
 PDF下载 ( 3506 KB)
PDF下载 ( 3506 KB)

血清肠型脂肪酸结合蛋白对肝硬化食管胃静脉曲张破裂出血患者内镜下止血后短期死亡的预测价值
DOI: 10.12449/JCH260511
Value of serum intestinal fatty acid-binding protein in predicting short-term mortality after endoscopic hemostasis for esophagogastric variceal bleeding in patients with liver cirrhosis
-
摘要:
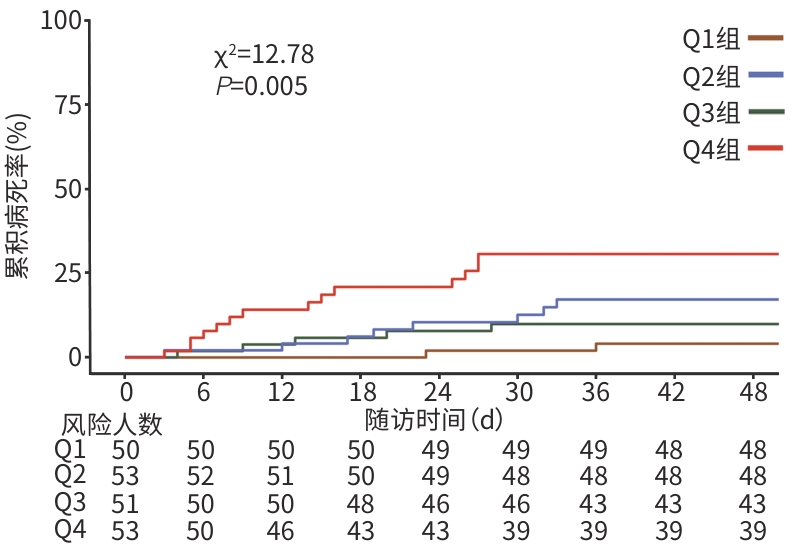
目的 探讨肠型脂肪酸结合蛋白(I-FABP)对成功接受内镜下止血治疗的肝硬化食管胃静脉曲张破裂出血(EVB)患者6周病死率的预测价值。 方法 回顾性分析2020年9月—2025年6月在延边大学附属医院因EVB接受内镜治疗(包括套扎术和硬化剂注射术)的207例肝硬化患者的临床资料。研究终点为出血相关6周病死率。采用酶联免疫吸附法测定患者入院血清I-FABP水平,并按I-FABP检测值四分位数进行分层分析。计量资料两组间比较采用Mann-Whitney U检验;计数资料两组间比较采用χ2检验。通过Kaplan-Meier生存分析、Cox回归及限制性立方样条曲线探究I-FABP与6周病死率的关联。通过机器学习模型进一步量化I-FABP对预后的影响。采用综合布里尔评分和综合累积/动态曲线下面积评估时间依赖性变量的重要性。采用受试者操作特征(ROC)曲线评估预测模型的性能。 结果 研究期间,共有29例(14.0%)患者在内镜止血成功后6周内死亡,中位死亡时间为16(8~26)d。死亡组的血清I-FABP水平高于生存组,差异有统计学意义(Z=-3.731,P<0.001)。Kaplan-Meier生存分析显示,不同I-FABP四分位数分组患者的6周病死率差异有统计学意义(χ2=12.78,P=0.005)。多因素Cox回归分析显示,I-FABP升高是6周病死率的独立影响因素(风险比=1.87,P=0.003)。限制性立方样条曲线分析显示,I-FABP与6周病死率之间呈线性关联(P非线性=0.280,P总体=0.029)。机器学习模型结果显示,I-FABP的重要性随时间推移呈动态变化特征,置换后布里尔评分损失和累积/动态曲线下面积损失均表明I-FABP是影响6周病死率的重要变量。 结论 I-FABP水平与肝硬化EVB患者内镜下止血后的6周死亡风险独立相关,可作为短期预后不良的潜在生物标志物。 Abstract:Objective To investigate the value of intestinal fatty acid-binding protein (I-FABP) in predicting 6-week mortality in patients with liver cirrhosis after successful endoscopic hemostasis for esophagogastric variceal bleeding (EVB). Methods A retrospective analysis was performed for the clinical data of 207 patients with liver cirrhosis who underwent successful endoscopic treatment for EVB (including ligation and sclerotherapy) in The Affiliated Hospital of Yanbian University from September 2020 to June 2025, with the endpoint of 6-week bleeding-related mortality. ELISA was used to measure the serum level of I-FABP on admission, and a stratified analysis was performed based on the quartiles