002/hep.27057. [26] SEROR O, NAULT JC, NAHON P, et al. Is segmental transarterial yttrium 90 radiation a curative option for solitary hepatocellular carcinoma ≤5 cm?[J]. Hepatology, 2015, 61( 1): 406- 407. DOI: 10.1002/hep.27174. [27] SALEM R, VOUCHE M, HABIB A, et al. Reply: To PMID 24691943[J]. Hepatology, 2015, 61( 1): 407. DOI: 10.1002/hep.27179. [28] CARDARELLI-LEITE L, CHUNG J, KLASS D, et al. Ablative transarterial radioembolization improves survival in patients with HCC and portal vein tumor thrombus[J]. Cardiovasc Intervent Radiol, 2020, 43( 3): 411- 422. DOI: 10.1007/s00270-019-02404-5. [29] ZHANG L, FENG XB, HUANG X, et al. Progress in the application of selective internal radiation therapy with yttrium‑90 microsph-eres in the downstaging and conversion treatment of hepatocellular carcinoma before liver transplantation[J]. Chin J Dig Surg, 2024, 23( 12): 1566- 1570. DOI: 10.3760/cma.j.cn115610-20241025-00467.张琳, 冯晓彬, 黄鑫, 等. 钇‑90微球选择性内放射治疗在肝癌降期转化移植中的应用进展[J]. 中华消化外科杂志, 2024, 23( 12): 1566- 1570. DOI: 10.3760/cma.j.cn115610-20241025-00467. [30] SALEM R, GORDON AC, MOULI S, et al. Y90 radioembolization significantly prolongs time to progression compared with chemoembolization in patients with hepatocellular carcinoma[J]. Gastroenterology, 2016, 151( 6): 1155- 1163.e2. DOI: 10.1053/j.gastro.2016.08.029. [31] GABR A, POLINENI P, MOULI SK, et al. Neoadjuvant radiation lobectomy as an alternative to portal vein embolization in hepatocellular carcinoma[J]. Semin Nucl Med, 2019, 49( 3): 197- 203. DOI: 10.1053/j.semnuclmed.2019.01.009. [32] GABA RC, LEWANDOWSKI RJ, KULIK LM, et al. Radiation lobectomy: Preliminary findings of hepatic volumetric response to lobar yttrium-90 radioembolization[J]. Ann Surg Oncol, 2009, 16( 6): 1587- 1596. DOI: 10.1245/s10434-009-0454-0. [33] TITANO J, VOUTSINAS N, KIM E. The role of radioembolization in bridging and downstaging hepatocellular carcinoma to curative therapy[J]. Semin Nucl Med, 2019, 49( 3): 189- 196. DOI: 10.1053/j.semnuclmed.2019.01.003. [34] GIRAUD J, CHALOPIN D, BLANC JF, et al. Hepatocellular carcinoma immune landscape and the potential of immunotherapies[J]. Front Immunol, 2021, 12: 655697. DOI: 10.3389/fimmu.2021.655697. [35] VALERY M, CERVANTES B, SAMAHA R, et al. Immunotherapy and hepatocellular cancer: Where are we now?[J]. Cancers, 2022, 14( 18): 4523. DOI: 10.3390/cancers14184523. [36] YIN PF, WU K, WANG HZ, et al. Advances in immunotherapy strategy for hepatocellular carcinoma and its application in perioperative period[J/OL]. Chin J Hepat Surg(Electronic Edition), 2026, 15( 1): 21- 27. DOI: 10.3877/cma.j.issn.2095-3232.2026.01.005.尹鹏飞, 吴堃, 王槐志, 等. 肝癌免疫治疗策略及其在围手术期中应用进展[J/OL]. 中华肝脏外科手术学电子杂志, 2026, 15( 1): 21- 27. DOI: 10.3877/cma.j.issn.2095-3232.2026.01.005. [37] SHEN X, ZHAO B. Efficacy of PD-1 or PD-L1 inhibitors and PD-L1 expression status in cancer: Meta-analysis[J]. BMJ, 2018, 362: k3529. DOI: 10.1136/bmj.k3529. -

 本文二维码
本文二维码
计量
- 文章访问数: 347
- HTML全文浏览量: 100
- PDF下载量: 78
- 被引次数: 0

