
 PDF下载 ( 2484 KB)
PDF下载 ( 2484 KB)

代谢指标联合人体测量指标对代谢相关脂肪性肝病及其中高危程度的预测价值及列线图模型构建
DOI: 10.12449/JCH260510
Value of metabolic markers combined with anthropometric indicators in predicting and risk stratification of metabolic dysfunction-associated fatty liver disease and establishment of a nomogram model
-
摘要:
目的 构建基于代谢与人体测量指标的代谢相关脂肪性肝病(MAFLD)临床预测模型,为MAFLD筛查和干预提供更有效的工具。 方法 回顾性纳入2024年1月1日—2025年1月1日于兰州大学第一医院体检中心进行腹部彩超检查的2 824例体检人群为研究对象,将其按7∶3的比例随机分为训练集(n=1 976)和验证集(n=848)。收集研究对象的临床资料、血清学指标及腹部超声结果,计算甘油三酯-葡萄糖(TyG)指数、甘油三酯/高密度脂蛋白胆固醇比值(TG/HDL-C)及多种人体测量指标。符合正态或近似正态分布的计量资料2组间比较采用独立样本t检验,偏态分布的计量资料2组间比较采用Mann-Whitney U检验,计数资料组间比较采用χ2检验或Fisher精确检验。采用多因素Logistic回归分析分别筛选MAFLD及中高危MAFLD的独立相关因素,根据MAFLD的独立影响因素构建5种风险预测模型。绘制受试者操作特征曲线评估模型效能,并计算曲线下面积(AUC)。采用校准曲线评估模型的预测准确性,采用决策曲线分析评估模型的临床实用价值,并与传统模型的性能进行比较。 结果 训练集1 976例体检者中937例(47.42%)为MAFLD,中高危MAFLD有423例(21.41%);验证集848例体检者中MAFLD为 406例(47.88%)。多因素Logistic回归分析显示,男性[比值比(OR)=0.23,95%置信区间(CI):0.13~0.39]、腰围(OR=1.11,95%CI:1.06~1.17)、丙氨酸氨基转移酶(ALT)>40 U/L(OR=2.24,95%CI:1.44~3.51)、高密度脂蛋白胆固醇(OR=0.07,95%CI:0.04~0.15)、TyG指数(OR=8.27,95%CI:5.09~13.44)、TG/HDL-C(OR=0.84,95%CI:0.71~0.99)、身体形态指数(ABSI)(OR=0.45,95%CI:0.39~0.52)及体圆指数(BRI)(OR=2.31,95%CI:1.50~3.55)为MAFLD的独立影响因素(P值均<0.05)。而中高危MAFLD的独立影响因素则包括男性(OR=0.17,95%CI:0.10~0.31)、年龄(OR=1.09,95%CI:1.07~1.11)、血红蛋白(OR=0.98,95%CI:0.97~0.98)、血小板计数(OR=0.81,95%CI:0.70~0.93)、空腹血糖(OR=0.80,95%CI:0.71~0.89)、甘油三酯(OR=0.14,95%CI:0.07~0.29)、TG/HDL-C(OR=0.78,95%CI:0.67~0.91)、TyG指数(OR=5.26,95%CI:3.32~8.33)、腰围(OR=2.50,95%CI:1.72~3.61)、ABSI(OR=0.58,95%CI:0.51~0.66)及BRI指数(OR=0.01,95%CI:0.00~0.21)(P值均<0.05)。在构建的5种预测模型中,模型5(包含性别、ALT升高、HDL-C、TyG指数、TG/HDL-C、腰围和ABSI)表现最优,其在训练集中的AUC为0.917(95%CI:0.905~0.929),验证集中AUC为0.911(95%CI:0.892~0.930)。校准曲线显示模型5具有良好的预测准确性,决策曲线分析证实其具有临床实用价值。 结论 基于代谢指标联合人体测量指标构建的MAFLD预测模型具有良好的判别能力,可用于MAFLD患病风险的评估。此外,本研究发现腰围、TyG指数、TG/HDL-C、ABSI及BRI等指标与中高危MAFLD独立相关,但其对肝纤维化进展的预测价值尚需进一步验证。 -
关键词:
- 代谢相关脂肪性肝病 /
- 危险因素 /
- Logistic 模型
Abstract:Objective To develop a novel clinical predictive model for metabolic dysfunction-associated fatty liver disease (MAFLD) based on metabolic markers and anthropometric indicators, and to provide a more effective tool for the early screening and intervention of MAFLD. Methods A retrospective analysis was performed for 2 824 individuals who underwent abdominal color Doppler ultrasound at Health Examination Center of The First Hospital of Lanzhou University from January 1, 2024 to January 1, 2025, and at a ratio of 7∶3, they were randomly divided into training set with 1 976 patients and validation set with 848 