of I-FABP measurements. The Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two groups; the chi-square test was used for comparison of categorical data between two groups. The Kaplan-Meier survival analysis, Cox regression analysis, and restricted cubic spline (RCS) curve were used to investigate the association between I-FABP and mortality. Machine learning models were used to further quantify the impact of I-FABP on mortality. The integrated Brier score and an integrated cumulative/dynamic area under the curve were used to assess the importance of time-dependent variables, and the receiver operating characteristic (ROC) curve was used to assess the performance of the predictive model. Results During the study, 29 patients (14.0%) died within 6 weeks after successful endoscopic hemostasis, with a median time to death of 16 (8—26) days. The mortality group had a significantly higher serum level of I-FABP than the survival group (Z=-3.731, P<0.001). The Kaplan-Meier survival analysis showed that there was a significant difference in 6-week mortality between the groups of patients based on I-FABP quartiles (χ2 =12.78, P=0.005). The multivariable Cox regression analysis showed that an increase in I-FABP (hazard ratio=1.87, P=0.003) was an independent influencing factor for 6-week mortality. The RCS analysis showed a linear relationship between I-FABP and 6-week mortality (Pnon-linear=0.280, Poverall=0.029). Machine learning models showed that there was a dynamic change in the importance of I-FABP over time, and Brier score loss and the loss of cumulative/dynamic area under the curve after permutation showed that I-FABP was an important variable affecting 6-week mortality rate. Conclusion I-FABP level is independently associated with the risk of 6-week mortality endoscopic hemostasis for EVB in patients with liver cirrhosis, and therefore, it can be used as a potential biomarker for poor short-term prognosis. -
