
 PDF下载 ( 1526 KB)
PDF下载 ( 1526 KB)

二维剪切波弹性成像检测肝脾硬度对门静脉高压严重程度的评估价值
DOI: 10.12449/JCH260512
Value of liver and spleen stiffness measured by two-dimensional shear wave elastography in diagnosing the severity of portal hypertension
-
摘要:
目的 评估二维剪切波弹性成像(2D-SWE)测量的肝硬度值(LSM)及脾硬度值(SSM)在诊断严重门静脉高压(SPH)及高危静脉曲张(HRV)中的价值,为门静脉高压的无创评估提供依据。 方法 前瞻性纳入2019年12月—2023年4月在首都医科大学附属北京友谊医院肝病中心就诊的78例肝硬化门静脉高压患者为研究对象。根据肝静脉压力梯度(HVPG)水平分为3组:6 mmHg≤HVPG<12 mmHg、12 mmHg≤HVPG<20 mmHg和HVPG≥20 mmHg。所有患者均在HVPG测定后1周内完成胃镜及2D-SWE检查,记录2D-SWE测得的SWE-LSM及SWE-SSM。计量资料多组间比较采用单因素方差分析或Kruskal-Wallis H检验;计数资料组间比较采用χ2检验或Fisher确切概率法。以HVPG和胃镜检查结果为金标准,绘制受试者操作特征曲线,计算曲线下面积(AUC)以评价诊断效能,DeLong检验比较AUC。变量间相关性采用Pearson或Spearman相关分析,分别进行线性回归及Logistic回归分析HVPG及HRV的影响因素。 结果 78例患者的平均HVPG为(18.1±6.4)mmHg,HRV阳性62例(79.5%)。SWE-LSM及SWE-SSM均与HVPG呈显著正相关(r值分别为0.413、0.633,P值均<0.001),诊断HVPG≥12 mmHg时的AUC分别为0.812和0.902,诊断HVPG≥20 mmHg的AUC分别为0.804和0.789(P值均>0.05)。多因素线性回归分析结果显示,SWE-SSM是HVPG的独立影响因素(β=0.17,P<0.001)。在诊断HRV方面,仅SWE-SSM与HRV正相关(r=0.432,P<0.001),其诊断效能显著优于SWE-LSM(AUC:0.808 vs 0.642,Z=2.775,P=0.006)。多因素Logistic回归分析显示,血小板计数是HRV的独立影响因素(OR=0.97,P=0.014)。 结论 SWE-SSM与HVPG及HRV均密切相关,对SPH和HRV具有较好的诊断效能,有可能成为无创评估门静脉高压的有效方法。 Abstract:Objective To investigate the value of liver stiffness measurement (LSM) and spleen stiffness measurement (SSM) measured by two-dimensional shear wave elastography (2D-SWE) in the diagnosis of severe portal hypertension (SPH) and high-risk varices (HRV), and to provide a basis for noninvasive assessment of portal hypertension. Methods A prospective study was conducted among 78 patients with cirrhotic portal hypertension who were treated in Liver Research Center of Beijing Friendship Hospital, Capital Medical University, from December 2019 to April 2023. According to hepatic venous pressure gradient (HVPG), the patients were divided into 6 mmHg≤HVPG<12 mmHg group, 12 mmHg≤HVPG<20 mmHg group, and HVPG ≥20 mmHg group. All patients underwent gastroscopy and 2D-SWE within 1 week after HVPG measurement, and SWE-LSM and SWE-SSM measured by 2D-SWE were recorded. A one-way analysis of