patients. Clinical data, serological markers, and abdominal ultrasound results were collected from all patients, and triglyceride-glucose (TyG) index, triglyceride-to-high-density lipoprotein cholesterol (TG/HDL-C) ratio, and anthropometric indicators were calculated. The independent samples t-test was used for comparison of normally distributed or approximately normally distributed continuous data between two groups, and the Mann-Whitney U test was used for comparison of continuous data with skewed distribution between two groups; the chi-square test or the Fisher’s exact test was used for comparison of categorical data between groups. The multivariate logistic regression analysis was used to identify independent predictive factors for MAFLD and intermediate- to high-risk MAFLD. Five risk prediction models were established for MAFLD based on the independent influencing factors, and a nomogram was plotted. The receiver operating characteristic (ROC) curve was plotted to assess model performance, and the area under the ROC curve (AUC) was calculated. The calibration curve was used to evaluate the predictive accuracy of the models, and decision curve analysis was used to assess the clinical practicability of the models. These models were then compared with traditional models. Results Among the 1 976 individuals in the training set, 937 (47.42%) were diagnosed with MAFLD, and 423 (21.41%) were diagnosed with intermediate- to high-risk MAFLD; among the 848 individuals in the validation set, 406 (47.88%) were diagnosed with MAFLD. The multivariate logistic regression analysis showed that male sex (odds ratio [OR]=0.23, 95% confidence interval [CI]: 0.13 — 0.39, P<0.05), waist circumference (OR=1.11, 95%CI: 1.06 — 1.17, P<0.05), alanine aminotransferase (ALT) >40 U/L (OR=2.24, 95%CI: 1.44 — 3.51, P<0.05), high-density lipoprotein cholesterol (HDL-C) (OR=0.07, 95%CI: 0.04 — 0.15, P<0.05), TyG index (OR=8.27, 95%CI: 5.09 — 13.44, P<0.05), TG/HDL-C ratio (OR=0.84, 95%CI: 0.71 — 0.99, P<0.05), A Body Shape Index (ABSI) (OR=0.45, 95%CI: 0.39 — 0.52, P<0.05), and body roundness index (BRI) (OR=2.31, 95%CI: 1.50 — 3.55, P<0.05) were independent influencing factors for MAFLD, and male sex (OR=0.17, 95%CI: 0.10 — 0.31, P<0.05), age (OR=1.09, 95%CI: 1.07 — 1.11, P<0.05), hemoglobin (OR=0.98, 95%CI: 0.97 — 0.98, P<0.05), platelet count (OR=0.81, 95%CI: 0.70 — 0.93, P<0.05), fasting blood glucose (OR=0.80, 95%CI: 0.71 — 0.89, P<0.05), triglycerides (OR=0.14, 95%CI: 0.07 — 0.29, P<0.05), TG/HDL-C ratio (OR=0.78, 95%CI: 