注: I-FABP,肠型脂肪酸结合蛋白;EVB,食管胃静脉曲张破裂出血。
图 1 不同I-FABP四分位数分组的EVB患者6周病死率Kaplan-Meier曲线
Figure 1. Kaplan-Meier curve of 6-week mortality rates for EVB patients stratified by I-FABP quartiles
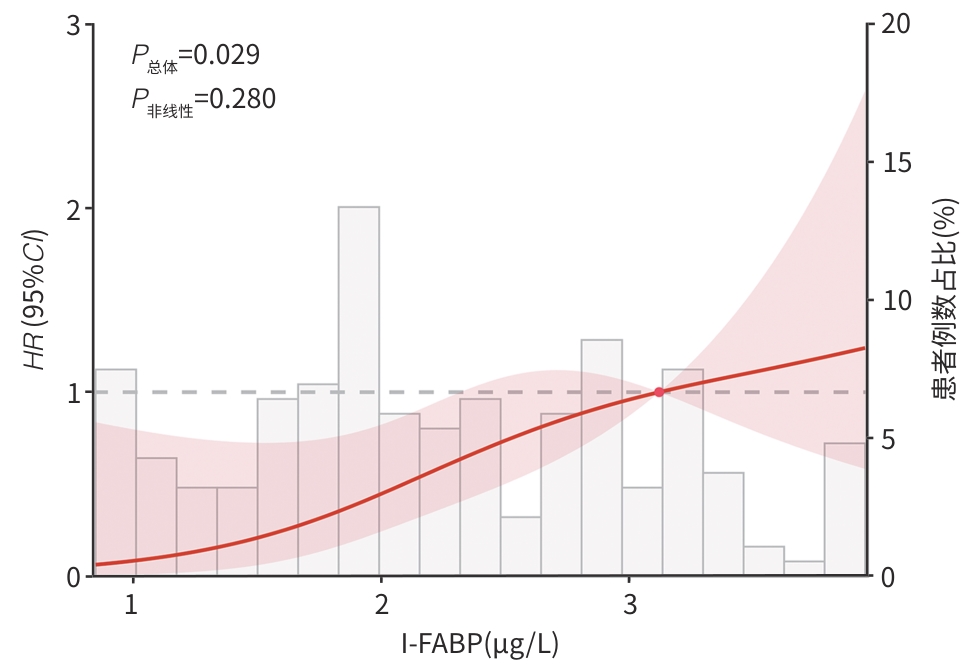
注: I-FABP,肠型脂肪酸结合蛋白;EVB,食管胃静脉曲张破裂出血;HR,风险比;95%CI,95%置信区间。
图 2 I-FABP与EVB患者6周病死率相关性的RCS分析
Figure 2. RCS analysis of the correlation between I-FABP and 6-week mortality in EVB patients
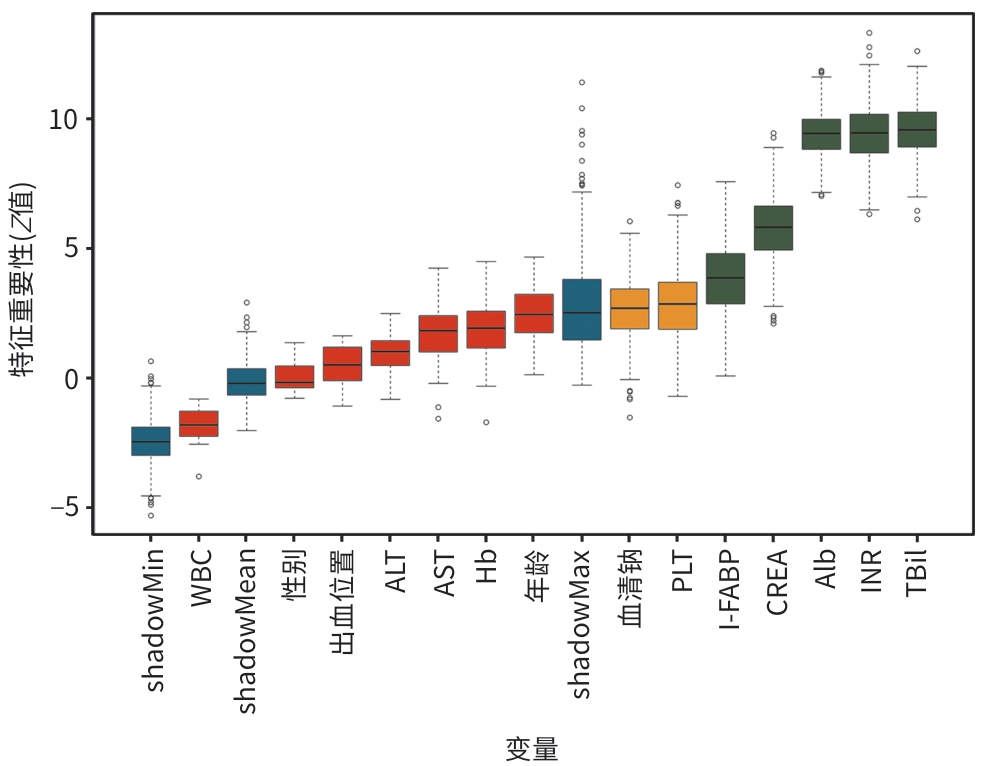
注: WBC,白细胞;Hb,血红蛋白;PLT,血小板计数;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;Alb,白蛋白;CREA,肌酐;TBil,总胆红素;INR,国际标准化比值;I-FABP,肠型脂肪酸结合蛋白。Shadow-Max,影子特征高值;ShadowMean,影子特征均值;ShadowMin,影子特征低值。绿色表示重要变量。
图 3 Boruta算法识别影响6周病死率的关键变量
Figure 3. Boruta algorithm identifying key variables for predicting 6-week mortality
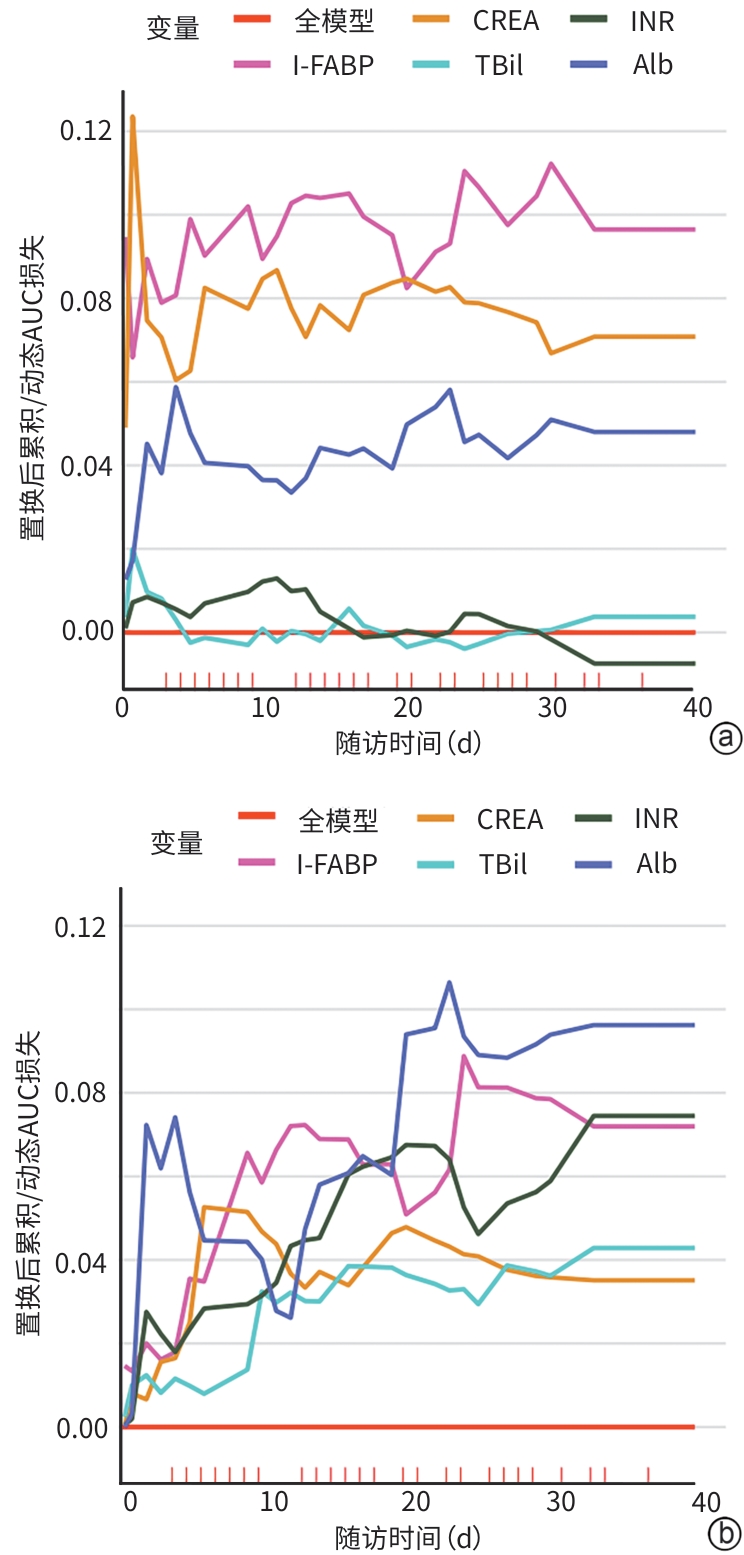
注: a,基于Cox比例风险模型;b,基于随机生存森林模型。纵轴表示置换后各协变量的损失,损失值越大表明对应的协变量对维持模型预测性能的重要性越高。Alb,白蛋白;CREA,肌酐;TBil,总胆红素;INR,国际标准化比值;I-FABP,肠型脂肪酸结合蛋白;AUC,曲线下面积。
图 4 置换后累积/动态AUC损失评估变量的时间依赖重要性
Figure 4. Time-dependent feature importance for the whole cohort, cumulative/dynamic AUC loss after permutation
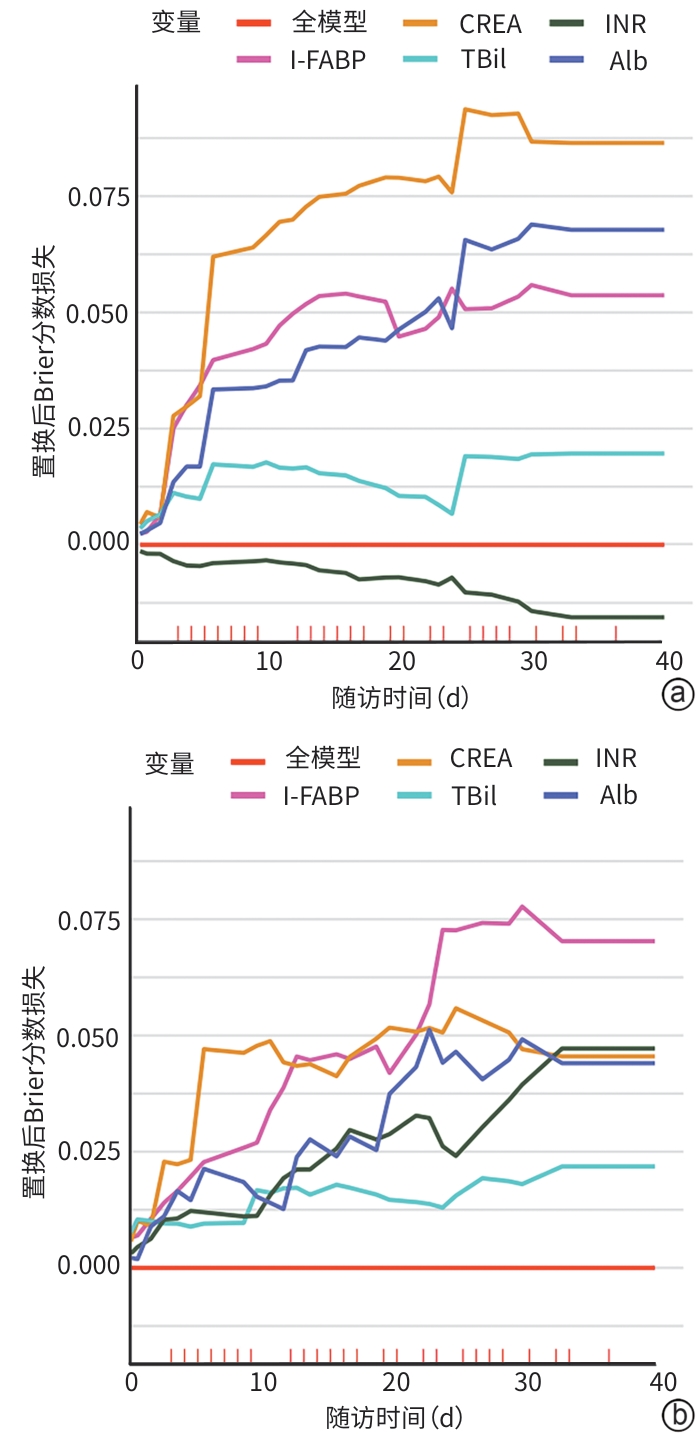
注: a,基于Cox比例风险模型;b,基于随机生存森林模型。纵轴表示置换后各协变量的损失,损失值越大表明对应的协变量对维持模型预测性能的重要性越高。Alb,白蛋白;CREA,肌酐;TBil,总胆红素;INR,国际标准化比值;I-FABP,肠型脂肪酸结合蛋白。
图 5 置换后Brier评分损失评估变量的时间依赖重要性
Figure 5. Time-dependent feature importance for the whole cohort, Brier score loss after permutation
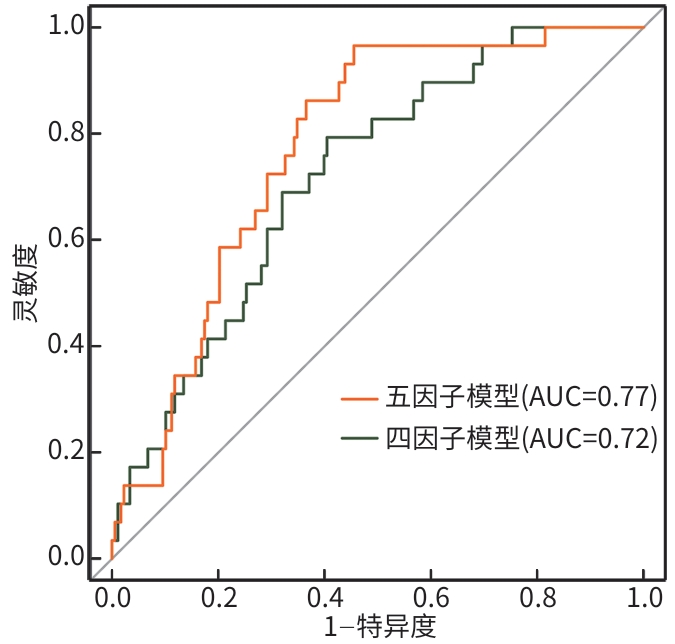
注: EVB,食管胃静脉曲张破裂出血;ROC,受试者操作特征;AUC,曲线下面积。
图 6 Cox比例风险模型预测EVB患者6周死亡的ROC曲线
Figure 6. ROC curve of the Cox proportional hazards model for predicting 6-week mortality in EVB patients
表 1 不同预后分组患者基线特征比较
Table 1. Comparison of baseline characteristics of patients in different groups