variance or the Kruskal-Wallis H test was used for comparison of continuous data between multiple groups, and the chi-square test or the Fisher’s exact test was used for comparison of categorical data between groups. With HVPG and gastroscopy findings as the gold standard, the receiver operating characteristic (ROC) curve was plotted and the area under the ROC curve (AUC) was calculated to evaluate diagnostic performance, while the DeLong test was used for comparison of AUC. The Pearson or Spearman correlation analysis was used to investigate the correlation between variables, and the linear regression analysis and the Logistic regression analysis were used to investigate the influencing factors for HVPG and HRV. Results The mean HVPG was 18.1±6.4 mmHg for the patients enrolled in this study, and HRV was observed in 62 patients (79.5%). Both SWE-LSM and SWE-SSM were significantly positively correlated with HVPG (r=0.413 and 0.633, both P<0.001), with an AUC of 0.812 and 0.902, respectively, in the diagnosis of HVPG≥12 mmHg and an AUC of 0.804 and 0.789, respectively, in the diagnosis of HVPG≥20 mmHg (all P>0.05). The multivariate linear regression analysis showed that SWE-SSM was an independent influencing factor for HVPG (β=0.17, P<0.001). In the diagnosis of HRV, only SWE-SSM showed a significant positive correlation with HRV (r=0.432, P<0.001), with a better diagnostic performance than SWE-LSM in terms of AUC (0.808 vs 0.642, Z=2.775, P=0.006). The multivariate Logistic regression analysis showed that platelet count was an independent influencing factor for HRV (odds ratio=0.97, P=0.014). Conclusion SWE-SSM is closely correlated with both HVPG and HRV, showing a good performance in the diagnosis of SPH and HRV, and therefore, it is expected to become an effective noninvasive tool for assessing portal hypertension. -
Key words:
- Liver Cirrhosis /
- Hypertension, Portal /
- Varicose Veins /
- Elasticity Imaging Techniques
-
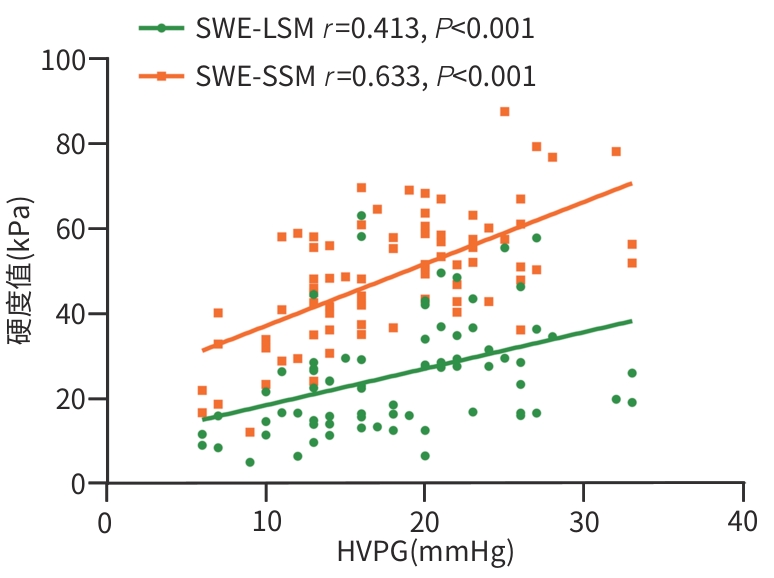
注: HVPG,肝静脉压力梯度;SWE,剪切波弹性成像;SWE-LSM,二维剪切波弹性成像测得的肝硬度值;SWE-SSM,二维剪切波弹性成像测得的脾硬度值。
