
 PDF下载 ( 8151 KB)
PDF下载 ( 8151 KB)

不同中医证型原发性肝癌的临床特征及多模态定量影像学特征分析
DOI: 10.12449/JCH260514
Clinical features and multimodal quantitative radiological features of primary liver cancer patients with different traditional Chinese medicine syndrome types
-
摘要:
目的 分析原发性肝癌(PLC)中医证型与临床特征及计算机体层成像(CT)、磁共振成像(MRI)多模态定量影像特征之间的关联,为中医辨证的客观化与精准诊疗提供参考依据。 方法 回顾性分析2020年3月—2025年6月在湖南中医药大学第一附属医院确诊为PLC的312例患者临床资料,分为肝气郁结证(n=40)、肝郁脾虚证(n=109)、气滞血瘀证(n=62)、湿热毒蕴证(n=81)及肝肾阴虚证(n=20)。比较不同中医证型间临床特征及多模态影像特征的差异。正态分布的计量资料多组间比较采用单因素方差分析,进一步两两比较采用LSD-t检验;非正态分布的计量资料多组间比较采用Kruskal-Wallis H秩和检验,进一步两两比较采用Dunn检验。计数资料组间比较采用χ2检验,进一步两两比较采用Bonferroni校正法。 结果 中国肝癌临床分期、蔡尔德-皮尤分级、丙氨酸氨基转移酶、天冬氨酸氨基转移酶、白蛋白、直接胆红素、总胆红素、凝血酶原时间、中性粒细胞和白蛋白-胆红素评分在不同中医证型间的差异均有统计学意义(P值均<0.05);肝气郁结证患者蔡尔德-皮尤分级以A级(75.00%)为主;肝气郁结证(60.00%)和气滞血瘀证(59.68%)多见于中国肝癌临床分期Ⅰ期,而湿热毒蕴证(27.16%)和肝肾阴虚证(30.00%)在Ⅳ期的分布比例显著高于肝气郁结证(2.50%)(P值均<0.05)。影像学结果显示,肿瘤数目、腹水、静脉癌栓、肿瘤最长径、肝内转移及肝门区、腹膜后淋巴结转移在不同证型间的差异均有统计学意义(P值均<0.05);与肝气郁结证相比,肝郁脾虚证和肝肾阴虚证更易发生肝内转移,肝郁脾虚证、湿热毒蕴证及肝肾阴虚证更易发生肝门区、腹膜后淋巴结转移,肝肾阴虚证更易出现肿瘤多发,且肝郁脾虚证和湿热毒蕴证更易出现腹水(P值均<0.05)。与气滞血瘀证相比,肝郁脾虚证肿瘤最长径更长且静脉癌栓占比更高(P值均<0.05)。此外,在184例具有MRI弥散加权成像序列的患者中,湿热毒蕴证和气滞血瘀证的表观扩散系数及相对表观扩散系数显著高于肝气郁结证(P值均<0.05)。 结论 不同中医证型的PLC患者在CT与MRI影像特征及临床表现方面存在显著差异,其中肝郁脾虚证、湿热毒蕴证及肝肾阴虚证更易呈现肿瘤进展性影像学特征,湿热毒蕴证与气滞血瘀证表观扩散系数较高,为PLC中医辨证分型提供了客观依据。 Abstract:Objective To investigate the association of the traditional Chinese medicine (TCM) syndrome types of primary liver cancer (PLC) with clinical features and multimodal quantitative radiological features on computed tomography (CT) and magnetic resonance imaging (MRI), and to provide a reference for the objectification of TCM syndrome differentiation and precise diagnosis and treatment. Methods A retrospective analysis was performed for the clinical data of 312 patients who were diagnosed with PLC in The First Affiliated Hospital of Hunan University of Chinese Medicine from March 2020 to June 2025, and according to the TCM syndrome type, they were divided into stagnation of liver Qi group with 40 patients, stagnation of liver Qi and spleen deficiency group with 109 patients, Qi stagnation and blood stasis group with 62 patients, dampness-heat toxin amassment group with 81 patients, and liver-kidney Yin deficiency group with 20 patients. Clinical features and multimodal quantitative radiological features were compared between the patients with different TCM syndrome types. A one-way analysis of