
 PDF下载 ( 1297 KB)
PDF下载 ( 1297 KB)

代谢相关脂肪性肝病与动脉粥样硬化性心血管疾病发病风险的相互影响
DOI: 10.12449/JCH260414
Bidirectional association between metabolic associated fatty liver disease and the risk of atherosclerotic cardiovascular disease
-
摘要:
目的 探讨代谢相关脂肪性肝病(MAFLD)与动脉粥样硬化性心血管疾病(ASCVD)发病风险之间的关联,为临床此类代谢相关疾病防治提供数据支持。 方法 以2006年6月—2007年10月参加首次健康体检,且肝脏评估资料完整、既往无恶性肿瘤病史以及无MAFLD病史或ASCVD病史的开滦职工为观察队列。根据是否患有MAFLD将患者分为非MAFLD组(n=67 565)和MAFLD组(n=29 004);根据是否患有ASCVD将患者分为非ASCVD组(n=69 141)和ASCVD组(n=481)。计量资料两组间比较采用成组t检验或Wilcoxon 秩和检验。计数资料两组间比较采用χ2检验。采用寿命表法计算ASCVD及MAFLD的累积发病率,通过Kaplan-Meier法绘制MAFLD组与非MAFLD组ASCVD累积发病率的生存曲线及ASCVD组与非ASCVD组MAFLD累积发病率的生存曲线,并使用Log-rank检验比较两组患者累积发病率的差异。采用多因素Cox比例风险回归模型分析MAFLD对ASCVD发病风险的影响及ASCVD对MAFLD发病风险的影响。 结果 MAFLD组体重指数(BMI)、腰围、收缩压(SBP)、舒张压(DBP)、静息心率、丙氨酸氨基转移酶(ALT)、尿酸(UA)、空腹血糖(FBG)、甘油三酯(TG)、总胆固醇(TC)、低密度脂蛋白胆固醇(LDL-C)和超敏C反应蛋白(hs-CRP)等均高于非MAFLD组,估算肾小球滤过率(eGFR)、高密度脂蛋白胆固醇等均低于非MAFLD组,差异均有统计学意义(P值均<0.05);ASCVD组BMI、腰围、SBP、DBP、UA、FBG、TG、hs-CRP等均显著高于非ASCVD组,eGFR显著低于非ASCVD组(P值均<0.05)。随着时间的增长,MAFLD组与非MAFLD组ASCVD的累积发病率持续上升;而ASCVD组与非ASCVD组MAFLD的累积发病率先随时间增长,随后趋于平稳。MAFLD组新发ASCVD为4 263例(14.70%),发病密度为12.90/千人年;非MAFLD组新发ASCVD为6 529例(9.66%),发病密度为8.24/千人年,两组ASCVD的发病密度和累积发病率比较,差异均有统计学意义( 结论 MAFLD与ASCVD发病风险存在显著关联,MAFLD人群的ASCVD发病风险升高,而ASCVD人群的MAFLD发病风险降低。 Abstract:Objective To investigate the association between metabolic associated fatty liver disease (MAFLD) and the risk of atherosclerotic cardiovascular disease (ASCVD), and to provide data support for the prevention and treatment of such metabolic-associated diseases in clinical practice. Methods An observation cohort was established for the workers of Kailuan who underwent physical examination for the first time from June 2006 to October 2007 and had complete liver assessment data, without the history of malignant tumor, MAFLD or ASCVD. According to the presence or absence of MAFLD, the patients were divided into non-MAFLD group with 67 565 patients and MAFLD group with 29 004 patients, and according to the presence or absence of ASCVD, the patients were divided into non-ASCVD group with 69 141 patients and ASCVD group with 481 patients. The group t-test or the Wilcoxon rank-sum test was used for comparison of continuous data between the two groups. The Results Compared with the non-MAFLD group, the MAFLD group had significantly higher levels of body mass index (BMI), waist circumference, systolic blood pressure (SBP), diastolic