图 1 SWE-LSM和SWE-SSM与HVPG的散点图
Figure 1. Scatter plots of SWE-LSM and SWE-SSM in patients with HVPG
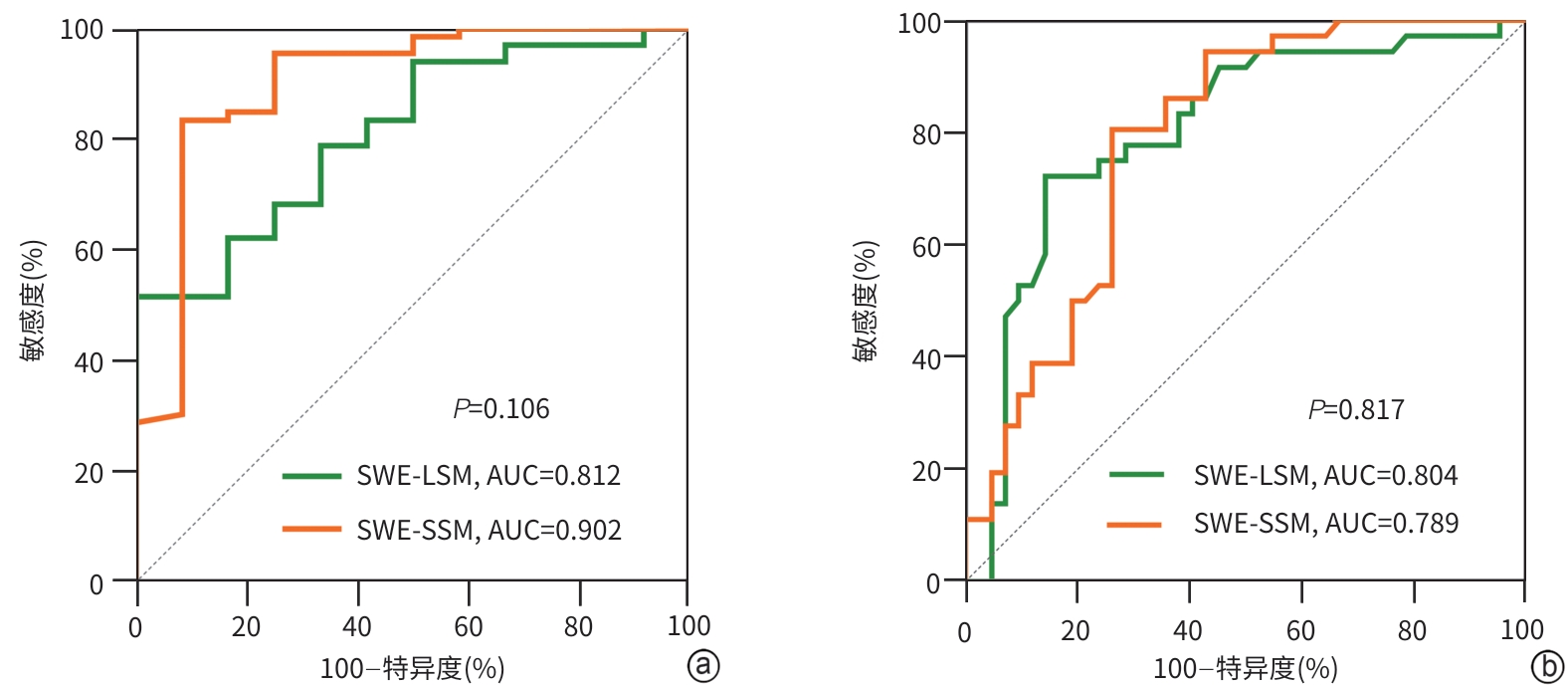
注: a,HVPG≥12 mmHg;b,HVPG≥20 mmHg。HVPG,肝静脉压力梯度;SWE-LSM,二维剪切波弹性成像测得的肝硬度值;SWE-SSM,二维剪切波弹性成像测得的脾硬度值;ROC曲线,受试者操作特征曲线;AUC,受试者操作特征曲线下面积;PH,门静脉高压。
图 2 SWE-LSM和SWE-SSM对不同程度PH诊断效能的ROC曲线
Figure 2. ROC curves of SWE-LSM and SWE-SSM for diagnosing severity of portal hypertension
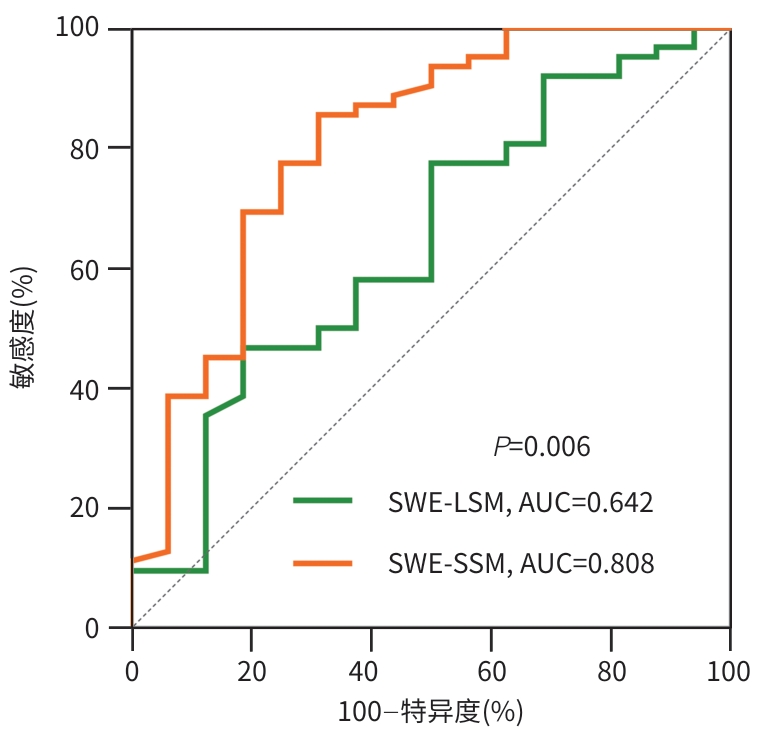
注: SWE-LSM,二维剪切波弹性成像测得的肝硬度值;SWE-SSM,二维剪切波弹性成像测得的脾硬度值;HRV,高危静脉曲张;AUC,受试者工作特征曲线下面积。
图 3 SWE-LSM和SWE-SSM对HRV的诊断效能
Figure 3. Diagnostic performance of SWE-LSM and SWE-SSM for high-risk varices
表 1 78例肝硬化PH患者的临床特征
Table 1. Clinical characteristics of 78 patients with liver cirrhosis and portal hypertension
指标 总计(n=78) 6 mmHg≤HVPG<
12 mmHg(n=12)12 mmHg≤HVPG<
20 mmHg(n=30)HVPG≥20 mmHg
(n=36)统计值 P值 男性[例(%)] 50(64.1) 8(66.7) 17(56.7) 25(69.4) χ2=1.20 0.565 年龄(岁) 54.2±10.6 50.1±10.4 55.5±9.5 54.6±11.5 F=1.16 0.319 病因[例(%)] — 0.200 病毒性肝炎 25(32.1) 6(50.0) 8(26.7) 11(30.6) 酒精性肝病 21(26.9) 0(0.0) 7(23.3) 14(38.9) 代谢相关脂肪性肝炎 9(11.5) 2(16.7) 4(13.3) 3(8.3) 自身免疫性肝病 15(19.2) 2(16.7) 7(23.3) 6(16.7) 其他 8(10.3) 2(16.7) 4(13.3) 2(5.6) BMI(kg/m2) 23.5(22.0~26.8) 23.6(21.7~26.7) 23.8(22.9~27.3) 23.0(21.7~25.9) H=1.10 0.576 ALT(U/L) 27.5(17.0~39.0) 31.0(20.0~38.5) 33.0(19.0~50.0) 23.0(15.5~36.0) H=3.73 0.155 AST(U/L) 36.5(28.0~51.8) 30.4(21.8~44.1) 35.3(31.3~50.6) 40.2(29.9~56.8) H=1.49 0.475 ALP(U/L) 92.5(74.0~138.0) 87.5(74.0~130.5) 90.0(72.0~133.0) 96.0(76.0~152.0) H=0.47 0.790 GGT(U/L) 44.0(28.0~88.0) 34.8(22.0~119.0) 47.5(32.0~100.0) 44.0(26.5~82.0) H=0.60 0.743 TBil(μmol/L) 25.9(15.0~38.1) 21.3(10.6~31.2) 20.3(13.3~31.2) 29.9(18.4~48.7) H=6.07 0.048 Alb(g/L) 33.5±5.1 37.2±5.6 35.4±4.1 30.7±4.2 F=14.61 <0.001 PLT(×109/L) 69.5(57.0~86.0) 89.5(70.5~184.5) 70.0(62.0~98.0) 63.0(47.5~75.5) H=12.04 0.002 PTA(%) 70.2±16.4 81.0±25.0 74.4±12.0 63.1±13.1 F=8.20 <0.001 Child-Pugh分级[例(%)] — <0.001 A级 31(39.7) 7(58.3) 19(63.3) 5(13.9) B级 34(43.6) 4(33.3) 9(30.0) 21(58.3) C级 13(16.7) 1(8.3) 2(6.7) 10(27.8) MELD评分(分) 