variance was used for comparison of normally distributed continuous data between multiple groups, and the least significant difference t-test was used for further comparison between two groups; the Kruskal-Wallis H test was used for comparison of non-normally distributed continuous data between multiple groups, and the Dunn’s multiple test was used for further comparison between two groups; the chi-square test was used for comparison of categorical data between groups, and the Bonferroni method was used for further comparison between two groups. Results There were significant differences between the patients with different TCM syndrome types in China liver cancer staging (CNLC), Child-Pugh class, alanine aminotransferase, aspartate aminotransferase, albumin, direct bilirubin, total bilirubin, prothrombin time, neutrophil, and albumin-bilirubin score (all P<0.05). In the stagnation of liver Qi group, the patients with Child-Pugh class A accounted for 75.00%; among the patients with CNLC stage I PLC, the patients with stagnation of liver Qi accounted for 60.00%, and those with Qi stagnation and blood stasis syndrome accounted for 59.68%, while among the patients with CNLC stage IV PLC, the distribution proportion of dampness-heat toxin amassment (27.16%) and liver-kidney Yin deficiency (30.00%) was significantly higher than that of stagnation of liver Qi (2.50%) (all P<0.05). Radiological examination showed that there were significant differences between the patients with different TCM syndrome types in the number of tumors, ascites, venous tumor thrombus, maximum tumor diameter, intrahepatic metastasis, and lymph node metastasis in the hepatic hilar and retroperitoneal regions (all P<0.05). Compared with the patients with stagnation of liver Qi, the patients with liver depression and spleen deficiency or liver-kidney Yin deficiency were more likely to develop intrahepatic metastasis; the patients with liver depression and spleen deficiency, dampness-heat toxin amassment, or liver-kidney Yin deficiency were more likely to develop lymph node metastasis in the hepatic hilar and retroperitoneal regions; the patients with liver-kidney Yin deficiency were more likely to experience multiple tumors; the patients with liver depression and spleen deficiency or dampness-heat toxin amassment were more likely to develop ascites (all P<0.05). Compared with the