blood pressure (DBP), resting heart rate, alanine aminotransferase, uric acid (UA), fasting blood glucose (FBG), triglyceride (TG), total cholesterol, low-density lipoprotein cholesterol, and high sensitivity C-reactive protein (hs-CRP), as well as significanty lower levels of estimated glomerular filtration rate (eGFR) and high-density lipoprotein cholesterol (all P <0.05). Compared with the non-ASCVD group, the ASCVD group had significantly higher levels of BMI, waist circumference, SBP, DBP, UA, FBG, TG, and hs-CRP and a significantly lower level of eGFR (all P<0.05). The incidence rate of new-onset ASCVD continued to increase over time in the MAFLD group and the non-MAFLD group, while the incidence rate of new-onset MAFLD firstly increased and then remained stable over time in the ASCVD group and the non-ASCVD group. There were 4 263 cases (14.70%) of new-osnet ASCVD in the MAFLD group, with an incidence density of 12.90 per 1 000 person-years, while there were 6 529 cases (9.66%) of new-osnet ASCVD in the non-MAFLD group, with an incidence density of 8.24 per 1 000 person-years, and there were significant differences in the incidence density and cumulative incidence rate of ASCVD between the two groups ( Conclusion There is a significant association between MAFLD and ASCVD, with an increase in the risk of ASCVD in the MAFLD population and a reduction in the risk of MAFLD in the ASCVD population. -
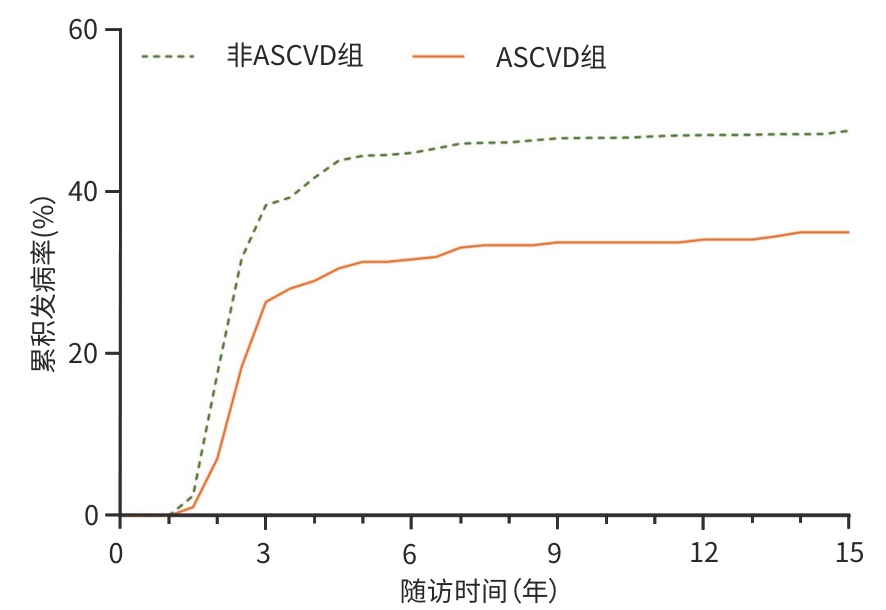
注: MAFLD,代谢相关脂肪性肝病;ASCVD,动脉粥样硬化性心血管疾病。
图 1 MAFLD组与非MAFLD组ASCVD累积发病率的生存曲线
Figure 1. Survival curves of cumulative incidence of new-onset ASCVD in MAFLD group and non-MAFLD group
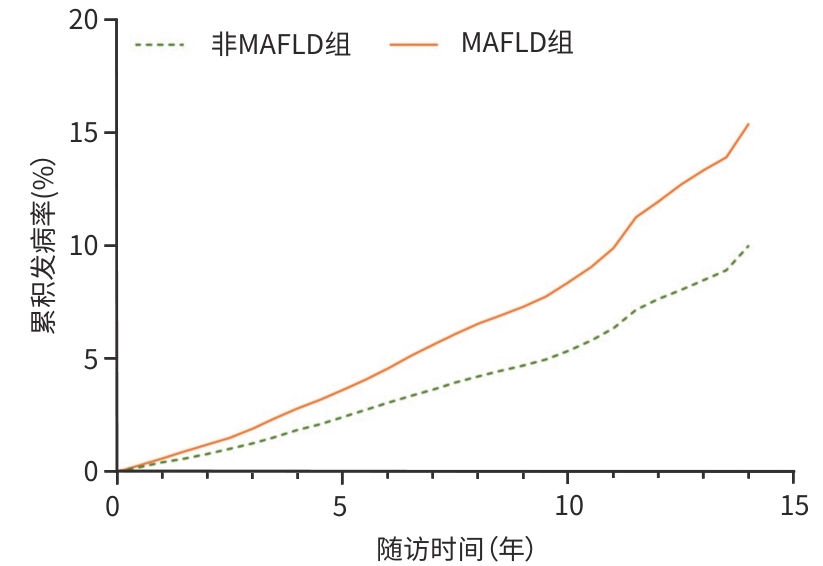
注: MAFLD,代谢相关脂肪性肝病;ASCVD,动脉粥样硬化性心血管疾病。
图 2 ASCVD组与非ASCVD组MAFLD累积发病率的生存曲线
Figure 2. Survival curves of cumulative incidence of new-onset MAFLD in ASCVD group and non-ASCVD group
表 1 MAFLD组与非MAFLD组临床基本特征比较
Table 1. Comparison of basic clinical characteristics between MAFLD and non-MAFLD groups
项目 总人群(n=96 569) MAFLD组(n=29 004) 非MAFLD组(n=67 565) 统计值 P值 年龄(岁) 51.48±12.57 52.32±11.42 51.11±13.02 t=-13.73 <0.001 BMI(kg/m2) 25.02±3.49 27.61±3.06 23.91±3.05 t=-172.26 <0.001 腰围(cm) 86.96±10.04 92.75±8.74 84.47±9.52 t=-126.90 <0.001 SBP(mmHg) 130.68±20.90 137.06±20.83 127.94±20.32 t=-63.43 <0.001 DBP(mmHg) 83.40±11.77 87.31±11.80 81.73±11.35 t=-69.30 <0.001 静息心率(次/min) 73.80±10.17 74.56±10.28 73.47±10.11 