
 PDF下载 ( 9541 KB)
PDF下载 ( 9541 KB)

门静脉癌栓分型对肝细胞癌合并食管胃静脉曲张破裂出血患者再出血的影响
DOI: 10.12449/JCH260515
Impact of portal vein tumor thrombus classification on rebleeding in hepatocellular carcinoma patients with esophagogastric variceal bleeding
-
摘要:
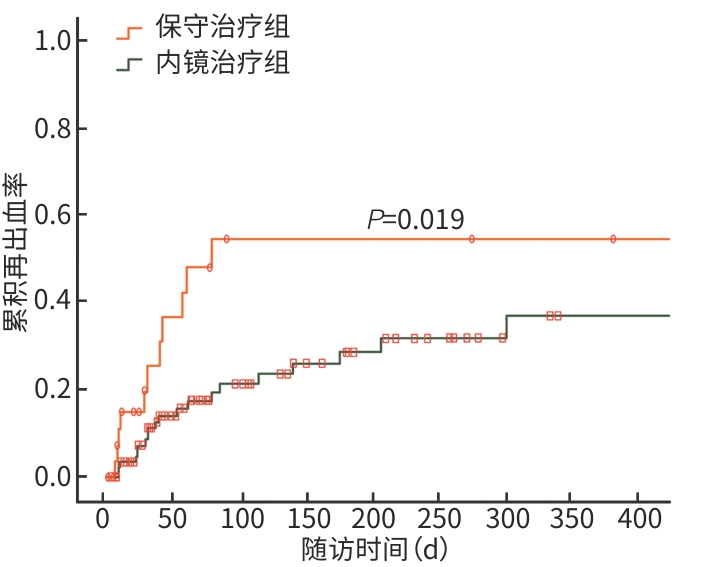
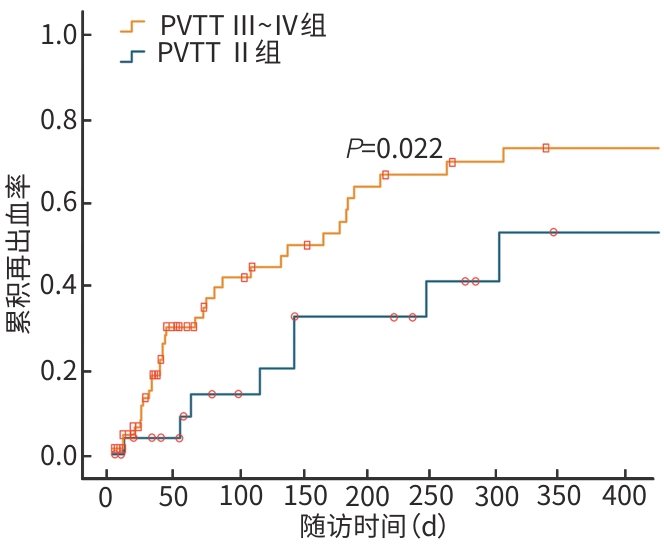
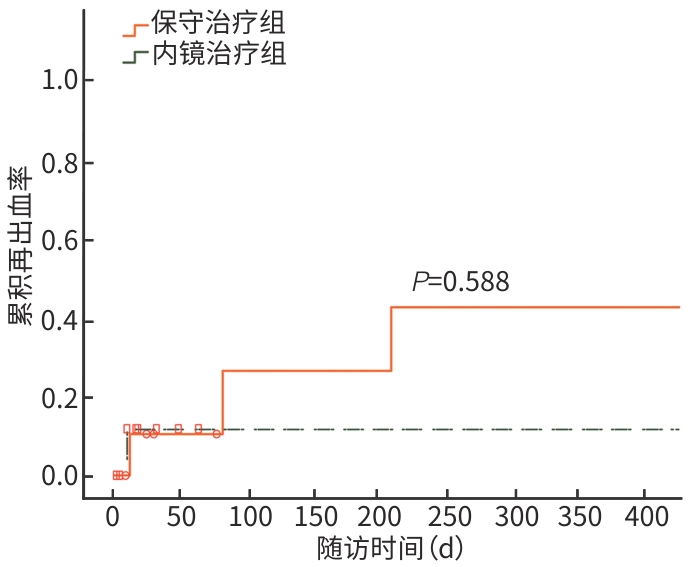
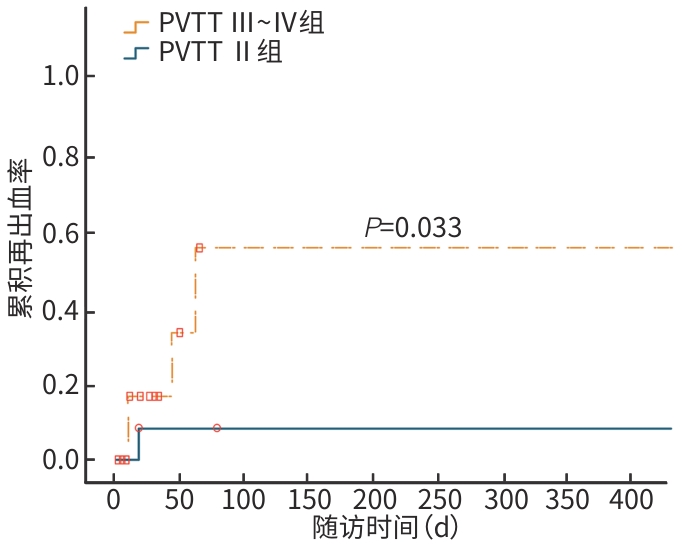
目的 通过观察肝细胞癌(HCC)合并不同分型门静脉癌栓(PVTT)及食管胃静脉曲张破裂出血(EGVB)患者的再出血情况,探讨PVTT分型对再出血的影响,为制订此类患者的合理治疗方案提供参考。 方法 回顾性纳入2020年7月—2025年1月因EGVB于首都医科大学附属北京地坛医院就诊的130例HCC合并PVTT患者为研究对象,根据是否接受内镜治疗将患者分为内镜治疗组(n=97)和保守治疗组(n=33)。收集患者人口学及临床资料,比较两组止血成功率及再出血情况。符合正态分布的计量资料组间比较采用成组t检验,不符合正态分布的计量资料组间比较采用Mann-Whitney U检验;计数资料组间比较采用χ2检验或Fisher’s精确检验。采用Kaplan-Meier法估计不同分型PVTT患者的再出血累积发生率。通过倾向性评分匹配(PSM)对内镜治疗组和保守治疗组进行配对,以均衡两组患者基线数据。采用Cox比例风险模型进行单因素和多因素分析,筛选再出血的独立危险因素。 结果 内镜治疗组患者的6个月内累积再出血率显著低于保守治疗组[35.1% vs 57.6%,风险比(HR)=0.480,95%置信区间(95%CI):0.272~0.851,P=0.019]。PVTT Ⅲ~Ⅳ组患者的6个月累积再出血率显著高于PVTT Ⅱ组(52.2% vs 37.5%,HR=1.744,95%CI:1.008~3.018, P=0.022)。PSM后,内镜治疗组和保守治疗组的再出血率差异无统计学意义(38.1% vs 14.3%,HR=1.500,95%CI:0.125~2.002,P=0.588),但PVTT Ⅲ~Ⅳ组患者的累积再出血率显著高于PVTT Ⅱ组(58.8% vs 12.5%,HR=1.561,95%CI:1.195~12.499,P=0.033)。多因素Cox回归分析显示,PVTT分型(HR=1.412,95%CI:0.998~1.997,P=0.049)、血小板计数(HR=1.006,95%CI:1.001~1.010,P=0.021)、C反应蛋白(HR=1.011,95%CI:1.001~1.021,P=0.026)和腹水(HR=1.803,95%CI:1.059~3.068,P=0.030)是再出血的独立危险因素。 结论 对于HCC合并PVTT及EGVB患者,内镜治疗可成功止血,但未能显著降低再出血率;PVTT分型影响再出血风险,其中PVTT Ⅲ~Ⅳ型患者再出血率较高。 Abstract:Objective To investigate the impact of portal vein tumor thrombus (PVTT) classification on rebleeding in hepatocellular carcinoma (HCC) patients with different PVTT subtypes and esophagogastric variceal bleeding (EGVB), and to provide a reference for formulating rational treatment regimens for such patients. Methods A retrospective study was performed for 130 patients with HCC and PVTT who were treated due to EGVB in Beijing Ditan Hospital, Capital Medical University, from July 2020 to January 2025, and according to whether endoscopic treatment was performed, the patients were divided into endoscopic treatment group with 97 patients and conservative treatment group with 