9.2±4.6 8.8±4.3 7.8±4.3 10.6±4.7 F=3.18 0.047 HVPG(mmHg) 18.1±6.4 8.8±2.0 14.8±1.9 23.9±3.7 F=152.93 <0.001 HRV[例(%)] 62(79.5) 4(33.3) 25(83.3) 33(91.7) χ2=19.22 <0.001 SWE-LSM(kPa) 23.9(15.9~31.7) 13.3(8.9~19.4) 16.7(14.1~26.8) 29.6(24.9~42.3) H=24.26 <0.001 SWE-SSM(kPa) 49.1±14.9 30.1±12.7 47.1±11.7 57.0±11.4 F=24.37 <0.001 注:PH,门静脉高压;BMI,体重指数;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;ALP,碱性磷酸酶;GGT,γ-谷氨酰转移酶;TBil,总胆红素;Alb,白蛋白;PLT,血小板计数;PTA,凝血酶原活动度;Child-Pugh分级,蔡尔德-皮尤分级;MELD,终末期肝病模型;HVPG,肝静脉压力梯度;HRV,高危静脉曲张;SWE-LSM,二维剪切波弹性成像测得的肝硬度值;SWE-SSM,二维剪切波弹性成像测得的脾硬度值。
 下载: 导出CSV
下载: 导出CSV
表 2 SWE-LSM和SWE-SSM对不同程度PH及HRV的诊断效能
Table 2. Diagnostic performance of SWE-LSM and SWE-SSM for portal hypertension and high-risk varices
因素 AUC(95%CI) Cut-off值(kPa) 敏感度(%) 特异度(%) 阳性预测值(%) 阴性预测值(%) HVPG≥12 mmHg SWE-LSM 0.812(0.707~0.891) 26.6 51.5 100.0 100.0 27.3 SWE-SSM 0.902(0.814~0.958) 41.1 83.3 91.7 98.2 50.0 HVPG≥20 mmHg SWE-LSM 0.804(0.698~0.885) 27.2 72.2 85.7 81.2 78.3 SWE-SSM 0.789(0.682~0.873) 48.9 80.6 73.8 72.5 81.6 HRV SWE-LSM 0.642(0.526~0.748) 27.2 46.8 81.3 90.6 28.3 SWE-SSM 0.808(0.704~0.889) 40.4 85.5 68.8 91.4 55.0 注:PH,门静脉高压;HRV,高危静脉曲张;AUC,受试者操作特征曲线下面积;HVPG,肝静脉压力梯度;SWE-LSM,二维剪切波弹性成像测得的肝硬度值;SWE-SSM,二维剪切波弹性成像测得的脾硬度值。
下载: 导出CSV
表 3 HVPG影响因素的单因素回归分析
Table 3. Univariate regression analysis of influencing factors for HVPG
指标 β 95%CI P值 女性 -1.33 -4.31~1.66 0.387 年龄 0.05 -0.09~0.18 0.704 病因 病毒性肝炎 0.00 酒精性肝病 2.06 -1.71~5.84 0.287 代谢相关脂肪性肝炎 -1.17 -6.13~3.78 0.644 自身免疫性肝病 -0.71 -4.87~3.45 0.740 其他 -0.59 -5.77~4.59 0.824 BMI -0.07 -0.43~0.29 0.704 ALT -0.02 -0.06~0.02 0.330 AST 0.01 -0.01~0.03 0.359 ALP 0.00 -0.02~0.02 0.726 GGT -0.01 -0.02~0.01 0.248 TBil 0.04 -0.02~0.09 0.221 Alb -0.58 -0.84~-0.33 <0.001 PLT -0.07 -0.10~-0.04 <0.001 PTA -0.16 -0.24~-0.08 <0.001 SWE-LSM 0.20 0.10~0.30 <0.001 SWE-SSM 0.27 0.20~0.35 <0.001 注:BMI,体重指数;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;ALP,碱性磷酸酶;GGT,γ-谷氨酰转移酶;TBil,总胆红素;Alb,白蛋白;PLT,血小板计数;PTA,凝血酶原活动度;HVPG,肝静脉压力梯度;SWE-LSM,二维剪切波弹性成像测得的肝硬度值;SWE-SSM,二维剪切波弹性成像测得的脾硬度值;95%CI,95%置信区间。