t=-15.26 <0.001 ALT(U/L) 18.00(13.00~25.00) 22.00(16.00~30.00) 17.00(12.00~23.00) Z=80.48 <0.001 UA(μmol/L) 288.95±83.65 311.67±90.03 279.20±78.77 t=-56.19 <0.001 eGFR(mL·min-1·1.73 m-2) 82.30±25.79 80.65±25.10 83.01±26.05 t=13.02 <0.001 FBG(mmol/L) 5.47±1.67 5.91±2.04 5.28±1.44 t=-54.26 <0.001 TG(mmol/L) 1.27(0.89~1.93) 1.76(1.22~2.65) 1.13(0.81~1.62) Z=105.79 <0.001 TC(mmol/L) 4.95±1.15 5.10±1.24 4.88±1.10 t=-28.22 <0.001 HDL-C(mmol/L) 1.55±0.40 1.53±0.41 1.56±0.40 t=9.71 <0.001 LDL-C(mmol/L) 2.34±0.91 2.38±0.92 2.33±0.91 t=-9.05 <0.001 hs-CRP(mg/L) 0.83(0.30~2.34) 1.21(0.50~3.12) 0.70(0.26~2.00) Z=51.98 <0.001 男性[例(%)] 76 835(79.56) 23 773(81.96) 53 062(78.53) <0.001 高中及以上教育程度[例(%)] 19 336(20.02) 5 544(19.11) 13 792(20.41) <0.001 月人均收入≥800元[例(%)] 69 073(71.53) 21 082(72.69) 47 991(71.03) <0.001 体育锻炼[例(%)] 88 264(91.40) 26 649(91.88) 61 615(91.19) 0.023 吸烟史[例(%)] 32 902(34.07) 10 016(34.53) 22 886(33.87) 0.139 饮酒史[[例(%)] 35 946(37.22) 11 318(39.02) 24 628(36.45) <0.001 糖尿病史[例(%)] 9 312(9.64) 5 012(17.28) 4 300(6.36) <0.001 高血压史[例(%)] 42 007(43.50) 16 968(58.50) 25 039(37.06) <0.001 血脂异常[例(%)] 57 444(59.48) 21 642(74.62) 35 802(52.99) <0.001 服降糖药[例(%)] 2 557(2.65) 1 585(5.46) 972(1.44) <0.001 服降压药[例(%)] 8 338(8.63) 4 038(13.92) 4 300(6.36) <0.001 服降脂药[例(%)] 7 162(7.42) 3 412(11.76) 3 750(5.55) <0.001 注:BMI,体重指数;SBP,收缩压;DBP,舒张压;ALT,丙氨酸氨基转移酶;UA,尿酸;eGFR,估算肾小球滤过率;FBG,空腹血糖;TG,甘油三酯;TC,总胆固醇;HDL-C,高密度脂蛋白胆固醇;LDL-C,低密度脂蛋白胆固醇;hs-CRP,超敏C反应蛋白;MAFLD,代谢相关脂肪性肝病。
 下载: 导出CSV
下载: 导出CSV
表 2 ASCVD组与非ASCVD组临床基本特征比较
Table 2. Comparison of basic clinical characteristics between ASCVD and non-ASCVD groups
项目 总人群(n=69 622) ASCVD组(n=481) 非ASCVD组(n=69 141) 统计值 P值 年龄(岁) 51.49±13.11 63.29±10.50 51.40±13.09 t=-19.87 <0.001 BMI(kg/m2) 23.92±3.05 24.64±3.15 23.92±3.05 t=-5.18 <0.001 腰围(cm) 84.53±9.50 88.19±8.86 84.51±9.50 t=-8.48 <0.001 SBP(mmHg) 128.32±20.52 143.40±24.20 128.21±20.45 t=-16.21 <0.001 DBP(mmHg) 81.81±11.37 86.88±12.50 81.77±11.35 t=-9.81 <0.001 静息心率(次/min) 73.46±10.11 73.88±10.70 73.46±10.11 t=-0.91 0.664 ALT(U/L) 17.00(12.00~22.90) 17.00(12.00~22.20) 17.00(12.00~22.92) t=-1.39 0.382 UA(μmol/L) 280.39±76.38 320.87±93.34 280.10±79.20 t=-11.24 <0.001 eGFR(mL·min-1·1.73 m-2) 82.69±25.91 74.82±30.18 82.75±25.87 t=6.69 <0.001 FBG(mmol/L) 5.29±1.46 5.90±2.38 5.28±1.45 t=-9.23 <0.001 TG(mmol/L) 1.13(0.81~1.62) 1.24(0.91~1.82) 1.13(0.81~1.62) Z=4.51 <0.001 TC(mmol/L) 4.88±1.10 