33 patients. Demographic and clinical data were collected from all patients, and the two groups were compared in terms of hemostasis success rate and rebleeding rate. The independent-samples t test was used for comparison of normally distributed continuous data between groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between groups; the chi-square test or the Fisher’s exact test was used for comparison of categorical data between groups. The Kaplan-Meier method was used to estimate the cumulative incidence rate of rebleeding in patients with different subtypes of PVTT. Propensity score matching (PSM) was performed for the endoscopic treatment group and the conservative treatment group to balance the baseline data of the two groups. The Cox proportional hazards model was used to perform univariate and multivariate analyses and identify independent risk factors for rebleeding. Results The endoscopic treatment group had a significantly lower cumulative rebleeding rate within 6 months than the conservative treatment group (35.1% vs 57.6%, hazard ratio [HR]=0.480, 95% confidence interval [CI]: 0.272—0.851, P=0.019). The PVTT Ⅲ—Ⅳ group had a significantly higher cumulative rebleeding rate within 6 months than the PVTT Ⅱ group (52.2% vs 37.5%, HR=1.744, 95%CI: 1.008 — 3.018, P=0.022). After PSM, there was no significant difference in rebleeding rate between the endoscopic treatment group and the conservative treatment group (38.1% vs 14.3%,HR=1.500,95%CI:0.125 — 2.002, P=0.588), while the PVTT Ⅲ—Ⅳ group had a significantly higher cumulative rebleeding rate than the PVTT Ⅱ group (58.8% vs 12.5%,HR=1.561,95%CI:1.195 — 12.499,P=0.033). The multivariate Cox regression analysis showed that PVTT subtype (HR=1.412, 95%CI: 0.998 — 1.997, P=0.049), platelet count (HR=1.006, 95%CI: 1.001 — 1.010, P=0.021), C-reactive protein (HR=1.011, 95%CI: 1.001 — 1.021, P=0.026), and ascites (HR=1.803, 95%CI: 1.059 — 3.068, P=0.030) were independent risk factors for rebleeding. Conclusion For HCC patients with PVTT and EGVB, endoscopic treatment can successfully achieve hemostasis, while it fails to significantly reduce rebleeding rates. PVTT classification can affect the risk of rebleeding, and patients with PVTT types Ⅲ—Ⅳ have a relatively high rebleeding rate. -