下载: 导出CSV
表 4 HRV发生的单因素回归分析
Table 4. Univariate regression analysis of influencing factors for HRV
指标 OR 95%CI P值 女性 0.92 0.29~2.86 0.881 年龄 1.03 0.98~1.09 0.229 病因 病毒性肝炎 1.00 酒精性肝病 3.69 0.68~20.19 0.132 代谢相关脂肪性肝炎 1.36 0.23~8.22 0.737 自身免疫肝病 5.44 0.60~49.56 0.133 其他 0.39 0.08~2.00 0.258 BMI 0.98 0.86~1.12 0.749 ALT 0.99 0.98~1.00 0.165 AST 1.00 0.99~1.01 0.867 ALP 1.01 1.00~1.02 0.212 GGT 1.00 0.99~1.00 0.304 TBil 1.00 0.98~1.02 0.796 Alb 0.97 0.87~1.09 0.618 PLT 0.96 0.94~0.98 <0.001 PTA 0.98 0.95~1.02 0.300 SWE-LSM 1.04 0.99~1.09 0.141 SWE-SSM 1.11 1.05~1.17 <0.001 注:BMI,体重指数;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;ALP,碱性磷酸酶;GGT,γ-谷氨酰转移酶;TBil,总胆红素;Alb,白蛋白;PLT,血小板计数;PTA,凝血酶原活动度;HRV,高危静脉曲张;SWE-LSM,二维剪切波弹性成像测得的肝硬度值;SWE-SSM,二维剪切波弹性成像测得的脾硬度值;95%CI,95%置信区间。
下载: 导出CSV
-
[1] de FRANCHIS R, BOSCH J, GARCIA-TSAO G, et al. Baveno VII-Renewing consensus in portal hypertension[J]. J Hepatol, 2022, 76( 4): 959- 974. DOI: 10.1016/j.jhep.2021.12.022. [2] WEI JA, YANG SW, WANG Y, et al. Balloon and end-hole catheter measurement of hepatic venous pressure gradient:A retrospective comparative study[J/CD]. Chin J Liver Dis(Electronic Version), 2025, 17( 1): 64- 68. DOI: 10.3969/j.issn.1674-7380.2025.01.010.尉建安, 杨思维, 王宇, 等. 球囊法和端孔导管法测量肝静脉压力梯度: 一项回顾性对照研究[J/CD]. 中国肝脏病杂志(电子版), 2025, 17( 1): 64- 68. DOI: 10.3969/j.issn.1674-7380.2025.01.010. [3] KAPLAN DE, RIPOLL C, THIELE M, et al. AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis[J]. Hepatology, 2024, 79( 5): 1180- 1211. DOI: 10.1097/HEP.0000000000000647. [4] Chinese Society of Hepatology, Chinese Society of Gastroenterology, Chinese Society of Digestive Endoscopology of Chinese Medical Association. Guidelines on the management of esophagogastric variceal bleeding in cirrhotic portal hypertension[J]. J Clin Hepatol, 2023, 39( 3): 527- 538. DOI: 10.3760/cmaj.cn501113-20220824-00436.中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会消化内镜学分会. 肝硬化门静脉高压食管胃静脉曲张出血的防治指南[J]. 