指标 生存组(n=178) 死亡组(n=29) 统计值 P值 年龄(岁) 58(43~65) 58(53~66) Z=-1.053 0.292 性别[例(%)] χ2=0.211 0.646 男 122(68.54) 21(72.41) 女 56(31.46) 8(27.59) 腹水[例(%)] 87(48.88) 20(68.97) χ2=4.030 0.045 门静脉血栓[例(%)] 35(19.66) 8(27.59) χ2=0.951 0.329 肝性脑病[例(%)] 28(15.73) 11(37.93) χ2=8.038 0.005 肝细胞癌[例(%)] 19(10.67) 10(34.48) χ2=9.841 0.002 Child-Pugh分级[例(%)] χ2=33.213 <0.001 A级 50(28.09) 2(6.90) B级 88(49.44) 5(17.24) C级 40(22.47) 22(75.86) 静脉曲张出血部位[例(%)] χ2=3.438 0.633 Le-s 14(7.87) 3(10.34) Le-m 77(43.26) 16(55.17) Le-i 25(14.04) 3(10.34) Lg-c 51(28.65) 6(20.69) Lg-cf 3(1.69) 1(3.45) Lg-f 8(4.49) 0(0.00) WBC(×109/L) 5.12(3.67~6.98) 5.65(4.02~9.20) Z=‒1.406 0.160 Hb(g/L) 96.00(80.00~110.00) 83.00(70.00~90.00) Z=3.668 <0.001 PLT(×109/L) 77.00(61.00~96.00) 53.00(45.00~67.00) Z=4.489 <0.001 血清钠(mmol/L) 136.00(134.00~140.00) 133.00(130.00~135.00) Z=3.801 <0.001 ALT(U/L) 37.00(27.00~51.00) 52.00(24.00~67.00) Z=‒0.308 0.758 AST(U/L) 54.00(35.00~73.00) 55.00(38.00~105.00) Z=‒1.668 0.095 Alb(g/L) 33.00(30.00~35.00) 28.00(26.00~32.00) Z=3.728 <0.001 CREA(μmol/L) 78.00(63.00~96.00) 97.00(84.00~137.00) Z=‒4.246 <0.001 TBil(μmol/L) 34.40(21.90~49.50) 61.20(33.50~85.10) Z=‒3.397 0.001 INR 1.39(1.24~1.68) 1.85(1.51~2.05) Z=‒4.176 <0.001 I-FABP(μg/L) 1.96(1.52~2.83) 2.88(2.24~3.29) Z=‒3.731 <0.001 MELD评分(分) 11.00(7.00~17.00) 19.00(17.00~21.00) Z=‒4.987 <0.001 注:Child-Pugh分级,蔡尔德-皮尤分级;WBC,白细胞;Hb,血红蛋白;PLT,血小板计数;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;Alb,白蛋白;CREA,肌酐;TBil,总胆红素;INR,国际标准化比值;I-FABP,肠型脂肪酸结合蛋白;MELD,终末期肝病模型。
 下载: 导出CSV
下载: 导出CSV
表 2 I-FABP与6周病死率的Cox回归分析
Table 2. Cox regression analysis of I-FABP and 6-week mortality
变量 单因素分析 多因素分析 Β值 HR(95%CI) P值 Β值 HR(95%CI) P值 I-FABP水平 0.664 1.94(1.32~2.86) 0.001 0.627 1.87(1.23~2.84) 0.003 I-FABP四分位数分层 Q1组 1.00 1.00 Q2组 0.905 2.47(0.48~12.74) 0.259 0.889 2.43(0.47~12.74) 0.230 Q3组 1.423 4.15(0.88~19.53) 0.064 1.025 2.79(0.58~13.46) 0.322 Q4组 2.049 7.77(1.76~34.17) 0.005 1.864 6.45(1.43~29.13) 0.017 注:I-FABP,肠型脂肪酸结合蛋白;HR,风险比;95%CI,95%置信区间。