patients with Qi stagnation and blood stasis syndrome, the patients with liver depression and spleen deficiency had a significantly longer maximum tumor diameter and a significantly higher proportion of patients with venous tumor thrombus (both P<0.05). Furthermore, among the 184 patients with MRI diffusion-weighted imaging sequences, the patients with dampness-heat toxin amassment or Qi stagnation and blood stasis syndrome had significantly higher ADC values and relative ADC values than those with stagnation of liver Qi (all P<0.05). Conclusion There are significant differences in CT/MRI radiological features and clinical features between PLC patients with different TCM syndrome types, among whom the patients with liver depression and spleen deficiency, dampness-heat toxin amassment, and liver-kidney Yin deficiency tend to exhibit progressive radiological features, and those with dampness-heat toxin amassment or Qi stagnation and blood stasis syndrome tend to have higher ADC values. These findings provide an objective basis for TCM syndrome differentiation in PLC. -
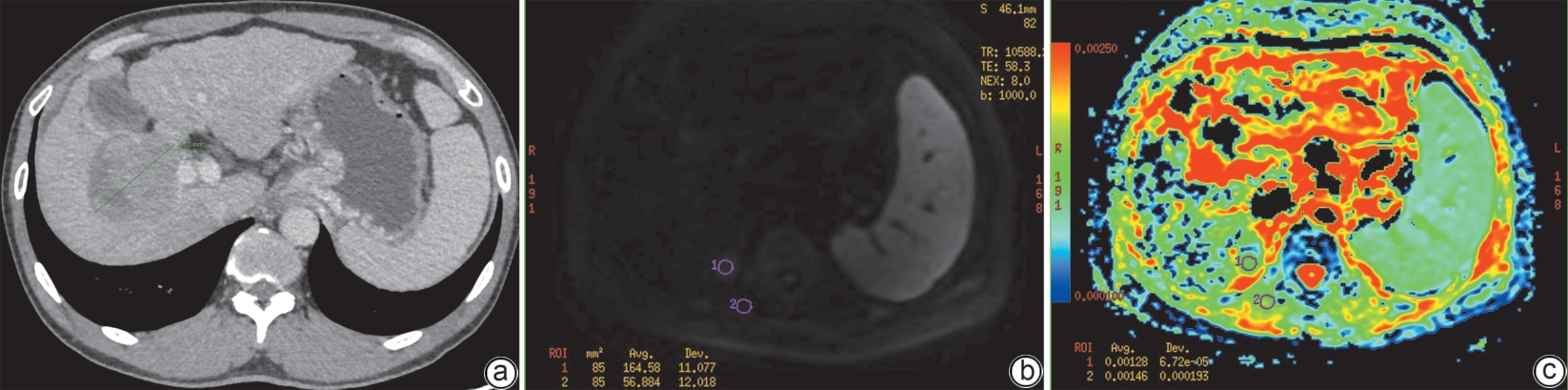
注: a,CT静脉期,测量肿瘤最长径;b,DWI图,勾画感兴趣区;c,ADC图。CT,计算机体层成像;DWI,弥散加权成像;ADC,表观扩散系数。
图 1 定量特征提取示意图
Figure 1. Schematic diagram of quantitative feature extraction
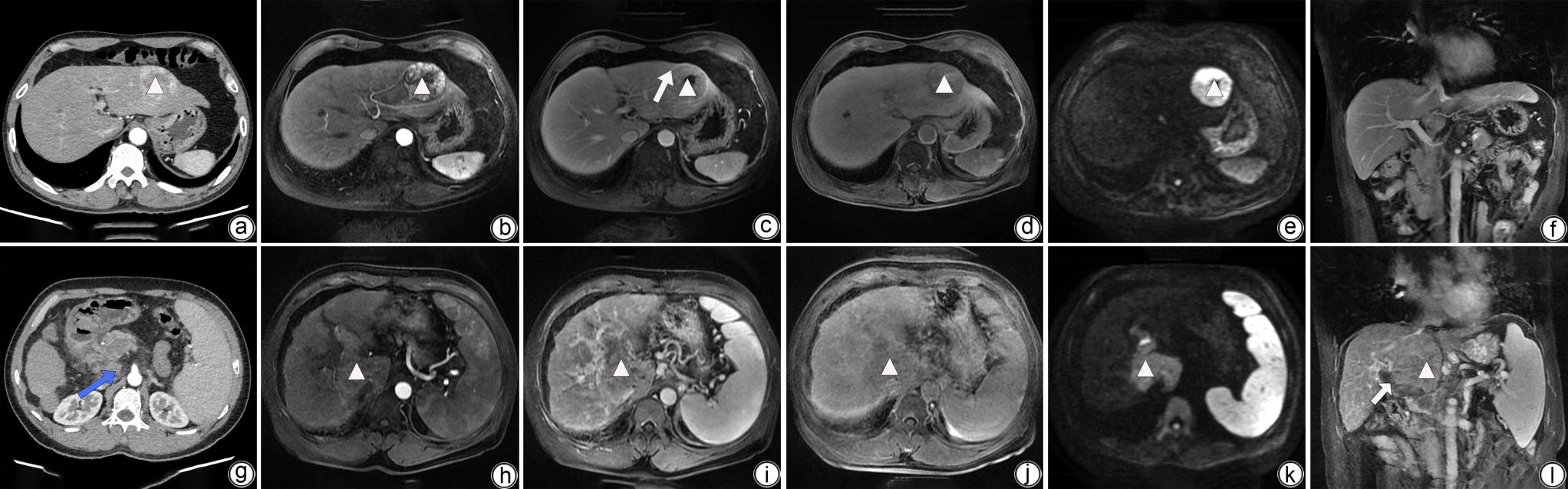
注: a、b、g、h,动脉期;c、i,静脉期;d、j,肝胆期;e、k,弥散加权成像;f、l,冠状位。a~f,男性患者,肝气郁结证,肝左外叶结节(白色三角形),完全假包膜(长白色箭头),无腹水、静脉癌栓、肝内转移、肝门区及腹膜后淋巴结转移;g~l,男性患者,肝郁脾虚证,肝尾状叶结节(白色三角形),静脉癌栓(短白色箭头),腹膜后淋巴结转移(蓝色箭头)。CT,计算机体层成像;MRI,磁共振成像。
图 2 不同中医证型患者CT、MRI表现
Figure 2. CT and MRI manifestations of patients with different TCM syndromes
表 1 不同中医证型基线特征比较
Table 1. Comparison of baseline characteristics among different TCM syndrome types
基线特征 肝气郁结证
(n=40)肝郁脾虚证
(n=109)气滞血瘀证
(n=62)湿热毒蕴证
(n=81)肝肾阴虚证
(n=20)统计值 P值 男[例(%)] 29(72.50) 91(83.49) 50(80.65) 68(83.95) 15(75.00) χ2=3.257 0.516 年龄(岁) 57.13±12.46 62.12±11.18 60.71±11.46 60.35±12.33 63.60±8.17 F=1.691 0.152 Child-Pugh分级
[例(%)]χ2=31.569 <0.001 A 30(75.00) 41(37.61)1) 24(38.71)1) 26(32.10)1) 5(25.00)1) B 9(22.50) 45(41.28) 31(50.00) 35(43.21) 8(40.00) C 1(2.50) 23(21.10) 7(11.29) 20(24.69)1) 7(35.00)1)2) CNLC分期
[例(%)]χ2=34.304 <0.001 Ⅰ 24(60.00) 37(33.94)1)2) 37(59.68) 38(46.91) 3(15.00)1)2) Ⅱ 9(22.50) 19(17.43) 7(11.29) 9(11.11) 6(30.00) Ⅲ 6(15.00) 30(27.52) 10(16.13) 12(14.81) 5(25.00) Ⅳ 1(2.50) 23(21.10) 8(12.90) 22(27.16)1) 6(30.00)1) AFP[例(%)] χ2=6.099 0.192 ≥400 ug/L 13(32.50) 45(41.28) 17(27.42) 20(24.69) 7(35.00) <400 ug/L 27(67.50) 64(58.72) 45(72.58) 61(75.31) 13(65.00) AST(U/L) 41.82