0.67 — 0.91, P<0.05), TyG index (OR=5.26, 95%CI: 3.32 — 8.33), waist circumference (OR=2.50, 95%CI: 1.72 — 3.61, P<0.05), ABSI (OR=0.58, 95%CI: 0.51 — 0.66, P<0.05), and BRI (OR=0.01, 95%CI: 0.00 — 0.21, P<0.05) were independent influencing factors for intermediate- to high-risk MAFLD. Among the five models established, model 5 (incorporating sex, ALT elevation, HDL-C, TyG index, TG/HDL-C ratio, waist circumference, and ABSI) had the best performance, with an AUC of 0.917 (95%CI: 0.905 — 0.929) in the training set and 0.911 (95%CI: 0.892 — 0.930) in the validation set. The calibration curve showed that model 5 had good predictive accuracy, and the decision curve analysis confirmed its clinical practicability. Conclusion The predictive model for MAFLD constructed based on metabolic markers and anthropometric indicators has good discriminatory ability and can be used to assess the risk of MAFLD. In addition, this study shows that waist circumference, TyG index, TG/HDL-C ratio, ABSI, and BRI are independently associated with intermediate- to high-risk MAFLD, but further studies are needed to confirm their value in predicting liver fibrosis progression. -
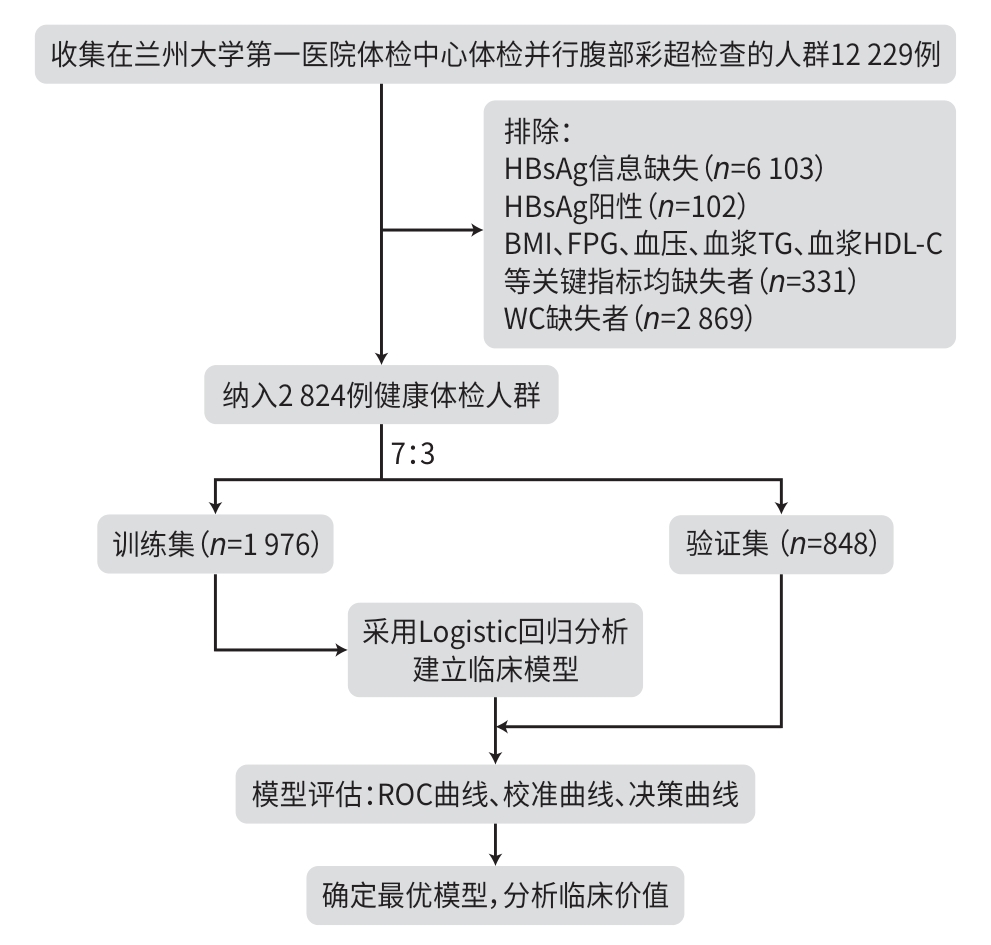
注: HBsAg,乙型肝炎表面抗原;BMI,体重指数;FPG,空腹血糖;TG,甘油三酯;WC,腰围;HDL-C,高密度脂蛋白胆固醇;ROC曲线,受试者操作特征曲线。
图 1 技术路线图
Figure 1. Technical roadmap
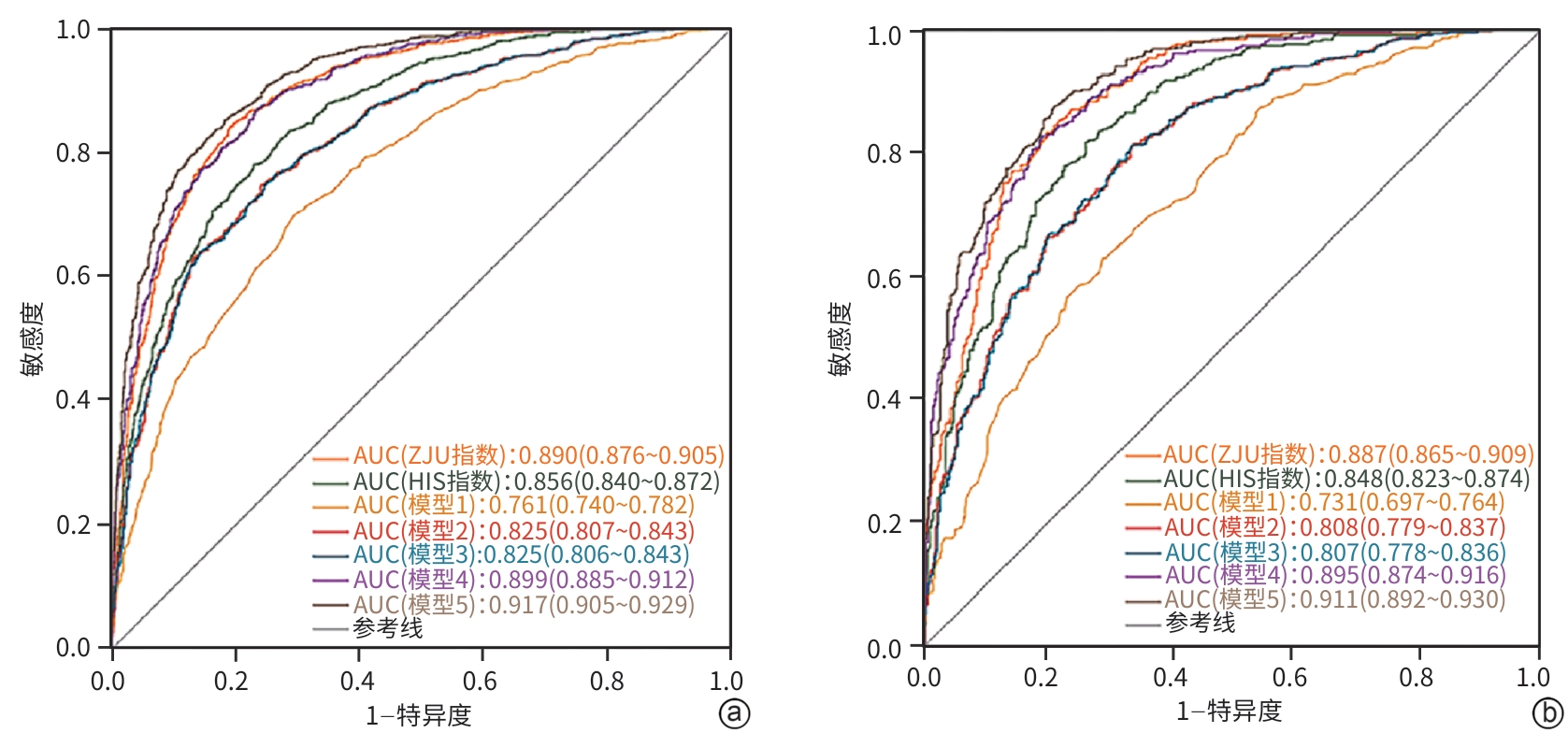
注: a,训练集;b,验证集。ZJU指数浙江大学指数;HIS指数,肝脂肪变性指数;ROC曲线,受试者操作特征曲线;AUC,ROC曲线下面积。
图 2 5种预测模型的ROC曲线
Figure 2. ROC curve analysis of the five prediction models
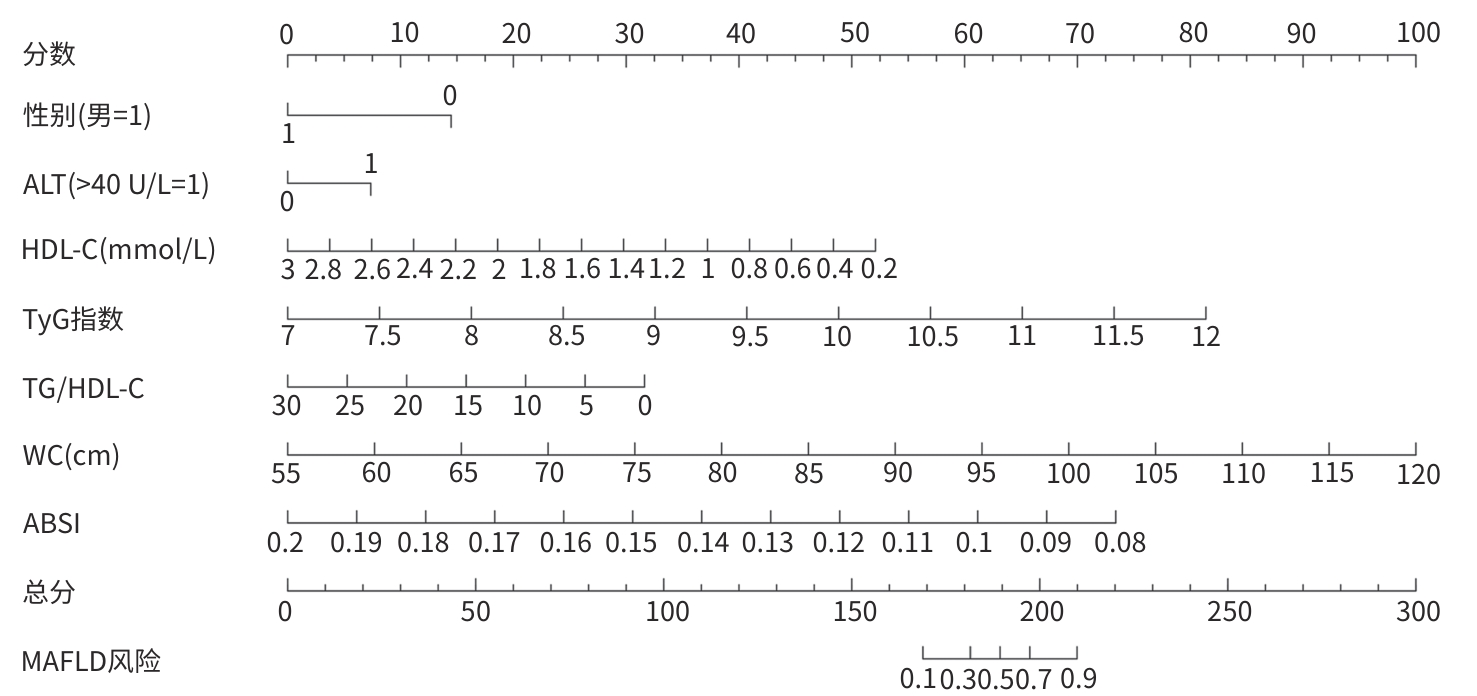
注: TyG指数,甘油三酯-葡萄糖指数;ABSI,身体形态指数;HDL-C,高密度脂蛋白胆固醇;TG,甘油三酯;WC,腰围;ALT,丙氨酸氨基转移酶;MAFLD,代谢相关脂肪性肝病。
图 3 预测模型5的列线图
Figure 3. Nomogram of prediction model 5
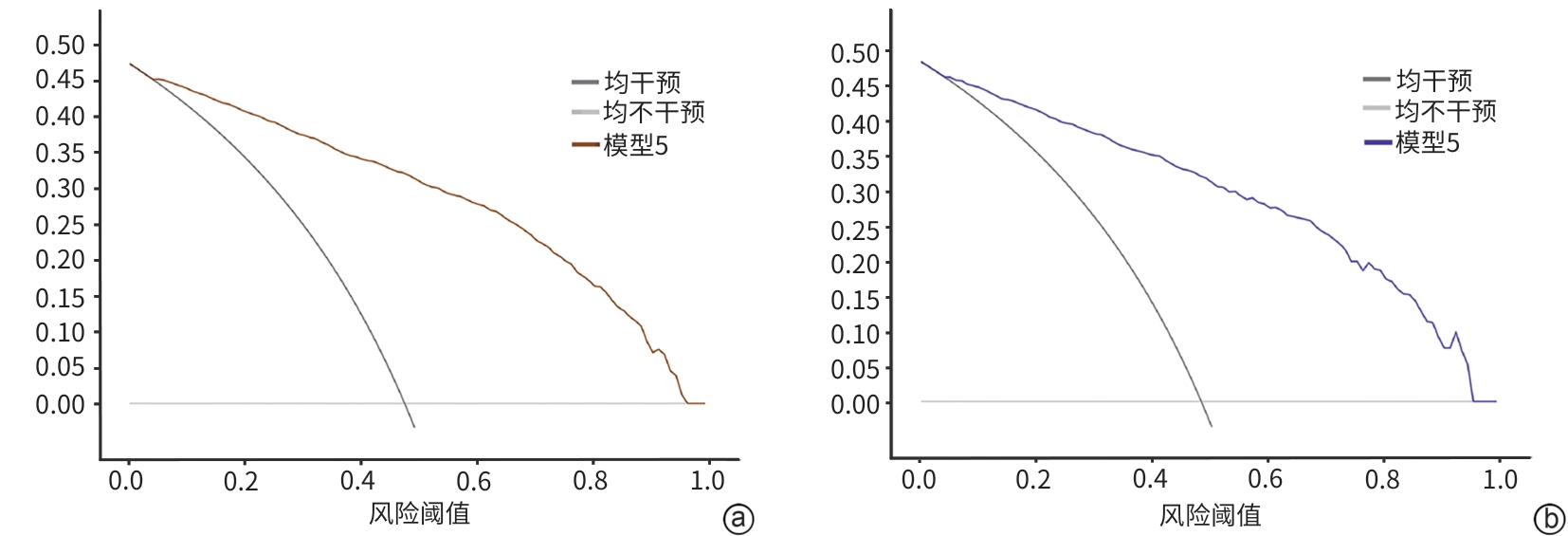
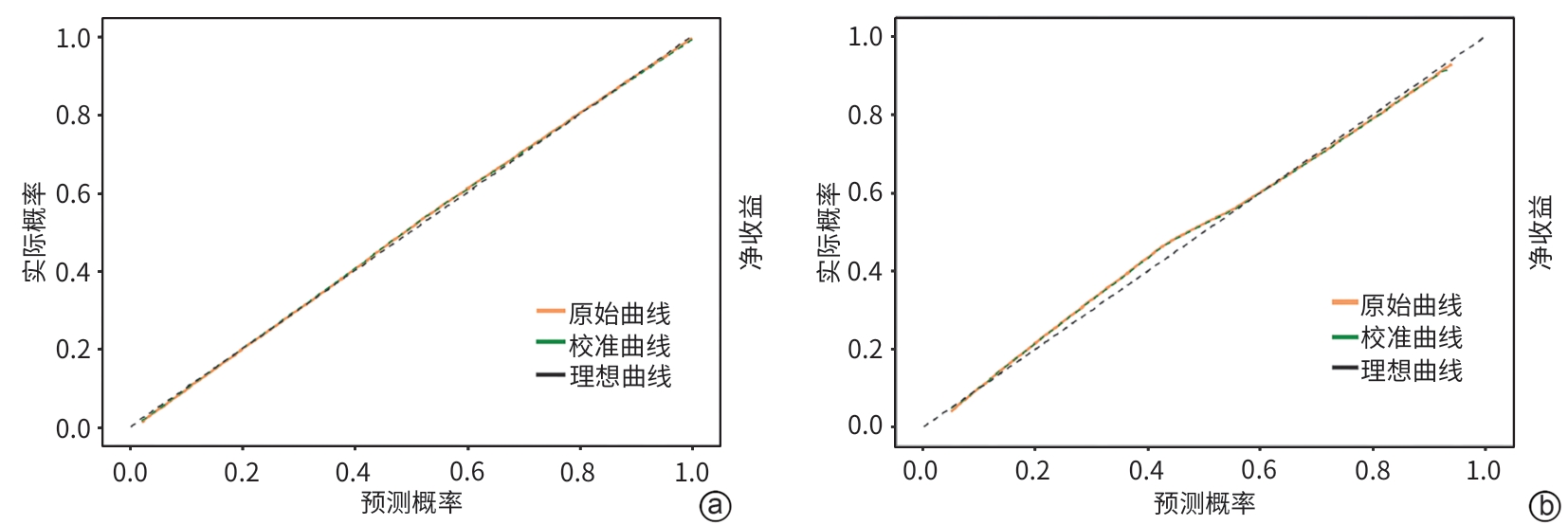
注: a,训练集;b,验证集。
图 5 预测模型5的决策曲线
Figure 5. Decision curve analysis of prediction model 5
表 1 训练集中MAFLD组和非MAFLD组临床资料比较
Table 1. Comparison of clinical data between MAFLD group and non-MAFLD group
项目 总计(n=1 976) 非MAFLD(n=1 039) MAFLD(n=937) 统计值 P值 性别[例(%)] χ2=78.33 <0.001 女 450(22.77) 319(30.70) 131(13.98) 男 1 526(77.23) 720(69.30) 806(86.02) BMI分级[例(%)] χ2=699.93 <0.001 偏瘦 57(2.89) 55(5.30) 2(0.21) 正常 1 061(53.75) 820(79.07) 241(25.72) 超重 773(39.16) 158(15.24) 615(65.64) 肥胖 83(4.20) 4(0.39) 79(8.43) 年龄分层[例(%)] χ2=38.68 <0.001 <30岁 89(4.50) 59(5.68) 30(3.20) 30~39岁 261(13.21) 151(14.53) 110(11.74) 40~49岁 324(16.40) 159(15.30) 165(17.61) 50~59岁 605(30.62) 305(29.36) 300(32.02) 60~69岁 469(23.73) 218(20.98) 251(26.79) 70~79岁 149(7.54) 87(8.37) 