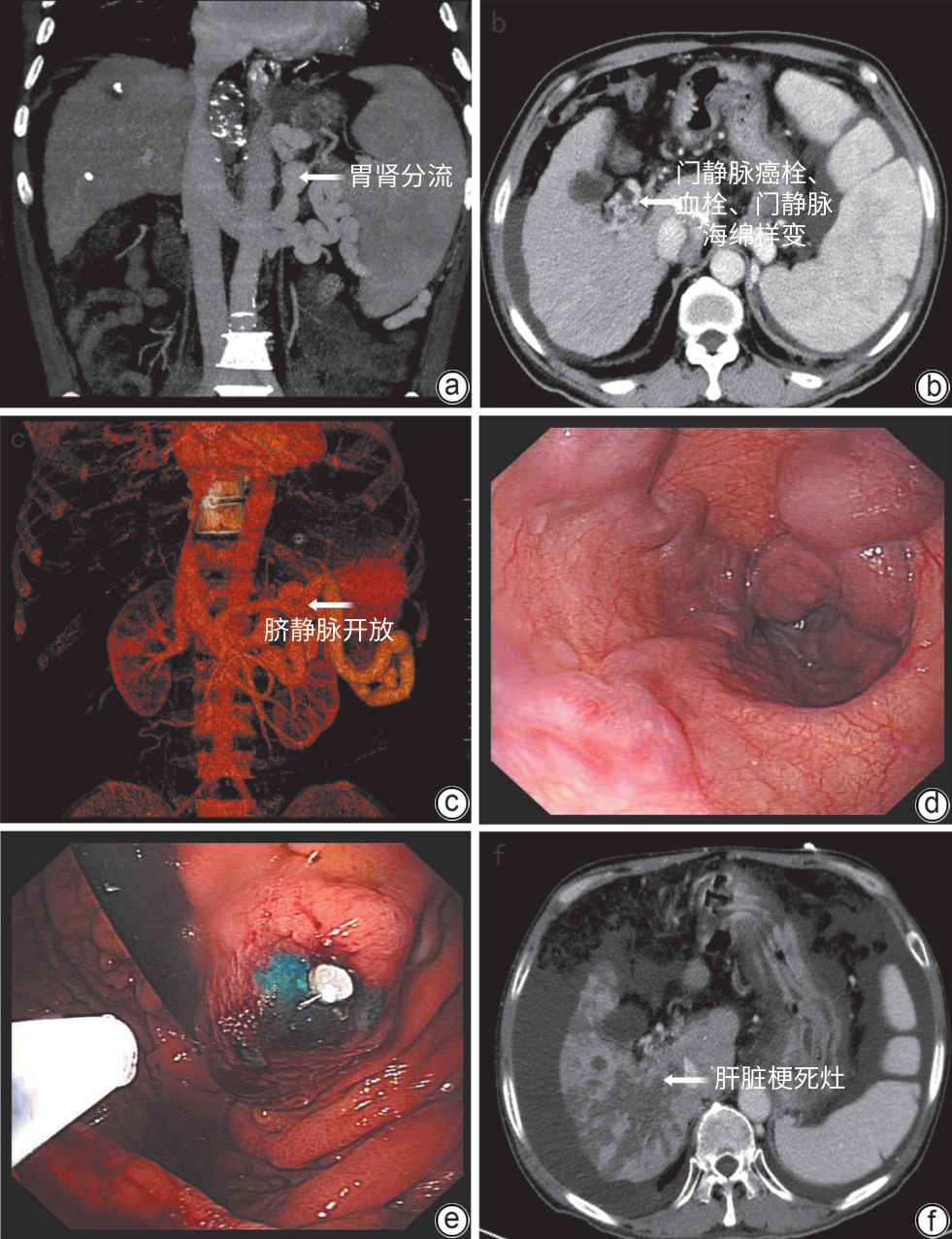
注: a~c,肝硬化合并HCC及PVTT患者出现门静脉海绵样变、门静脉系统多发血栓、胃肾分流道及脐静脉分流道开放;d、e,患者合并重度食管胃静脉曲张,反复出血,行内镜下治疗;f,内镜治疗后出现大面积肝梗死。HCC,肝细胞癌;PVTT,门静脉癌栓。
图 1 HCC合并PVTT患者内镜治疗后出现肝梗死
Figure 1. Hepatic infarction occurred in patients with HCC and PVTT after endoscopic treatment
注: HCC,肝细胞癌;PVTT,门静脉癌栓。
图 2 HCC合并PVTT内镜治疗组和保守治疗组的累积再出血率
Figure 2. The cumulative rebleeding rates of HCC with PVTT were compared between the endoscopic treatment group and the conservative treatment group
注: HCC,肝细胞癌;PVTT,门静脉癌栓。
图 3 HCC合并不同PVTT分型患者的累积再出血率
Figure 3. The cumulative rebleeding rates among HCC patients with various types of PVTT
注: PSM,倾向性评分匹配;HCC,肝细胞癌;PVTT,门静脉癌栓。
图 4 PSM后HCC合并PVTT内镜治疗组和保守治疗组累积再出血率
Figure 4. The cumulative rebleeding rates of HCC with PVTT were compared between the endoscopic treatment group and the conservative treatment group after PSM
注: PSM,倾向性评分匹配;HCC,肝细胞癌;PVTT,门静脉癌栓。
图 5 PSM后HCC合并不同PVTT分型患者的累积再出血率
Figure 5. The cumulative rebleeding rates among HCC patients with various types of PVTT after PSM
表 1 2组患者基线数据比较
Table 1. Baseline data of the patients
项目 内镜治疗组
(n=97)保守治疗组
(n=33)统计值 P值 匹配后内镜
治疗组(n=21)匹配后保守
治疗组(n=21)统计值 P值 年龄(岁) 57.7±9.8 57.2±10.5 t=0.263 0.609 56.6±9.1 57.6±7.2 t=0.462 0.501 性别[例(%)] χ2=2.012 0.241 0.606 男 86(88.7) 26(78.8) 18(85.7) 20(95.2) 女 11(11.3) 7(21.2) 3(14.3) 1(4.8) 病因控制[例(%)] χ2=0.208 0.685 χ2=0.404 0.525 是 41(42.3) 15(45.5) 12(57.1) 14(66.7) 否 56(57.7) 18(54.5) 9(42.9) 7(33.3) 肝病病因[例(%)] 0.893 0.875 乙型肝炎 50(51.5) 17(51.5) 11(52.4) 10(47.6) 丙型肝炎 12(12.4) 4(12.1) 2(9.5) 3(14.3) 酒精性肝病 8(8.2) 5(15.2) 2(9.5) 3(14.3) 自身免疫性肝病 10(10.3) 2(6.1) 2(9.5) 1(4.8) 胆汁淤积性肝病 3(3.1) 1(3.0) 0(0.0) 2(9.5) 其他 14(14.4) 4(12.1) 4(19.1) 2(9.5) 合并急性感染[例(%)] 0.738 1.000 是 9(9.3) 4(12.1) 1(4.8) 1(4.8) 否 88(90.7) 29(87.9) 20(95.2) 20(95.2) 肿瘤干预[例(%)] χ2=3.565 0.168 χ2=3.500 0.174 无 30(30.9) 6(18.1) 6(28.6) 10(47.6) 单一治疗 21(21.6) 12(36.4) 12(57.1) 6(28.6) 多种方法综合治疗 46(47.4) 15(45.5) 3(14.3) 5(23.8) 中性粒细胞(×109/L) 4.1(1.8~4.9) 4.8(2.9~4.1) Z=-2.926 0.003 3.3(1.8~5.6) 