(33.64~50.00)116.95
(77.50~156.40)1)68.61
(50.79~86.43)76.20
(63.54~88.86)1)132.49
(56.08~208.89)1)H=31.227 <0.001 ALT(U/L) 30.96
(25.34~36.57)68.11
(43.62~92.59)44.98
(31.54~58.43)51.05
(37.47~64.64)68.31
(21.10~115.52)H=12.969 0.011 Alb(g/L) 40.75
(38.43~43.07)37.10
(34.18~40.03)36.32
(34.78~37.85)34.86
(33.30~36.42)1)32.87
(30.35~35.40)1)H=23.967 <0.001 DBil(μmol/L) 7.28
(6.06~8.49)21.58
(15.73~27.42)1)15.37
(10.84~19.91)1)27.01
(16.68~37.34)1)20.83
(10.22~31.43)1)H=25.092 <0.001 IBil(μmol/L) 10.34
(8.23~12.45)12.77
(11.04~14.51)14.20
(10.51~17.89)14.51
(11.97~17.04)10.84
(7.78~13.90)H=3.563 0.468 TBil(μmol/L) 17.61
(14.52~20.70)34.35
(27.21~41.48)1)29.57
(22.72~36.43)1)41.34
(29.21~53.46)1)31.67
(20.33~43.00)H=14.340 0.006 PT(s) 14.09
(13.53~14.65)15.30
(14.73~15.87)15.43
(14.55~16.31)15.96
(15.21~16.72)1)15.54
(14.32~16.76)H=12.828 0.012 PLT(×109/L) 102.38
(85.03~119.72)113.68
(99.73~127.62)107.15
(81.69~132.60)116.20
(102.93~129.47)123.05
(90.65~155.45)H=7.245 0.124 NEUT(×109/L) 2.98
(2.44~3.52)3.50
(3.10~3.89)3.22
(2.73~3.72)3.69
(3.17~4.22)4.22
(3.50~4.94)1)H=10.882 0.028 LYM(×109/L) 0.98
(0.85~1.11)0.94
(0.86~1.03)0.98
(0.81~1.14)1.06
(0.93~1.19)1.03
(0.79~1.28)H=3.143 0.534 ALBI评分(分) -2.68
(-2.89~-2.47)-2.23v(-2.48~-1.97)1) -2.19
(-2.34~-2.03)1)-2.04
(-2.20~-1.87)1)-1.87
(-2.16~-1.59)1)H=26.470 <0.001 NLR 3.46
(2.78~4.14)4.58
(3.73~5.43)4.28
(3.28~5.28)3.98
(3.42~4.54)4.95
(3.76~6.13)H=5.496 0.240 注:与肝气郁结证比较,1)P<0.05;与气滞血瘀证比较,2)P<0.05。Child-Pugh分级,蔡尔德-皮尤分级;CNLC分期,中国肝癌临床分期;AFP,甲胎蛋白;AST,天冬氨酸氨基转移酶;ALT,丙氨酸氨基转移酶;Alb,白蛋白;DBil,直接胆红素;IBil,间接胆红素;TBil,总胆红素;PT,凝血酶原时间;PLT,血小板;NEUT,中性粒细胞;LYM,淋巴细胞;ALBI,白蛋白-胆红素评分;NLR,中性粒细胞/淋巴细胞比值。
 下载: 导出CSV
下载: 导出CSV
表 2 不同中医证型影像特征比较
Table 2. Comparison of imaging features of different TCM syndrome types
影像征象 肝气郁结证
(n=40)肝郁脾虚证
(n=109)气滞血瘀证
(n=62)湿热毒蕴证
(n=81)肝肾阴虚证
(n=20)统计值 P值 肿瘤数目[例(%)] χ2=16.470 0.002 单发 27(67.50) 51(46.79) 41(66.13) 48(59.26) 5(25.00)1) 多发 13(32.50) 58(53.21) 21(33.87) 33(40.74) 15(75.00)1) 肿瘤边界[例(%)] χ2=7.612 0.107 清晰 30(75.00) 63(57.80) 45(72.58) 52(64.20) 10(50.00) 模糊 10(25.00) 46(42.20) 17(27.42) 29(35.80) 10(50.00) 假包膜[例(%)] χ2=6.315 0.612 无假包膜 4(10.00) 15(13.76) 9(14.52) 12(14.81) 3(15.00) 不完全假包膜 19(47.50) 66(60.55) 32(51.61) 50(61.73) 