62(6.61) ≥80岁 79(4.00) 60(5.78) 19(2.03) 血红蛋白(g/L) 154.45±15.08 151.10±15.40 158.17±13.80 t=-10.77 <0.001 WC(cm) 88.0(80.0~93.0) 82.0(76.0~88.0) 92.0(88.0~98.0) Z=-25.21 <0.001 血小板计数(×109/L) 207.0(174.0~242.0) 208.0(174.5~241.0) 206.0(174.0~242.0) Z=-0.08 0.935 中性粒细胞绝对值(×109/L) 3.40(2.76~4.14) 3.22(2.55~3.96) 3.61(2.96~4.37) Z=-8.71 <0.001 白细胞计数(×109/L) 5.92(4.98~6.92) 5.63(4.70~6.62) 6.27(5.32~7.33) Z=-9.87 <0.001 ALT>40 U/L[例(%)] χ2=111.16 <0.001 否 1 700(86.03) 975(93.84) 725(77.37) 是 276(13.97) 64(6.16) 212(22.63) AST>40 U/L[例 (%)] χ2=27.93 <0.001 否 1 909(96.61) 1 025(98.65) 884(94.34) 是 67(3.39) 14(1.35) 53(5.66) 血清尿酸(μmol/L) 370(315~426) 341(291~401) 397(349~449) Z=-13.94 <0.001 FPG(mmol/L) 5.34(4.99~5.87) 5.17(4.89~5.61) 5.52(5.16~6.07) Z=-11.50 <0.001 TG(mmol/L) 1.40(1.02~1.98) 1.15(0.88~1.48) 1.82(1.31~2.46) Z=-20.68 <0.001 HDL-C(mmol/L) 1.17(1.02~1.38) 1.28(1.12~1.48) 1.07(0.95~1.22) Z=-18.33 <0.001 LDL-C(mmol/L) 2.86(2.35~3.37) 2.76(2.27~3.25) 2.98(2.45~3.49) Z=-5.50 <0.001 TyG指数 8.72(8.38~9.09) 8.51(8.21~8.78) 9.02(8.67~9.38) Z=-21.28 <0.001 TG/HDL-C 1.19(0.79~1.82) 0.91(0.63~1.25) 1.69(1.18~2.35) Z=-23.40 <0.001 NHR 2.88(2.15~3.84) 2.50(1.86~3.31) 3.37(2.60~4.31) Z=-15.87 <0.001 UHR 13.66(10.54~17.29) 11.58(8.95~14.67) 16.01(13.13~19.22) Z=-19.90 <0.001 WWI 10.38(9.97~10.76) 10.19(9.77~10.62) 10.53(10.21~10.84) Z=-12.45 <0.001 ABSI 0.12(0.12~0.13) 0.12(0.11~0.12) 0.13(0.12~0.13) Z=-18.05 <0.001 TyG-WC指数 766.96(689.44~836.35) 701.99(632.30~763.06) 832.19(778.80~884.79) Z=-28.35 <0.001 BRI 3.63(3.00~4.23) 3.15(2.60~3.64) 4.14(3.68~4.69) Z=-25.48 <0.001 注:MAFLD,代谢相关脂肪性肝病;BMI,体重指数;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;WC,腰围;FPG,空腹血糖;TG,甘油三酯;HDL-C,高密度脂蛋白胆固醇;LDL-C,低密度脂蛋白胆固醇;TyG指数,甘油三酯-葡萄糖指数;NHR,中性粒细胞/高密度脂蛋白胆固醇比值;UHR,血清尿酸/高密度脂蛋白胆固醇比值;WWI,体重调整腰围指数;ABSI,身体形态指数;BRI,体圆指数。
 下载: 导出CSV
下载: 导出CSV
表 2 代谢及炎症相关因素与MAFLD关联的单因素及多因素回归分析
Table 2. Univariate and multivariate regression analysis of the association between metabolic and inflammatory factors and MAFLD
项目 单因素分析 多因素分析 OR(95%CI) P值 OR(95%CI) P值 男性 2.73(2.17~3.42) <0.001 0.23(0.13~0.39) <0.001 年龄 1.00(0.99~1.01) 0.682 BMI 1.90(1.79~2.01) <0.001 WC 1.19(1.17~1.21) <0.001 1.11(1.06~1.17) <0.001 血红蛋白 1.03(1.03~1.04) <0.001 1.00(0.99~1.01) 0.682 中性粒细胞绝对值 1.39(1.28~1.51) <0.001 1.12(0.85~1.46) 0.425 白细胞计数 1.34(1.26~1.43) <0.001 0.92(0.74~1.13) 0.428 ALT>40 U/L 4.45(3.31~5.99) <0.001 2.24(1.44~3.51) <0.001 AST>40 U/L 4.39(2.42~7.96) <0.001 1.57(0.62~4.03) 0.343 血清尿酸 1.01(1.01~1.01) <0.001 1.00(1.00~1.00) 0.255 FPG 1.36(1.25~1.49) <0.001 