2.9(2.2~4.0) Z<0.001 1.000 血小板计数(×109/L) 99.2(59.5~119.0) 112.2(69.0~150.1) Z=-1.461 0.144 89.0(41.0~89.0) 90.0(48.0~90.0) Z=-0.655 0.513 血红蛋白(g/L) 90.4±24.2 88.9±26.4 t=0.357 0.552 85.7±23.5 84.9±22.7 t=0.252 0.615 ALT(U/L) 53.1(21.3~53.4) 84.2(31.7~114.7) Z=-2.600 0.009 40.0(26.8~85.0) 52.1(38.3~200.4) Z=-1.158 0.247 AST(U/L) 95.1(33.4~106.6) 159.5(51.4~177.8) Z=-3.140 0.002 87.6(47.6~107.9) 93.3(67.9~258.4) Z=-1.762 0.078 总胆红素(μmol/L) 36.0(16.4~36.3) 99.6(20.6~87.9) Z=-3.349 0.001 55.9(13.6~70.6) 24.7(20.8~34.5) Z=-0.906 0.365 白蛋白(g/L) 31.2(28.2~34.2) 31.6(27.3~35.4) Z=-1.115 0.909 30.3(25.4~35.3) 27.7(25.6~32.1) Z=-1.410 0.159 肌酐(μmol/L) 74.4(58.5~85.4) 86.2(61.5~87.2) Z=-0.930 0.352 65.2(60.6~82.1) 76.3(59.4~85.1) Z=-0.554 0.580 国际标准化比值 1.4(1.2~1.5) 1.6(1.3~1.6) Z=-1.896 0.058 1.5(1.3~1.6) 1.6(1.3~1.9) Z=-0.466 0.641 AFP(ng/mL) 254.5
(10.8~2 000.0)878.0
(142.0~2 000.0)Z=-0.638 0.523 1 115.0
(9.5~2 000.0)421.0
(128.0~2 000.0)Z=-0.073 0.501 C反应蛋白(mg/L) 26.2
(5.4~39.7)59.1
(14.8~77.5)Z=-3.469 0.001 12.3(4.8~40.6) 27.2(10.9~72.1) Z=-1.511 0.131 血钠(mmol/L) 133.3
(134.3~140.2)137.1
(133.9~141.1)Z=-0.202 0.840 140.2
(134.5~142.2)135.2
(131.8~138.2)Z=-1.763 0.078 合并肝硬化[例(%)] 95(97.9) 31(94.0) χ2=2.763 0.158 19(90.5) 19(90.5) χ2=0.000 1.000 合并腹水[例(%)] 68(70.1) 27(81.8) χ2=1.718 0.190 12(57.1) 16(76.2) χ2=1.714 0.190 合并肝性脑病[例(%)] 22(22.7) 17(51.5) χ2=9.749 0.002 6(28.6) 4(19.0) 0.719 首次出血[例(%)] χ2=1.315 0.252 0.469 是 55(56.7) 22(66.7) 6(28.6) 4(19.1) 否 42(43.3) 11(33.3) 15(71.4) 17(80.9)  下载: 导出CSV
下载: 导出CSV
表 1 (续)
Table 1. (continued)
项目 内镜治疗组
(n=97)保守治疗组
(n=33)统计值 P值 匹配后内镜
治疗组(n=21)匹配后保守
治疗组(n=21)统计值 P值 PVTT分型(程氏分型)
[例(%)]χ2=3.104 0.212 χ2=5.700 0.058 Ⅱ型 30(30.9) 10(30.3) 5(23.8) 3(14.3) Ⅲ型 10(10.3) 3(9.1) 4(19.1) 0(0.0) Ⅳ型 57(58.8) 20(60.6) 12(57.1) 18(85.7) 肿瘤BCLC分期
[例(%)]χ2=12.912 0.001 χ2=0.429 0.513 C期 74(76.3) 14(42.4) 13(61.9) 15(71.4) D期 23(23.7) 19(57.6) 8(38.1) 6(28.6) 蔡尔德-皮尤分级
[例(%)]χ2=9.417 0.009 χ2=0.963 0.618 A级 20(20.6) 5(15.1) 7(33.3) 6(28.6) B级 65(67.0) 16(48.5) 6(28.6) 9(42.8) C级 12(12.4) 12(36.4) 8(38.1) 6(28.6) 再出血时间(d) 55(23~168) 28(8~78) Z=-2.141 0.032 9(9~27) 42(9~60) Z=-1.361 0.174 注:PVTT,门静脉癌栓;BCLC,巴塞罗那肝癌临床分期;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;AFP,甲胎蛋白。