11(55.00) 完全假包膜 17(42.50) 28(25.69) 21(33.87) 19(23.46) 6(30.00) 门静脉增宽[例(%)] 31(77.50) 86(78.90) 48(77.42) 61(75.31) 13(65.00) χ2=1.940 0.747 脾大[例(%)] 33(82.50) 98(89.91) 57(91.94) 69(85.19) 17(85.00) χ2=3.159 0.532 腹水[例(%)] 15(37.50) 72(66.06)1) 32(51.61) 53(65.43)1) 13(65.00) χ2=12.986 0.011 侧支循环开放[例(%)] 26(65.00) 74(67.89) 47(75.81) 54(66.67) 16(80.00) χ2=3.028 0.553 静脉癌栓[例(%)] 6(15.00) 35(32.11)2) 6(9.68) 23(28.40) 7(35.00) χ2=14.508 0.006 肝内转移[例(%)] 4(10.00) 38(34.86)1) 11(17.74) 25(30.86) 9(45.00)1) χ2=15.445 0.004 肝门区、腹膜后淋巴
结转移[例(%)]0(0.00) 24(22.02)1) 9(14.52) 18(22.22)1) 5(25.00)1) χ2=12.152 0.016 远处转移[例(%)] 2(5.00) 7(6.42) 6(9.68) 9(11.11) 2(10.00) χ2=2.141 0.710 肿瘤出血[例(%)] 4(10.00) 13(11.93) 3(4.84) 14(17.28) 4(20.00) χ2=6.424 0.170 卫星结节[例(%)] 8(20.00) 33(30.28) 9(14.52) 20(24.69) 6(30.00) χ2=6.093 0.192 肿瘤最长径(mm) 49.33
(39.85~58.80)67.25
(59.66~74.84)2)50.47
(41.81~59.12)64.44
(54.91~73.98)71.00
(53.16~88.84)H=13.082 0.011 ADC值(×10-3 mm2/s) 1.13
(1.07~1.19)1.23
(1.18~1.27)1.33
(1.23~1.44)1)1.35
(1.27~1.44)1)1.26
(1.15~1.36)H=20.940 <0.001 相对ADC值 0.81
(0.76~0.86)0.89
(0.85~0.93)0.98
(0.90~1.07)1)0.96
(0.89~1.02)1)0.92
(0.82~1.01)H=16.774 0.002 注:与肝气郁结证比较,1)P<0.05;与气滞血瘀证比较,2)P<0.05。ADC,表观扩散系数。
下载: 导出CSV
-
[1] BRAY F, LAVERSANNE M, SUNG H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2024, 74( 3): 229- 263. DOI: 10.3322/caac.21834. [2] HAN BF, ZHENG RS, ZENG HM, et al. Cancer incidence and mortality in China, 2022[J]. J Natl Cancer Cent, 2024, 4( 1): 47- 53. DOI: 10.1016/j.jncc.2024.01.006. [3] WANG HB, LU ZM, ZHAO XX. Tumorigenesis, diagnosis, and therapeutic potential of exosomes in liver cancer[J]. J Hematol Oncol, 2019, 12( 1): 133. DOI: 10.1186/s13045-019-0806-6. [4] BRUIX J, REIG M, SHERMAN M. Evidence-based diagnosis, staging, and treatment of patients with hepatocellular carcinoma[J]. Gastroenterology, 2016, 150( 4): 835- 853. DOI: 10.1053/j.gastro.2015.12.041. [5] Alliance of Liver Cancer Conversion Therapy, Committee of Liver Cancer, China Anti-Cancer Association. Chinese expert consensus on conversion and perioperative therapy of primary liver cancer(2024 edition)[J]. Chin J Dig Surg, 2024, 23( 4): 492- 513. DOI: 10.3760/cma.j.cn115610-20240228-00135.中国抗癌协会肝癌专业委员会转化治疗协作组. 原发性肝癌转化及围手术期治疗中国专家共识(2024版)[J]. 