4.97±1.09 4.88±1.10 t=-1.86 0.178 HDL-C(mmol/L) 1.56±0.40 1.54±0.41 1.56±0.40 t=0.67 0.798 LDL-C(mmol/L) 2.33±0.91 2.37±1.10 2.33±0.91 t=-1.01 0.997 hs-CRP(mg/L) 0.70(0.27~2.00) 1.28(0.48~3.49) 0.70(0.26~2.00) Z=8.31 <0.001 男性[例(%)] 54 930(78.90) 443(92.10) 54 487(78.81) <0.001 高中及以上教育程度[例(%)] 14 107(20.26) 73(15.18) 14 034(20.30) 0.021 月人均收入≥800元[例(%)] 49 204(70.67) 351(72.97) 48 853(70.66) 0.539 体育锻炼[例(%)] 63 473(91.17) 457(95.01) 63 016(91.14) 0.012 吸烟史[例(%)] 23 756(34.12) 149(30.98) 23 607(34.14) 0.345 饮酒史[例(%)] 25 310(36.35) 132(27.44) 25 178(36.42) <0.001 糖尿病史[例(%)] 4 718(6.78) 99(20.58) 4 619(6.68) <0.001 高血压史[例(%)] 26 457(38.00) 325(67.57) 26 132(37.80) <0.001 血脂异常[例(%)] 36 978(53.11) 273(56.76) 36 705(53.09) 0.275 服降糖药[例(%)] 1 028(1.48) 8(1.66) 1 020(1.48) 0.944 服降压药[例(%)] 4 733(6.80) 133(27.65) 4 600(6.65) <0.001 服降脂药[例(%)] 4 119(5.92) 126(26.20) 3 993(5.78) <0.001 注:BMI,体重指数;SBP,收缩压;DBP,舒张压;ALT,丙氨酸氨基转移酶;UA,尿酸;eGFR,估算肾小球滤过率;FBG,空腹血糖;TG,甘油三酯;TC,总胆固醇;HDL-C,高密度脂蛋白胆固醇;LDL-C,低密度脂蛋白胆固醇;hs-CRP,超敏C反应蛋白;ASCVD,动脉粥样硬化性心血管疾病。
下载: 导出CSV
表 3 MAFLD组与非MAFLD组ASCVD累积发病率与发病密度
Table 3. The cumulative incidence and incidence density of new ASCVD in the MAFLD group and the non-MAFLD group
项目 新发ASCVD[例(%)] 发病密度(/千人年) 累积发病率(%) 非MAFLD组 6 529(9.66) 8.24 10.02 年龄 18~<45岁 767(11.75) 2.65 3.26 45~<60岁 3 415(52.31) 8.94 10.82 ≥60岁 2 347(35.95) 19.25 22.13 MAFLD组 4 263(14.70) 12.90 15.43 年龄 18~<45岁 577(13.54) 5.88 6.99 45~<60岁 2 400(56.30) 13.25 15.97 ≥60岁 1 286(30.17) 25.08 28.01 注:MAFLD,代谢相关脂肪性肝病;ASCVD,动脉粥样硬化性心血管疾病。
下载: 导出CSV
表 4 ASCVD组与非ASCVD组ASCVD累积发病率与发病密度
Table 4. Cumulative incidence and incidence density of new ASCVD in the ASCVD group and the non-ASCVD group
项目 新发MAFLD[例(%)] 发病密度(/千人年) 累积发病率(%) 非ASCVD组 32 194(46.56) 57.59 47.57 年龄 18~<45岁 11 517(35.77) 70.73 56.01 45~<60岁 15 580(48.39) 60.65 50.35 ≥60岁 5 097(15.83) 36.58 33.15 ASCVD组 148(30.77) 40.10 35.01 年龄 18~<45岁 10(6.76) 85.24 54.39 45~<60岁 72(48.65) 52.23 45.16 ≥60岁 66(44.59) 30.07 26.56 注:MAFLD,代谢相关脂肪性肝病;ASCVD,动脉粥样硬化性心血管疾病。
下载: 导出CSV
表 5 多因素Cox比例风险回归模型分析MAFLD对新发ASCVD风险的影响
Table 5. Multivariate Cox proportional risk regression model analysis of the effect of MAFLD on the risk of new-onset ASCVD