下载: 导出CSV
表 3 联合模型对EVB患者6周病死率的预测效能
Table 3. Predictive performance of the combined model on 6-week mortality in EVB patients
模型 AUC(95%CI) 敏感度(%) 特异度(%) 阳性预测值(%) 阴性预测值(%) P值 四因子模型 0.72(0.63~0.81) 79.3 59.6 24.2 94.6 <0.001 五因子模型 0.77(0.70~0.85) 96.6 54.5 25.7 99.0 <0.001 注:EVB,食管胃静脉曲张破裂出血;AUC,曲线下面积;95%CI,95%置信区间。
下载: 导出CSV
-
[1] GARCIA-TSAO G, ABRALDES JG, BERZIGOTTI A, et al. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases[J]. Hepatology, 2017, 65( 1): 310- 335. DOI: 10.1002/hep.28906. [2] LYU Y, HAN GH, FAN DM. Current status of treatment for acute variceal bleeding in liver cirrhosis[J]. Chin J Hepatol, 2024, 32( 11): 1037- 1041. DOI: 10.3760/cma.j.cn501113-20240306-00113.吕勇, 韩国宏, 樊代明. 肝硬化急性静脉曲张出血的治疗现状[J]. 中华肝脏病杂志, 2024, 32( 11): 1037- 1041. DOI: 10.3760/cma.j.cn501113-20240306-00113. [3] Chinese Society of Spleen and Portal Hypertension Surgery, Chinese Society of Surgery, Chinese Medical Association. Expert consensus on the diagnosis and treatment of esophageal and gastric variceal rupture bleeding in cirrhotic portal hypertension(2025 edition)[J]. Chin J Dig Surg, 2025, 24( 3): 271- 280. DOI: 10.3760/cma.j.cn115610-20241228-00590.中华医学会外科学分会脾及门静脉高压外科学组. 肝硬化门静脉高压症食管、胃底静脉曲张破裂出血诊治专家共识(2025版)[J]. 中华消化外科杂志, 2025, 24( 3): 271- 280. DOI: 10.3760/cma.j.cn115610-20241228-00590. [4] GRALNEK IM, CAMUS DUBOC M, GARCIA-PAGAN JC, et al. Endoscopic diagnosis and management of esophagogastric variceal hemorrhage: European Society of Gastrointestinal Endoscopy(ESGE) Guideline[J]. Endoscopy, 2022, 54( 11): 1094- 1120. DOI: 10.1055/a-1939-4887. [5] de FRANCHIS R, BOSCH J, GARCIA-TSAO G, et al. Baveno VII- renewing consensus in portal hypertension[J]. J Hepatol, 2022, 76( 4): 959- 974. DOI: 10.1016/j.jhep.2021.12.022. [6] LI XH, QI XS, WANG J, et al. Construction and optimization of an endoscopic quality control system for esophageal and gastric varices in liver cirrhosis[J]. Clin J Med Offic, 2026, 54( 1): 1- 5, 10. DOI: 10.16680/j.1671-3826.2026.01.01.