临床肝胆病杂志, 2023, 39( 3): 527- 538. DOI: 10.3760/cmaj.cn501113-20220824-00436. [5] STERLING RK, ASRANI SK, LEVINE D, et al. AASLD Practice Guideline on noninvasive liver disease assessment of portal hypertension[J]. Hepatology, 2025, 81( 3): 1060- 1085. DOI: 10.1097/HEP.0000000000000844. [6] DAJTI E, HUBER AT, FERRAIOLI G, et al. Advances in imaging-elastography[J]. Hepatology, 2025. DOI: 10.1097/HEP.0000000000001342. [7] VIZZUTTI F, ARENA U, ROMANELLI RG, et al. Liver stiffness measurement predicts severe portal hypertension in patients with HCV-related cirrhosis[J]. Hepatology, 2007, 45( 5): 1290- 1297. DOI: 10.1002/hep.21665. [8] STEFANESCU H, MARASCO G, CALÈS P, et al. A novel spleen-dedicated stiffness measurement by FibroScan® improves the screening of high-risk oesophageal varices[J]. Liver Int, 2020, 40( 1): 175- 185. DOI: 10.1111/liv.14228. [9] BERZIGOTTI A. Non-invasive evaluation of portal hypertension using ultrasound elastography[J]. J Hepatol, 2017, 67( 2): 399- 411. DOI: 10.1016/j.jhep.2017.02.003. [10] Chinese Society of Hepatology, Chinese Medical Association. Chinese guidelines on the management of liver cirrhosis[J]. J Clin Hepatol, 2019, 35( 11): 2408- 2425. DOI: 10.3969/j.issn.1001-5256.2019.11.006.中华医学会肝病学分会. 肝硬化诊治指南[J]. 临床肝胆病杂志, 2019, 35( 11): 2408- 2425. DOI: 10.3969/j.issn.1001-5256.2019.11.006. [11] Chinese Portal Hypertension Alliance(CHESS); Minimally Invasive Intervention Collaborative Group, Chinese Society of Gastroenterology. Consensus on clinical application of hepatic venous pressure gradient in China(2023 edition)[J]. Natl Med J China, 2023, 103( 48): 3885- 3895. DOI: 10.3760/cma.j.cn112137-20230831-00342.中国门静脉高压联盟(CHESS), 中华医学会消化病学分会微创介入协作组. 中国肝静脉压力梯度临床应用专家共识(2023版)[J]. 中华医学杂志, 2023, 103( 48): 3885- 3895. DOI: 10.3760/cma.j.cn112137-20230831-00342. [12] FERRAIOLI G, WONG VW, CASTERA L, et al. Liver ultrasound elastography: An update to the world federation for ultrasound in medicine and biology guidelines and recommendations[J]. Ultrasound Med Biol, 2018, 44( 12): 2419- 2440. DOI: 10.1016/j.ultrasmedbio.2018.07.008. [13] Chinese Society of Ultrasound in Medicine, Chinese Portal Hypertension Alliance(CHESS). Chinese expert consensus on the diagnosis of cirrhotic portal hypertension by ultrasound elastography(2023 version)[J]. Natl Med J China, 2023, 103( 32): 2480- 2494. DOI: 10.3760/cma.j.cn112137-20230513-00782.