中华消化外科杂志, 2024, 23( 4): 492- 513. DOI: 10.3760/cma.j.cn115610-20240228-00135. [6] HU ZY, YANG QR, ZHOU C, et al. Mechanism of chemotherapy resistance of hepatocellular carcinoma and intervention with Chinese medicine: A review[J]. Chin J Exp Tradit Med Formulae, 2022, 28( 14): 254- 261. DOI: 10.13422/j.cnki.syfjx.20220923.胡泽玉, 杨清瑞, 周铖, 等. 肝癌化疗耐药机制及中药干预研究进展[J]. 中国实验方剂学杂志, 2022, 28( 14): 254- 261. DOI: 10.13422/j.cnki.syfjx.20220923. [7] GAO XY, HU J, CHEN LW. Application of healthy qi-reinforcing and tonifying Chinese medicines in primary liver cancer: A review[J]. World Chin Med, 2023, 18( 15): 2231- 2236. DOI: 10.3969/j.issn.1673-7202.2023.15.022.高心宇, 胡娟, 陈立武. 扶正补益类中药在原发性肝癌中应用研究进展[J]. 世界中医药, 2023, 18( 15): 2231- 2236. DOI: 10.3969/j.issn.1673-7202.2023.15.022. [8] ZHANG XY, GUAN ZY, LI WL, et al. Impact of clinical physicians’ interaction with intelligent platforms in assisting traditional Chinese medicine diagnosis and treatment decision-making: A survey[J]. World Chin Med, 2024, 19( 21): 3242- 3246. DOI: 10.3969/j.issn.1673-7202.2024.21.004.张心怡, 关之玥, 李文龙, 等. 临床医师应用智能平台交互辅助中医诊疗的影响调查[J]. 世界中医药, 2024, 19( 21): 3242- 3246. DOI: 10.3969/j.issn.1673-7202.2024.21.004. [9] ZHANG K, ZHU L, ZHU KJ. Exploration of the correlation between modern imaging and TCM syndromes and construction of new TCM syndrome imageology[J]. World Chin Med, 2016, 11( 6): 1101- 1104. DOI: 10.3969/j.issn.1673-7202.2016.06.045.张堃, 朱璐, 朱克俭. 探索证候与影像相关性, 构建中医证候影像新学科[J]. 世界中医药, 2016, 11( 6): 1101- 1104. DOI: 10.3969/j.issn.1673-7202.2016.06.045. [10] Korean Liver Cancer Association(KLCA), National Cancer Center(NCC) Korea. 2022 KLCA-NCC Korea practice guidelines for the management of hepatocellular carcinoma[J]. Clin Mol Hepatol, 2022, 28( 4): 583- 705. DOI: 10.3350/cmh.2022.0294. [11] National Health Commission of the People’s Republic of China. Standard for diagnosis and treatment of primary liver cancer(2024 edition)[J]. J Clin Hepatol, 2024, 40( 5): 893- 918. DOI: 10.12449/JCH240508.中华人民共和国国家卫生健康委员会. 原发性肝癌诊疗指南(2024年版)[J]. 临床肝胆病杂志, 2024, 40( 5): 893- 918. DOI: 10.12449/JCH240508. [12] Branch of Hepatobiliary Diseases, China Association of Chinese Medicine. Guideline for traditional Chinese medicine diagnosis and treatment of primary liver cancer[J]. J Clin Hepatol, 2024, 40( 5): 919- 927. DOI: 10.12449/JCH240509.中华中医药学会肝胆病分会. 原发性肝癌中医诊疗指南[J]. 