李鑫会, 祁兴顺, 王静, 等. 肝硬化食管胃静脉曲张内镜管理质量控制体系构建与优化[J]. 临床军医杂志, 2026, 54( 1): 1- 5, 10. DOI: 10.16680/j.1671-3826.2026.01.01. [7] Chinese Society of Hepatology, Chinese Society of Gastroenterology, Chinese Society of Digestive Endoscopy; Chinese Medical Association. Guidelines on the management of esophagogastric variceal bleeding in cirrhotic portal hypertension[J]. J Clin Hepatol, 2023, 39( 3): 527- 538.中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会消化内镜学分会. 肝硬化门静脉高压食管胃静脉曲张出血的防治指南[J]. 临床肝胆病杂志, 2023, 39( 3): 527- 538. [8] BAFFY G. Potential mechanisms linking gut microbiota and portal hypertension[J]. Liver Int, 2019, 39( 4): 598- 609. DOI: 10.1111/liv.13986. [9] LOMBARDI M, TROISI J, MOTTA BM, et al. Gut-liver axis dysregulation in portal hypertension: Emerging frontiers[J]. Nutrients, 2024, 16( 7): 1025. DOI: 10.3390/nu16071025. [10] LI B, HAO JQ, ZENG J, et al. SnapShot: FABP functions[J]. Cell, 2020, 182( 4): 1066- 1066. DOI: 10.1016/j.cell.2020.07.027. [11] SMATHERS RL, PETERSEN DR. The human fatty acid-binding protein family: Evolutionary divergences and functions[J]. Hum Genomics, 2011, 5( 3): 170- 191. DOI: 10.1186/1479-7364-5-3-170. [12] HAN CJ, WU ZX, HUANG Y, et al. Correlation between intestinal fatty acid-binding protein and bacterial infection as well as poor prognosis in patients with liver cirrhosis[J]. Chin J Infect Control, 2023, 22( 3): 315- 321. DOI: 10.12138/j.issn.1671-9638.20233630.韩才均, 吴政燮, 黄媛, 等. 肠脂肪酸结合蛋白与肝硬化患者细菌感染和不良预后的相关性研究[J]. 