0.91(0.80~1.04) 0.164 TG 3.84(3.26~4.52) <0.001 HDL-C 0.03(0.02~0.05) <0.001 0.07(0.04~0.15) <0.001 LDL-C 1.32(1.18~1.48) <0.001 1.13(0.94~1.35) 0.199 TyG指数 9.08(7.16~11.50) <0.001 8.27(5.09~13.44) <0.001 TG/HDL-C 3.99(3.40~4.69) <0.001 0.84(0.71~0.99) 0.041 NHR 1.77(1.63~1.92) <0.001 UHR 1.23(1.20~1.26) <0.001 WWI 2.66(2.25~3.13) <0.001 ABSI 1.02(1.02~1.03) <0.001 0.45(0.39~0.52) <0.001 TyG-WC指数 1.02(1.02~1.02) <0.001 BRI 5.68(4.82~6.71) <0.001 2.31(1.50~3.55) <0.001 注:MAFLD,代谢相关脂肪性肝病;OR,比值比;CI,置信区间;BMI,体重指数;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;WC,腰围;FPG,空腹血糖;TG,甘油三酯;HDL-C,高密度脂蛋白胆固醇;LDL-C,低密度脂蛋白胆固醇;TyG指数,甘油三酯-葡萄糖指数;NHR,中性粒细胞/高密度脂蛋白胆固醇比值;UHR,血清尿酸/高密度脂蛋白胆固醇比值;WWI,体重调整腰围指数;ABSI,身体形态指数;BRI,体圆指数。分类变量赋值方式:性别(女性=0,男性=1)、ALT>40 U/L(否=0,是=1)、AST>40 U/L(否=0,是=1);连续型变量均以原值纳入模型。
下载: 导出CSV
表 3 代谢及炎症相关因素与中高危MAFLD关联的单因素及多因素Logistic回归分析
Table 3. Univariate and multivariate Logistic regression analysis of clinical and biochemical factors associated withmedium/high-risk MAFLD
项目 单因素分析 多因素分析 OR(95%CI) P值 OR(95%CI) P值 男性 1.82(1.36~2.42) <0.001 0.17(0.10~0.31) <0.001 年龄 1.07(1.06~1.08) <0.001 1.09(1.07~1.11) <0.001 BMI 1.29(1.24~1.34) <0.001 0.62(0.33~1.19) 0.154 WC 1.10(1.09~1.12) <0.001 2.50(1.72~3.61) <0.001 血红蛋白 1.01(1.01~1.02) 0.007 0.98(0.97~0.98) <0.001 血小板计数 0.98(0.98~0.98) <0.001 0.81(0.70~0.93) 0.003 中性粒细胞绝对值 1.01(0.92~1.10) 0.891 白细胞计数 0.99(0.93~1.06) 0.786 血清尿酸 1.01(1.01~1.01) <0.001 1.00(1.00~1.00) 0.888 FPG 1.29(1.19~1.40) <0.001 0.80(0.71~0.89) <0.001 TG 1.26(1.15~1.37) <0.001 0.14(0.07~0.29) <0.001 HDL-C 0.16(0.10~0.25) <0.001 1.02(0.86~1.20) 0.836 LDL-C 0.91(0.79~1.04) 0.160 TyG指数 2.46(2.03~2.98) <0.001 5.26(3.32~8.33) <0.001 TG/HDL-C 1.23(1.13~1.33) <0.001 0.78(0.67~0.91) 0.001 NHR 1.16(1.07~1.24) <0.001 0.93(0.82~1.04) 0.207 UHR 1.08(1.06~1.10) <0.001 WWI 3.04(2.49~3.72) <0.001 ABSI 1.01(1.01~1.02) <0.001 0.58(0.51~0.66) <0.001 TyG-WC指数 1.01(1.01~1.01) <0.001 BRI 2.61(2.33~2.91) <0.001 0.01(0.00~0.21) 0.002 ALT>40 U/L 1.18(0.88~1.60) 0.276 AST>40 U/L 2.52(1.67~3.81) <0.001 注:MAFLD,代谢相关性脂肪性肝病;OR,比值比;CI,置信区间;BMI,体重指数;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;WC,腰围;FPG,空腹血糖;TG,甘油三酯;HDL-C,高密度脂蛋白胆固醇;LDL-C,低密度脂蛋白胆固醇;TyG指数,甘油三酯-葡萄糖指数;NHR,中性粒细胞/高密度脂蛋白胆固醇比值;UHR,血清尿酸/高密度脂蛋白胆固醇比值;WWI,体重调整腰围指数;ABSI,身体形态指数;BRI,体圆指数。分类变量赋值方式:性别(女性=0,男性=1)、ALT > 40 U/L(否=0,是=1)、AST > 40 U/L(否=0,是=1);连续型变量均以原值纳入模型。
下载: 导出CSV
表 4 5种临床模型在训练集中的AUC、敏感度和特异度分析
Table 4. Analysis of AUC, sensitivity, and specificity of five clinical models in the training dataset