中华医学会超声医学分会, 中国门静脉高压联盟(CHESS). 中国超声弹性成像技术诊断肝硬化门静脉高压专家共识(2023版)[J]. 中华医学杂志, 2023, 103( 32): 2480- 2494. DOI: 10.3760/cma.j.cn112137-20230513-00782. [14] KIM HY, SO YH, KIM W, et al. Non-invasive response prediction in prophylactic carvedilol therapy for cirrhotic patients with esophageal varices[J]. J Hepatol, 2019, 70( 3): 412- 422. DOI: 10.1016/j.jhep.2018.10.018. [15] TURCO L, GARCIA-TSAO G. Portal hypertension: Pathogenesis and diagnosis[J]. Clin Liver Dis, 2019, 23( 4): 573- 587. DOI: 10.1016/j.cld.2019.07.007. [16] GUIXÉ-MUNTET S, ZHU CP, XIE WF, et al. Novel therapeutics for portal hypertension and fibrosis in chronic liver disease[J]. Pharmacol Ther, 2020, 215: 107626. DOI: 10.1016/j.pharmthera.2020.107626. [17] JANSEN C, BOGS C, VERLINDEN W, et al. Shear-wave elastography of the liver and spleen identifies clinically significant portal hypertension: A prospective multicentre study[J]. Liver Int, 2017, 37( 3): 396- 405. DOI: 10.1111/liv.13243. [18] THIELE M, HUGGER MB, KIM Y, et al. 2D shear wave liver elastography by Aixplorer to detect portal hypertension in cirrhosis: An individual patient data meta-analysis[J]. Liver Int, 2020, 40( 6): 1435- 1446. DOI: 10.1111/liv.14439. [19] STEFANESCU H, RUSU C, LUPSOR-PLATON M, et al. Liver stiffness assessed by ultrasound shear wave elastography from general electric accurately predicts clinically significant portal hypertension in patients with advanced chronic liver disease[J]. Ultraschall Med, 2020, 41( 5): 526- 533. DOI: 10.1055/a-0965-0745. [20] GRGUREVIC I, MADIR A, TRKULJA V, et al. Assessment of clinically significant portal hypertension by two-dimensional shear wave elastography[J]. Eur J Clin Invest, 2022, 52( 6): e13750. DOI: 10.1111/eci.13750. [21] ZHU YL, DING H, FU TT, et al. Portal hypertension in hepatitis B-related cirrhosis: Diagnostic accuracy of liver