中国感染控制杂志, 2023, 22( 3): 315- 321. DOI: 10.12138/j.issn.1671-9638.20233630. [13] SHI T, YANG JP, ZHANG NL, et al. Comparison and use of explainable machine learning-based survival models for heart failure patients[J]. Digit Health, 2024, 10: 20552076241277027. DOI: 10.1177/20552076241277027. [14] LIANG ZX, YE LS, JIANG P, et al. Explainable machine learning for the assessment of donor grafts in liver transplantation[J]. Hepatol Res, 2025, 55( 6): 908- 921. DOI: 10.1111/hepr.14187. [15] Chinese Society of Hepatology, Chinese Medical Association. Chinese guidelines on the management of liver cirrhosis[J]. J Clin Hepatol, 2019, 35( 11): 2408- 2425. DOI: 10.3969/j.issn.1001-5256.2019.11.006.中华医学会肝病学分会. 肝硬化诊治指南[J]. 临床肝胆病杂志, 2019, 35( 11): 2408- 2425. DOI: 10.3969/j.issn.1001-5256.2019.11.006. [16] FUKUI H. Leaky gut and gut-liver axis in liver cirrhosis: Clinical studies update[J]. Gut Liver, 2021, 15( 5): 666- 676. DOI: 10.5009/gnl20032. [17] TILG H, ADOLPH TE, TRAUNER M. Gut-liver axis: Pathophysiological concepts and clinical implications[J]. Cell Metab, 2022, 34( 11): 1700- 1718. DOI: 10.1016/j.cmet.2022.09.017. [18] QIN N, YANG FL, LI A, et al. Alterations of the human gut microbiome in liver cirrhosis[J]. Nature, 2014, 513( 7516): 59- 64. DOI: 10.1038/nature13568. [19] BAJAJ JS, HEUMAN DM, HYLEMON PB, et al. Altered profile of human gut microbiome is associated with cirrhosis and its complications[J]. J Hepatol, 2014, 60( 5): 940- 947. DOI: 10.1016/j.jhep.2013.12.019. [20] NARDELLI S, GIOIA S, RIDOLA L, et al. Proton pump inhibitors are associated with minimal and overt hepatic encephalopathy and increased mortality in patients with cirrhosis[J]. Hepatology, 2019, 70( 2): 640- 649. DOI: 10.1002/hep.30304. [21] RIVA A, GRAY EH, AZARIAN S, et al. Faecal cytokine profiling as a marker of intestinal inflammation in acutely decompensated cirrhosis[J]. JHEP Rep, 2020, 2( 6): 100151. DOI: 10.1016/j.jhepr.2020.100151. [22] HAN CJ, WU ZX, HUANG Y, et al. Predicting value of intestinal fatty acid-binding protein in esophageal varices in patients with hepatitis B cirrhosis[J]. Chin J Lab Med, 2025, 48( 11): 1446- 1451. DOI: 10.3760/cma.j.cn114452-20250206-00057.