预测因子 AUC(95%CI) 截断值 敏感度 特异度 Z值1) P值1) ZJU指数 0.890(0.876~0.905) 0.456 0.828 0.812 HIS指数 0.856(0.840~0.872) 0.450 0.783 0.766 8.356 <0.001 模型1 0.761(0.740~0.782) 0.486 0.696 0.702 11.339 <0.001 模型2 0.825(0.807~0.843) 0.477 0.748 0.757 7.367 <0.001 模型3 0.825(0.806~0.843) 0.481 0.752 0.747 7.448 <0.001 模型4 0.899(0.885~0.912) 0.409 0.867 0.767 -0.580 0.562 模型5 0.917(0.905~0.929) 0.451 0.852 0.816 -4.738 <0.001 注:1)与ZJU指数比较。AUC,受试者操作特征曲线下面积;CI,置信区间;ZJU指数,浙江大学指数;HIS指数,肝脂肪变性指数。
下载: 导出CSV
表 5 5种临床模型在验证集中的AUC、敏感度和特异度分析
Table 5. Analysis of AUC, sensitivity, and specificity of five clinical models in the validation dataset
预测因子 AUC(95%CI) 截断值 敏感度 特异度 Z值1) P值1) ZJU指数 0.887(0.865~0.909) 0.454 0.823 0.807 HIS指数 0.848(0.823~0.874) 0.399 0.813 0.735 4.997 <0.001 模型1 0.731(0.697~0.764) 0.518 0.631 0.707 8.877 <0.001 模型2 0.808(0.779~0.837) 0.417 0.810 0.665 5.938 <0.001 模型3 0.807(0.778~0.836) 0.422 0.810 0.665 6.030 <0.001 模型4 0.895(0.874~0.916) 0.470 0.825 0.809 -0.473 0.636 模型5 0.911(0.892~0.930) 0.425 0.873 0.791 -2.842 0.004 注:1)与ZJU指数比较。AUC,受试者操作特征曲线下面积;CI,置信区间;ZJU指数,浙江大学指数;HIS指数,肝脂肪变性指数。
下载: 导出CSV
-
[1] YOUNOSSI ZM, GOLABI P, PAIK JM, et al. The global epidemiology of nonalcoholic fatty liver disease(NAFLD) and nonalcoholic steatohepatitis(NASH): A systematic review[J]. Hepatology, 2023, 77( 4): 1335- 1347. DOI: 10.1097/HEP.0000000000000004. [2] TARGHER G, COREY KE, BYRNE CD, et al. The complex link between NAFLD and type 2 diabetes mellitus- mechanisms and treatments[J]. Nat Rev Gastroenterol Hepatol, 2021, 18( 9): 599- 612. DOI: 10.1038/s41575-021-00448-y. [3] BYRNE CD, TARGHER G. NAFLD: A multisystem disease[J]. J Hepatol, 2015, 62( 1): S47- S64. DOI: 10.1016/j.jhep.2014.12.012. [4] LI J, ZOU BY, YEO YH, et al. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999-2019: A systematic review and meta-analysis[J]. Lancet Gastroenterol Hepatol, 2019, 4( 5): 389- 398. DOI: 10.1016/S2468-1253(19)30039-1. [5] ESTES C, RAZAVI H, LOOMBA R, et al. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease[J]. Hepatology, 2018, 67( 1): 123- 133. DOI: 10.1002/hep.29466. [6] ESLAM M, NEWSOME PN, SARIN SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement[J]. J Hepatol, 2020, 73( 1): 202- 209. DOI: 10.1016/j.jhep.2020.03.039. [7] ZHENG KY, YIN YZ, GUO H, et al. Association between the ZJU index and risk of new-onset non-alcoholic fatty liver disease in non-obese participants: A Chinese longitudinal prospective cohort study[J]. Front Endocrinol, 2024, 15: 1340644. DOI: 10.3389/fendo.2024.1340644. [8] LIU J, DUAN SJ, WANG C, et al. Optimum non-invasive predictive