下载: 导出CSV
表 2 PVTT合并EGVB患者再出血的危险因素分析
Table 2. Risk factors of rebleeding in patients with PVTT and EGVB
变量 单因素分析 多因素分析 HR(95%CI) P值 HR(95%CI) P值 肿瘤干预 3.450(1.598~7.447) 0.002 0.700(0.485~1.010) 0.057 内镜治疗 2.350(1.123~4.918) 0.023 0.911(0.371~2.235) 0.838 血小板计数 1.006(1.001~1.011) 0.010 1.006(1.001~1.010) 0.021 ALT 1.008(1.003~1.012) 0.001 1.004(0.996~1.013) 0.272 AST 1.003(1.001~1.005) 0.003 0.998(0.994~1.013) 0.202 总胆红素 1.005(1.001~1.009) 0.009 1.000(0.994~1.007) 0.898 C反应蛋白 1.011(1.005~1.017) <0.001 1.011(1.001~1.021) 0.026 BCLC分期 0.237(0.115~0.486) <0.001 0.997(0.449~2.217) 0.995 PVTT分型 1.553(1.005~2.402) 0.048 1.412(0.998~1.997) 0.049 腹水 1.644(1.033~2.618) 0.036 1.803(1.059~3.068) 0.030 肝性脑病 2.165(1.256~3.732) 0.005 1.359(0.727~2.540) 0.337 蔡尔德-皮尤分级 1.206(1.032~1.410) 0.019 0.985(0.482~2.012) 0.966 注:PVTT,门静脉癌栓;EGVB,食管胃静脉曲张破裂出血;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;BCLC,巴塞罗那肝癌临床分期;HR,风险比;CI,置信区间。
下载: 导出CSV
-
[1] National Health Commission of the People’s Republic of China. Standard for diagnosis and treatment of primary liver cancer(2024 edition)[J]. J Clin Hepatol, 2024, 40( 5): 893- 918. DOI: 10.12449/JCH240508.中华人民共和国国家卫生健康委员会. 原发性肝癌诊疗指南(2024年版)[J]. 临床肝胆病杂志, 2024, 40( 5): 893- 918. DOI: 10.12449/JCH240508. [2] KUDO M, IZUMI N, ICHIDA T, et al. Report of the 19th follow-up survey of primary liver cancer in Japan[J]. Hepatol Res, 2016, 46( 5): 372- 390. DOI: 10.1111/hepr.12697. [3] MÄHRINGER-KUNZ A, STEINLE V, DÜBER C, et al. Extent of portal vein tumour thrombosis in patients with hepatocellular carcinoma: The more, the worse?[J]. Liver Int, 2019, 39( 2): 324- 331. DOI: 10.1111/liv.13988. [4] QIU GT, XIE KL, JIN ZX, et al. The multidisciplinary management of hepatocellular carcinoma with portal vein tumor thrombus[J]. Biosci Trends, 2021, 15( 3): 148- 154. DOI: 10.5582/bst.2021.01173. [5] HAN ML, CHEN CC, KUO SH, et al. Predictors of in-hospital mortality after acute variceal bleeding in patients with hepatocellular carcinoma and concurrent main portal vein thrombosis[J]. J Gastroenterol Hepatol, 