项目 模型1 模型2 模型3 HR(95%CI) P值 HR(95%CI) P值 HR(95%CI) P值 非MAFLD组 1.00 1.00 1.00 年龄 18~<45岁 1.00 1.00 1.00 45~<60岁 3.15(2.92~3.41) <0.001 2.48(2.29~2.69) <0.001 2.32(2.14~2.52) <0.001 ≥60岁 6.21(5.72~6.74) <0.001 4.62(4.25~5.03) <0.001 4.13(3.78~4.52) <0.001 MAFLD组1) 1.53(1.47~1.59) <0.001 1.24(1.19~1.29) <0.001 1.11(1.06~1.16) <0.001 年龄 18~<45岁 1.00 1.00 1.00 45~<60岁 2.39(2.18~2.62) <0.001 2.08(1.90~2.28) <0.001 1.97(1.79~2.17) <0.001 ≥60岁 4.37(3.96~4.82) <0.001 3.66(3.31~4.05) <0.001 3.30(2.96~3.68) <0.001 注:1),以非MAFLD组为参照。HR,风险比;95%CI,95%置信区间;MAFLD,代谢相关脂肪性肝病;ASCVD,动脉粥样硬化性心血管疾病。
下载: 导出CSV
表 6 多因素Cox比例风险回归模型分析ASCVD对新发MAFLD风险的影响
Table 6. Multivariate Cox proportional risk regression model analysis of the effect of ASCVD on the risk of new-onset MAFLD
项目 模型1 模型2 模型3 HR(95%CI) P值 HR(95%CI) P值 HR(95%CI) P值 非ASCVD组 1.00 1.00 1.00 年龄 18~<45岁 1.00 1.00 1.00 45~<60岁 0.80(0.78~0.82) <0.001 0.74(0.72~0.76) <0.001 0.70(0.69~0.72) <0.001 ≥60岁 0.45(0.43~0.46) <0.001 0.40(0.39~0.42) <0.001 0.39(0.37~0.40) <0.001 ASCVD组1) 0.80(0.68~0.94) 0.006 0.77(0.66~0.91) 0.002 0.72(0.61~0.85) <0.001 年龄 18~<45岁 1.00 1.00 1.00 45~<60岁 0.58(0.30~1.11) 0.101 0.59(0.30~1.18) 0.141 0.40(0.20~0.83) 0.014 ≥60岁 0.30(0.16~0.59) <0.001 0.29(0.14~0.57) <0.001 0.23(0.11~0.48) <0.001 注:1),以非ASCVD组为参照。HR,风险比;95%CI,95%置信区间;MAFLD,代谢相关脂肪性肝病;ASCVD,动脉粥样硬化性心血管疾病。
下载: 导出CSV
表 7 MAFLD与ASCVD相互影响的敏感性分析
Table 7. Sensitivity analyses for bidirectional MAFLD and ASCVD study
项目 HR(95%CI) P值 ASCVD 排除2年内新发ASCVD事件的患者 非MAFLD组 1.00 MAFLD组 1.12(1.07~1.17) <0.001 死亡竞争风险模型 非MAFLD组 1.00 MAFLD组 1.11(1.06~1.16) <0.001 MAFLD 排除2年内新发MAFLD事件的患者 非ASCVD组 1.00 ASCVD组 0.69(0.56~0.84) <0.001 死亡竞争风险模型 非ASCVD组 1.00 ASCVD组 0.59(0.50~0.69) <0.001 注:HR,风险比;95%CI,95%置信区间;MAFLD,代谢相关脂肪性肝病;ASCVD,动脉粥样硬化性心血管疾病。
下载: 导出CSV
-
[1] LIM GEH, TANG A, NG CH, et al. An observational data meta-analysis on the differences in prevalence and risk factors between MAFLD vs NAFLD[J]. Clin Gastroenterol Hepatol, 2023, 21( 3): 619- 629. DOI: 10.1016/j.cgh.2021.11.038. [2] WONG MCS, HUANG JLW, GEORGE J, et al. The changing epidemiology of liver diseases in the Asia-Pacific region[J]. Nat Rev Gastroenterol Hepatol, 2019, 16( 1): 57- 73. DOI: 10.1038/s41575-018-0055-0. [3] HAN QL, MAO RY, YU J, et al. Risk factors analysis for prevalence of acute myocardial infarction in young and middle-aged population[J]. Chin Circ J, 2016, 31( 7): 632- 635. DOI: 10.3969/j.issn.1000-3614.2016.07.003.韩全乐, 毛瑞英, 郁静, 等. 中青年人群发生急性心肌梗死的危险因素分析[J]. 