indicators for metabolic dysfunction-associated fatty liver disease and its subgroups in the Chinese population: A retrospective case-control study[J]. Front Endocrinol, 2022, 13: 1035418. DOI: 10.3389/fendo.2022.1035418. [9] XUE Y, XU JH, LI M, et al. Potential screening indicators for early diagnosis of NAFLD/MAFLD and liver fibrosis: Triglyceride glucose index-related parameters[J]. Front Endocrinol, 2022, 13: 951689. DOI: 10.3389/fendo.2022.951689. [10] COLANTONI A, BUCCI T, COCOMELLO N, et al. Lipid-based insulin-resistance markers predict cardiovascular events in metabolic dysfunction associated steatotic liver disease[J]. Cardiovasc Diabetol, 2024, 23( 1): 175. DOI: 10.1186/s12933-024-02263-6. [11] GRAUPERA I, THIELE M, SERRA-BURRIEL M, et al. Low accuracy of FIB-4 and NAFLD fibrosis scores for screening for liver fibrosis in the population[J]. Clin Gastroenterol Hepatol, 2022, 20( 11): 2567- 2576. e 6. DOI: 10.1016/j.cgh.2021.12.034. [12] Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of metabolic dysfunction-associated(non-alcoholic) fatty liver disease(version 2024)[J]. J Prac Hepatol, 2024, 27( 4): 494- 510. DOI: 10.3760/cma.j.cn501113-20240327-00163.中华医学会肝病学分会. 代谢相关(非酒精性)脂肪性肝病防治指南(2024年版)[J]. 实用肝脏病杂志, 2024, 27( 4): 494- 510. DOI: 10.3760/cma.j.cn501113-20240327-00163. [13] LIU Z, HE H, DAI Y, et al. Comparison of the diagnostic value between triglyceride-glucose index and triglyceride to high-density lipoprotein cholesterol ratio in metabolic-associated fatty liver disease patients: A retrospective cross-sectional study[J]. Lipids Health Dis, 2022, 21( 1): 55. DOI: 10.1186/s12944-022-01661-7. [14] JIANG LN, ZHAO JM. Pathological mechanism of multi-organ injuries in metabolic dysfunction-associated fatty liver disease[J]. J Clin Hepatol, 2025, 41( 9): 1729- 1736. DOI: 10.12449/JCH250903.蒋丽娜, 赵景民. 代谢相关脂肪性肝病多器官损伤的病理机制[J]. 临床肝胆病杂志, 2025, 41( 9): 1729- 1736. DOI: 10.12449/JCH250903. [15] ZHANG C, ZHU PH, HE LL. Research progress on the correlation between metabolic associated fatty liver disease and cardiovascular disease risk[J/CD]. Chin J Liver Dis(Electronic Version), 2025, 17( 1): 12- 18. DOI: 10.3969/j.issn.1674-7380.2025.01.003.张成, 朱平辉, 何玲玲. 代谢相关脂肪性肝病与心血管疾病风险相关性研究现状[J/CD]. 