2014, 29( 2): 344- 351. DOI: 10.1111/jgh.12341. [6] MA JL, HE LL, LI P, et al. Clinical features and outcomes of repeated endoscopic therapy for esophagogastric variceal hemorrhage in cirrhotic patients: Ten-year real-world analysis[J]. Gastroenterol Res Pract, 2020, 2020: 5747563. DOI: 10.1155/2020/5747563. [7] CHENG SQ, WU MC, CHEN H, et al. A study on imagination features of tumor thrombi in the portal vein of primary liver cancer[J]. Chin J Gen Surg, 2004, 19( 4): 200- 201. DOI: 10.3760/j.issn: 1007-631X.2004.04.002.程树群, 吴孟超, 陈汉, 等. 肝癌门静脉癌栓分型的影像学意义[J]. 中华普通外科杂志, 2004, 19( 4): 200- 201. DOI: 10.3760/j.issn: 1007-631X.2004.04.002. [8] Chinese Society of Hepatology, Chinese Society of Gastroenterology, Chinese Society of Digestive Endoscopology of Chinese Medical Association. Guidelines on the management of esophagogastric variceal bleeding in cirrhotic portal hypertension[J]. J Clin Hepatol, 2023, 39( 3): 527- 538. DOI: 10.3760/cmaj.cn501113-20220824-00436.中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会消化内镜学分会. 肝硬化门静脉高压食管胃静脉曲张出血的防治指南[J]. 临床肝胆病杂志, 2023, 39( 3): 527- 538. DOI: 10.3760/cmaj.cn501113-20220824-00436. [9] LEUNG JH, WANG SY, LEUNG HWC, et al. Comparative efficacy and safety of multimodality treatment for advanced hepatocellular carcinoma with portal vein tumor thrombus: Patient-level network meta-analysis[J]. Front Oncol, 2024, 14: 1344798. DOI: 10.3389/fonc.2024.1344798. [10] WANG JP, WANG RM, ZHU XG. Three cases of radiotherapy for primary liver cancer with portal vein tumor thrombosis[J/CD]. Chin J Liver Dis(Electronic Version), 2025, 17( 3): 63- 67. DOI: 10.3969/j.issn.1674-7380.2025.03.010.王菊萍, 王润梅, 朱向高. 原发性肝癌合并门静脉癌栓放射治疗3例[J/CD]. 中国肝脏病杂志(电子版), 2025, 17( 3): 63- 67. DOI: 10.3969/j.issn.1674-7380.2025.03.010. [11] MU Y, GE NJ, WANG XH, et al. The efficacy CalliSpheres drug-eluding beads transcatheter arterial chemoembolization combined with hepatic artery infusion chemotherapy in the treatment of hepatocellular carcinoma complicated with portal vein tumor thrombus[J]. Clin J Med Offic, 2025, 53( 10): 1009- 1013, 1018. DOI: 10.16680/j.1671-3826.2025.10.04.