中国循环杂志, 2016, 31( 7): 632- 635. DOI: 10.3969/j.issn.1000-3614.2016.07.003. [4] YUE BC, YU J, HAN QL, et al. Risk and risk factors of acute myocardial infarction within 10 years in a young and middle-aged population of a vegion[J]. Chongqing Med, 2020, 49( 11): 1850- 1854. DOI: 10.3969/j.issn.1671-8348.2020.11.029.岳博成, 于洁, 韩全乐, 等. 某地区中青年人群10年内急性心肌梗死的风险及危险因素分析[J]. 重庆医学, 2020, 49( 11): 1850- 1854. DOI: 10.3969/j.issn.1671-8348.2020.11.029. [5] National Center for Cardiovascular Diseases, The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on cardiovascular health and diseases in China 2023: An updated summary[J]. Chin Circ J, 2024, 39( 7): 625- 660. DOI: 10.3969/j.issn.1000-3614.2024.07.001.国家心血管病中心, 中国心血管健康与疾病报告编写组. 中国心血管健康与疾病报告2023概要[J]. 中国循环杂志, 2024, 39( 7): 625- 660. DOI: 10.3969/j.issn.1000-3614.2024.07.001. [6] LEE H, LEE YH, KIM SU, et al. Metabolic dysfunction-associated fatty liver disease and incident cardiovascular disease risk: A nationwide cohort study[J]. Clin Gastroenterol Hepatol, 2021, 19( 10): 2138- 2147. DOI: 10.1016/j.cgh.2020.12.022. [7] TSUTSUMI T, ESLAM M, KAWAGUCHI T, et al. MAFLD better predicts the progression of atherosclerotic cardiovascular risk than NAFLD: Generalized estimating equation approach[J]. Hepatol Res, 2021, 51( 11): 1115- 1128. DOI: 10.1111/hepr.13685. [8] TOH JZK, PAN XH, TAY PWL, et al. A meta-analysis on the global prevalence, risk factors and screening of coronary heart disease in nonalcoholic fatty liver disease[J]. Clin Gastroenterol Hepatol, 2022, 20( 11): 2462- 2473. DOI: 10.1016/j.cgh.2021.09.021. [9] ZHOU XD, TIAN N, ZHENG MH. Excerpt of an international multidisciplinary consensus statement on MAFLD and the risk of CVD(2023)[J]. J Clin Hepatol, 2023, 39( 10): 2336- 2339. DOI: 10.3969/j.issn.1001-5256.2023.10.010.周晓东, 田娜, 郑明华.《2023年国际多学科专家共识: 代谢相关脂肪性肝病和心血管疾病风险》摘译[J]. 临床肝胆病杂志, 2023, 39( 10): 2336- 2339. DOI: 10.3969/j.issn.1001-5256.2023.10.010. [10] LIN S, HUANG JF, WANG MF, et al. Comparison of MAFLD and NAFLD diagnostic criteria in real world[J]. Liver Int, 2020, 40( 9): 2082- 2089. DOI: 10.1111/liv.14548. [11] DEWIDAR B, KAHL S, PAFILI K, et al. Metabolic liver disease in diabetes- From mechanisms to clinical trials[J]. Metabolism, 2020, 111: 154299. DOI: 10.1016/j.metabol.2020.154299. [12] SUN DQ, JIN Y, WANG TY, et al. MAFLD and risk of CKD[J]. Metabolism, 2021, 115: 154433. DOI: 10.1016/j.metabol.2020.154433. [13] KIM D, KONYN P, SANDHU KK, et al. Metabolic dysfunction-associated fatty liver disease is associated with increased all-cause