韩才均, 吴政燮, 黄媛, 等. 肠型脂肪酸结合蛋白对乙型肝炎肝硬化食管静脉曲张的预测价值[J]. 中华检验医学杂志, 2025, 48( 11): 1446- 1451. DOI: 10.3760/cma.j.cn114452-20250206-00057. [23] LIN XY, LI C, ZHANG T, et al. Changes of intestinal wall barrier function and its correlation with susceptibility to infection in patients with cirrhotic portal hypertension[J]. Chin J Hepatol, 2023, 31( 1): 70- 76. DOI: 10.3760/cma.j.cn501113-20220118-00031.林晓宇, 李琛, 张婷, 等. 肝硬化门静脉高压症患者肠壁屏障功能的改变及其与易发感染的关系[J]. 中华肝脏病杂志, 2023, 31( 1): 70- 76. DOI: 10.3760/cma.j.cn501113-20220118-00031. [24] RAMACHANDRAN A, PRABHU R, THOMAS S, et al. Intestinal mucosal alterations in experimental cirrhosis in the rat: Role of oxygen free radicals[J]. Hepatology, 2002, 35( 3): 622- 629. DOI: 10.1053/jhep.2002.31656. [25] ALBILLOS A, de GOTTARDI A, RESCIGNO M. The gut-liver axis in liver disease: Pathophysiological basis for therapy[J]. J Hepatol, 2020, 72( 3): 558- 577. DOI: 10.1016/j.jhep.2019.10.003. [26] YOKOYAMA S, HONDA T, ISHIZU Y, et al. Utility of MELD 3.0 and MELD-Na in predicting long-term mortality and rebleeding after endoscopic hemostasis for acute variceal hemorrhaging in patients with cirrhosis[J]. Intern Med, 2026, 65( 3): 368- 378. DOI: 10.2169/internalmedicine.5556-25. [27] YOKOYAMA S, HONDA T, ISHIZU Y, et al. Predicting early rebleeding and mortality after endoscopic hemostasis of esophagogastric varices: Diagnostic performance of aspartate aminotransferase-to-platelet ratio index and model for end-stage liver disease-Na score[J]. J Hepatobiliary Pancreat Sci, 2024, 31( 11): 830- 839. DOI: 10.1002/jhbp.12057. -

 本文二维码
本文二维码
计量
- 文章访问数: 183
- HTML全文浏览量: 39
- PDF下载量: 85
- 被引次数: 0