临床肝胆病杂志, 2024, 40( 5): 919- 927. DOI: 10.12449/JCH240509. [13] KANG HJ, KIM H, LEE DH, et al. Gadoxetate-enhanced MRI features of proliferative hepatocellular carcinoma are prognostic after surgery[J]. Radiology, 2021, 300( 3): 572- 582. DOI: 10.1148/radiol.2021204352. [14] CHOI SY, KIM SH, PARK CK, et al. Imaging features of gadoxetic acid-enhanced and diffusion-weighted MR imaging for identifying cytokeratin 19-positive hepatocellular carcinoma: A retrospective observational study[J]. Radiology, 2018, 286( 3): 897- 908. DOI: 10.1148/radiol.2017162846. [15] ZHOU B. Research on disease, syndrome and symptom of liver cancer in ancient TCM literature[J]. Chin Arch Tradit Chin Med, 2011, 29( 12): 2714- 2716.周蓓. 肝癌相关中医病证症的古代文献研究[J]. 中华中医药学刊, 2011, 29( 12): 2714- 2716. [16] BU JJ, DOU XY, SUN M, et al. Exploring diagnosis and treatment of primary liver cancer by Chinese medical master ZHOU Zhongying based on compound pathogenesis theory[J]. Chin Arch Tradit Chin Med, 2025, 43( 2): 80- 83. DOI: 10.13193/j.issn.1673-7717.2025.02.018.补娟娟, 豆晓云, 孙萌, 等. 基于复合病机论探讨国医大师周仲瑛原发性肝癌辨治思路[J]. 中华中医药学刊, 2025, 43( 2): 80- 83. DOI: 10.13193/j.issn.1673-7717.2025.02.018. [17] HAN H, XU Q, DENG TH, et al. Study on TCM syndrome differentiation and treatment of 1869 cases of primary liver cancer in Hunan Province[J]. Guid J Tradit Chin Med Pharm, 2020, 26( 15): 112- 116. DOI: 10.13862/j.cnki.cn43-1446/r.2020.15.028.韩晗, 徐琦, 邓天好, 等. 湖南省1869例原发性肝癌患者的中医证治规律研究[J]. 中医药导报, 2020, 26( 15): 112- 116. DOI: 10.13862/j.cnki.cn43-1446/r.2020.15.028. [18] SHI ZY, FAN XF, GAO Y, et al. The distribution pattern of traditional Chinese medicine syndromes and influencing factors for primary liver cancer: An analysis of 415 cases[J]. J Clin Hepatol, 2025, 41( 1): 84- 91. DOI: 10.12449/JCH250113.石智尧, 凡晓菲, 高宇, 等. 415例原发性肝癌中医证候分布规律及影响因素分析[J]. 临床肝胆病杂志, 2025, 41( 1): 84- 91. DOI: 10.12449/JCH250113. [19] YU ZH, CHEN JB, XU GS, et al. CHAI Kequn's experience in application of four principles and four methods of traditional Chinese medicine in treating liver cancer based on syndrome differentiation[J]. J Tradit Chin Med, 2019, 60( 7): 559- 561. DOI: 10.13288/j.11-2166/r.2019.07.005.余志红, 陈嘉斌, 徐国暑, 等. 柴可群运用中医辨治肿瘤四则四法论治肝癌经验[J]. 