穆亚, 葛乃建, 王鑫昊, 等. Callispheres可载药微球经导管动脉化疗栓塞联合肝动脉灌注化疗治疗肝细胞癌合并门静脉癌栓疗效[J]. 临床军医杂志, 2025, 53( 10): 1009- 1013, 1018. DOI: 10.16680/j.1671-3826.2025.10.04. [12] ABDELHAMED W, SHOUSHA H, EL-KASSAS M. Portal vein tumor thrombosis in hepatocellular carcinoma patients: Is it the end?[J]. Liver Res, 2024, 8( 3): 141- 151. DOI: 10.1016/j.livres.2024.09.002. [13] LIU W, XU LX, XU F, et al. A retrospective analysis of the efficacy of endoscopic variceal ligation versus endoscopic tissue adhesive injection in the treatment of esophagogastric variceal bleeding[J]. Dig Dis, 2023, 41( 3): 468- 475. DOI: 10.1159/000528519. [14] HU YH, ZHOU M, LIU DL, et al. Risk factors for rebleeding after endoscopic injection of cyanoacrylate glue for gastric varices: A systematic review and meta-analysis[J]. Dig Dis Sci, 2024, 69( 8): 2890- 2903. DOI: 10.1007/s10620-024-08482-x. [15] HUANG XQ, ZOU DT, WANG HS, et al. Gastric variceal obstruction improves the efficacy of endoscopic management of esophageal variceal bleeding in GOV type I[J]. Endosc Int Open, 2024, 12( 8): E940- E946. DOI: 10.1055/a-2360-4490. [16] BRUSILOVSKAYA K, HOFER BS, SIMBRUNNER B, et al. Platelet function decreases with increasing severity of liver cirrhosis and portal hypertension-a prospective study[J]. Thromb Haemost, 2023, 123( 12): 1140- 1150. DOI: 10.1055/s-0043-1771187. [17] LIU H, CHEN P, JIANG B, et al. The value of platelet parameters and related scoring system in predicting esophageal varices and collateral veins in patients with liver cirrhosis[J]. J Clin Lab Anal, 2021, 35( 3): e23694. DOI: 10.1002/jcla.23694. [18] LI BB, LI Y, PENG Y, et al. Visual prediction models for predicting rebleeding events after the first esophageal variceal ligation[J]. Surg Endosc, 2025, 39( 6): 3576- 3586. DOI: 10.1007/s00464-025-11714-4. [19] TONON M, PIANO S. Cirrhosis and portal hypertension: How do we deal with ascites and its consequences[J]. Med Clin North Am, 2023, 107( 3): 505- 516. DOI: 10.1016/j.mcna.2022.12.004. [20] de FRANCHIS R, BOSCH J, GARCIA-TSAO G, et al. Baveno VII-Renewing consensus in portal hypertension[J]. J Hepatol, 2022, 76( 4): 959- 974. DOI: 10.1016/j.jhep.2021.12.022. [21] GIRI