中国肝脏病杂志(电子版), 2025, 17( 1): 12- 18. DOI: 10.3969/j.issn.1674-7380.2025.01.003. [16] FAHAMI M, HOJATI A, FARHANGI MA. Body shape index(ABSI), body roundness index(BRI) and risk factors of metabolic syndrome among overweight and obese adults: A cross-sectional study[J]. BMC Endocr Disord, 2024, 24( 1): 230. DOI: 10.1186/s12902-024-01763-6. [17] KRAKAUER NY, KRAKAUER JC. A new body shape index predicts mortality hazard independently of body mass index[J]. PLoS One, 2012, 7( 7): e39504. DOI: 10.1371/journal.pone.0039504. [18] ENG PC, DER TEO AE, LEOW MKS, et al. Body roundness index(BRI) and obesity-related anthropometrics: Relationship to visceral adiposity, insulin sensitivity index and cardiometabolic risk[J]. Diabetes Obes Metab, 2025, 27( 10): 5554- 5565. DOI: 10.1111/dom.16601. [19] WANG HY, ZHANG YX, LIU YP, et al. Comparison between traditional and new obesity measurement index for screening metabolic associated fatty liver disease[J]. Front Endocrinol, 2023, 14: 1163682. DOI: 10.3389/fendo.2023.1163682. [20] van EYCK A, KWANTEN WJ, PELEMAN C, et al. The role of adipose tissue and subsequent liver tissue hypoxia in obesity and early stage metabolic dysfunction associated steatotic liver disease[J]. Int J Obes, 2024, 48( 4): 512- 522. DOI: 10.1038/s41366-023-01443-w. [21] WU ZY, ZHOU D, LIU Y, et al. Association of TyG index and TG/HDL-C ratio with arterial stiffness progression in a non-normotensive population[J]. Cardiovasc Diabetol, 2021, 20( 1): 134. DOI: 10.1186/s12933-021-01330-6. [22] YANG B, ZHANG R. Progress on the treatment of metabolic associated fatty liver disease[J/CD]. Chin J Liver Dis(Electronic Version), 2024, 16( 4): 25- 30. DOI: 10.3969/j.issn.1674-7380.2024.04.004.杨彬, 张瑞. 代谢相关脂肪性肝病治疗进展[J/CD]. 中国肝脏病杂志(电子版), 2024, 16( 4): 25- 30. DOI: 10.3969/j.issn.1674-7380.2024.04.004. [23] XU MJ, WEI YS, YE LY, et al. Novel obesity and metabolic indices better predict non-alcoholic fatty liver disease in elderly T2DM patients: Evidence from cross-sectional and longitudinal analysis[J]. Front Med, 2025, 12: 1649466. DOI: 10.3389/fmed.2025.1649466. [24] ZHANG F, HAN Y, MAO YH, et al. Non-invasive prediction nomogram for predicting significant fibrosis in patients with metabolic-associated fatty liver disease: A cross-sectional study[J]. Ann Med, 2024, 56( 1): 2337739. DOI: 10.1080/07853890.2024.2337739. [25] HUANG X, LUO YK, DING YQ, et al. Research on the exploration and implementation effectiveness of ultrasound medicine based teaching measures for pairing assistance in county-level hospitals in Xinjiang[J]. Chin J Disaster Med, 2025, 12( 5): 541- 545. DOI: 10.13919/j.issn.2095-6274.ZHJY202500000.黄鑫, 罗渝昆, 丁益强, 等. 基于超声医学的对口帮扶新疆县级医院教学措施探索与实施成效研究[J]. 中华灾害救援医学, 2025, 12( 5): 541- 545. DOI: 10.13919/j.issn.2095-6274.ZHJY202500000. -

 本文二维码
本文二维码
计量
- 文章访问数: 250
- HTML全文浏览量: 51
- PDF下载量: 89
- 被引次数: 0