中医杂志, 2019, 60( 7): 559- 561. DOI: 10.13288/j.11-2166/r.2019.07.005. [20] MATOBA M, TONAMI H, KONDOU T, et al. Lung carcinoma: Diffusion-weighted MR imaging: Preliminary evaluation with apparent diffusion coefficient[J]. Radiology, 2007, 243( 2): 570- 577. DOI: 10.1148/radiol.2432060131. [21] TARON J, JOHANNINK J, BITZER M, et al. Added value of diffusion-weighted imaging in hepatic tumors and its impact on patient management[J]. Cancer Imag, 2018, 18( 1): 10. DOI: 10.1186/s40644-018-0140-1. [22] LIU XA, ZHANG YF. Study on the correlation between the TCM syndrome types of primary liver cancer and the imaging manifestations of liver specific contrast agent[J]. Acta Chin Med, 2020, 35( 5): 1093- 1097. DOI: 10.16368/j.issn.1674-8999.2020.05.244.刘新爱, 张玉峰. 原发性肝癌的中医证型与肝脏特异性对比剂影像表现相关性研究[J]. 中医学报, 2020, 35( 5): 1093- 1097. DOI: 10.16368/j.issn.1674-8999.2020.05.244. [23] ZHANG SJ, CHEN Y, SUN BG, et al. Nature of spleen deficiency internal environment of hepatocellular carcinoma[J]. Chin Arch Tradit Chin Med, 2017, 35( 1): 7- 9. DOI: 10.13193/j.issn.1673-7717.2017.01.001.张诗军, 陈燕, 孙保国, 等. 肝癌的脾虚内环境本质研究[J]. 中华中医药学刊, 2017, 35( 1): 7- 9. DOI: 10.13193/j.issn.1673-7717.2017.01.001. [24] LUO HX, CHEN Y, SUN BG, et al. Establishment and evaluation of orthotopic hepatocellular carcinoma and drug-induced hepatocellular carcinoma in mice with spleen-deficiency syndrome in traditional Chinese medicine[J]. Afr J Tradit Complement Altern Med, 2016, 14( 1): 165- 173. DOI: 10.21010/ajtcam.v14i1.18. [25] MO ZM, LI P, CHEN QX, et al. Exploring the mechanism of enhanced metastasis of hepatocellular carcinoma in pi-deficiency state based on exosome miRNA sequencing[J]. Chin J Integr Tradit West Med, 2022, 42( 12): 1476- 1483. DOI: 10.7661/j.cjim.20220921.022.莫灼锚, 李攀, 陈秋霞, 等. 基于外泌体miRNA测序探讨肝癌在脾虚状态下转移增强机制[J]. 中国中西医结合杂志, 2022, 42( 12): 1476- 1483. DOI: 10.7661/j.cjim.20220921.022. [26] ZHANG JN, LIU XA. Correlation between TCM classification of primary liver cancer and MRI imaging manifestations[J]. Chin J Pract Med, 2020, 47( 10): 7- 10. DOI: 10.3760/cma.j.cn115689-20200103-00055.张瑾宁, 刘新爱. 原发性肝癌的中医分型与MRI影像学表现的相关性研究[J]. 中国实用医刊, 2020, 47( 10): 7- 10. DOI: 10.3760/cma.j.cn115689-20200103-00055. [27] LIN DY, PENG B, ZHENG JH, et al. Value of a logistic regression model based on the clinical features of liver cancer in judging the traditional Chinese medicine syndrome types of primary liver cancer[J]. J Clin Hepatol, 2020, 36( 6): 1293- 1298. DOI: 10.3969/j.issn.1001-5256.2020.06.021.林栋毅, 彭波, 郑景辉, 等. 基于肝癌临床特征构建的logistic回归模型对原发性肝癌中医证型的判断效能[J]. 临床肝胆病杂志, 2020, 36( 6): 1293- 1298. DOI: 10.3969/j.issn.1001-5256.2020.06.021. -

 本文二维码
本文二维码
计量
- 文章访问数: 204
- HTML全文浏览量: 44
- PDF下载量: 65
- 被引次数: 0