S, SUNDARAM S, JEARTH V, et al. Predictors of early bleeding after endoscopic variceal ligation for esophageal varices: A systematic review and meta-analysis[J]. Clin Exp Hepatol, 2022, 8( 4): 267- 277. DOI: 10.5114/ceh.2022.123096. [22] ZHAN JY, CHEN J, YU JZ, et al. Prognostic model for esophagogastric variceal rebleeding after endoscopic treatment in liver cirrhosis: A Chinese multicenter study[J]. World J Gastroenterol, 2025, 31( 2): 100234. DOI: 10.3748/wjg.v31.i2.100234. [23] CAZZANIGA M, DIONIGI E, GOBBO G, et al. The systemic inflammatory response syndrome in cirrhotic patients: Relationship with their in-hospital outcome[J]. J Hepatol, 2009, 51( 3): 475- 482. DOI: 10.1016/j.jhep.2009.04.017. [24] ICHIKAWA T, MACHIDA N, KANEKO H, et al. C-reactive protein can predict patients with cirrhosis at a high risk of early mortality after acute esophageal variceal bleeding[J]. Intern Med, 2019, 58( 4): 487- 495. DOI: 10.2169/internalmedicine.1447-18. [25] MA JL, HE LL, LI P, et al. Prognosis of endotherapy versus splenectomy and devascularization for variceal bleeding in patients with hepatitis B-related cirrhosis[J]. Surg Endosc, 2021, 35( 6): 2620- 2628. DOI: 10.1007/s00464-020-07682-6. [26] LV Y, QI XS, HE CY, et al. Covered TIPS versus endoscopic band ligation plus propranolol for the prevention of variceal rebleeding in cirrhotic patients with portal vein thrombosis: A randomised controlled trial[J]. Gut, 2018, 67( 12): 2156- 2168. DOI: 10.1136/gutjnl-2017-314634. [27] LIU J, LADBURY C, AMINI A, et al. Combination of yttrium-90 radioembolization with stereotactic body radiation therapy in the treatment of portal vein tumor thrombosis[J]. Radiat Oncol J, 2021, 39( 2): 113- 121. DOI: 10.3857/roj.2021.00213. [28] LI YY, WANG DC, ZHANG FT, et al. Hepatic arterial infusion chemotherapy combined with lenvatinib and toripalimab for large hepatocellular carcinoma(> 10 cm) with major portal vein tumor thrombosis: A multicenter propensity score matching analysis[J]. Front Immunol, 2025, 16: 1638173. DOI: 10.3389/fimmu.2025.1638173. -

 本文二维码
本文二维码
计量
- 文章访问数: 202
- HTML全文浏览量: 56
- PDF下载量: 81
- 被引次数: 0