and spleen stiffness by 2-D shear-wave elastography[J]. Hepatol Res, 2019, 49( 5): 540- 549. DOI: 10.1111/hepr.13306. [22] HU X, HUANG XJ, HOU JH, et al. Diagnostic accuracy of spleen stiffness to evaluate portal hypertension and esophageal varices in chronic liver disease: A systematic review and meta-analysis[J]. Eur Radiol, 2021, 31( 4): 2392- 2404. DOI: 10.1007/s00330-020-07223-8. [23] LIU Y, TAN HY, ZHANG XG, et al. Prediction of high-risk esophageal varices in patients with chronic liver disease with point and 2D shear wave elastography: A systematic review and meta-analysis[J]. Eur Radiol, 2022, 32( 7): 4616- 4627. DOI: 10.1007/s00330-022-08601-0. [24] KARAGIANNAKIS DS, MARKAKIS G, LEKAKIS V. Evaluation of spleen stiffness by 2D shear wave elastography for ruling out high risk varices in patients with chronic advanced liver disease. A systematic review and meta-analysis[J]. Eur J Radiol, 2024, 175: 111475. DOI: 10.1016/j.ejrad.2024.111475. [25] YU MR, YANG J, WANG JY, et al. Value of spleen stiffness measured by two-dimensional shear wave elastography combined with platelet count/spleen diameter ratio in evaluating moderate-to-severe gastroesophageal varices in patients with hepatitis B cirrhosis[J]. J Clin Hepatol, 2021, 37( 7): 1572- 1577. DOI: 10.3969/j.issn.1001-5256.2021.07.019.余敏睿, 杨杰, 王进勇, 等. 二维剪切波弹性成像测量脾硬度联合血小板/脾直径对乙型肝炎肝硬化患者中重度食管胃静脉曲张的评估价值[J]. 临床肝胆病杂志, 2021, 37( 7): 1572- 1577. DOI: 10.3969/j.issn.1001-5256.2021.07.019. [26] MUZICA C, DIACONU S, ZENOVIA S, et al. Role of spleen stiffness measurements with 2D shear-wave elastography for esophageal varices in patients with compensated advanced chronic liver disease[J]. Diagnostics, 2025, 15( 6): 674. DOI: 10.3390/diagnostics15060674. [27] YAN YL, XING X, WANG XZ, et al. Liver stiffness by two-dimensional shear wave elastography for screening high-risk varices in patients with compensated advanced chronic liver disease[J]. Eur Radiol, 2022, 32( 3): 2078- 2088. DOI: 10.1007/s00330-021-08280-3. -

 本文二维码
本文二维码
计量
- 文章访问数: 201
- HTML全文浏览量: 48
- PDF下载量: 82
- 被引次数: 0