mortality in the United States[J]. J Hepatol, 2021, 75( 6): 1284- 1291. DOI: 10.1016/j.jhep.2021.07.035. [14] MOON JH, KIM W, KOO BK, et al. Metabolic dysfunction-associated fatty liver disease predicts long-term mortality and cardiovascular disease[J]. Gut Liver, 2022, 16( 3): 433- 442. DOI: 10.5009/gnl210167. [15] HOU QQ, QI Q, HAN QL, et al. Association of the triglyceride-glucose index with early-onset atherosclerotic cardiovascular disease events and all-cause mortality: A prospective cohort study[J]. Cardiovasc Diabetol, 2024, 23( 1): 149. DOI: 10.1186/s12933-024-02249-4. [16] THYGESEN K, ALPERT JS, JAFFE AS, et al. Third universal definition of myocardial infarction[J]. Eur Heart J, 2012, 33( 20): 2551- 2567. DOI: 10.1093/eurheartj/ehs184. [17] LUO J, THOMASSEN JQ, NORDESTGAARD BG, et al. Neutrophil counts and cardiovascular disease[J]. Eur Heart J, 2023, 44( 47): 4953- 4964. DOI: 10.1093/eurheartj/ehad649. [18] Chinese Society of Neurology, Chinese Stroke Society. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018[J]. Chin J Neurol, 2018, 51( 9): 666- 682. DOI: 10.3760/cma.j.issn.1006-7876.2018.09.004.中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51( 9): 666- 682. DOI: 10.3760/cma.j.issn.1006-7876.2018.09.004. [19] Chinese Nutrition Society Obesity Prevention and Control Section, Chinese Nutrition Society Clinical Nutrition Section, Chinese Preventive Medicine Association Behavioral Health Section, et al. Expert consensus on obesity prevention and treatment in China[J]. China Prev Med, 2022, 23( 5): 321- 339. DOI: 10.16506/j.1009-6639.2022.05.001.中国营养学会肥胖防控分会, 中国营养学会临床营养分会, 中华预防医学会行为健康分会, 等. 中国居民肥胖防治专家共识[J]. 中国预防医学杂志, 2022, 23( 5): 321- 339. DOI: 10.16506/j.1009-6639.2022.05.001. [20] Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China(2020 edition)[J]. Chin J Diabetes Mellitus, 2021, 13( 4): 315- 409. DOI: 10.3760/cma.j.cn115791-20210221-00095.中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2020年版)[J]. 中华糖尿病杂志, 2021, 13( 4): 315- 409. DOI: 10.3760/cma.j.cn115791-20210221-00095. [21] Hypertension Branch of the Chinese Society of Geriatrics, Beijing Hypertension Prevention and Control Association, National Clinical Research Center for Geriatric Diseases. Chinese guidelines for hypertension management in the elderly 2023[J]. Chin J Hypertens, 2023, 31( 6): 508- 538. DOI: 10.16439/j.issn.1673-7245.2023.06.003.中国老年医学学会高血压分会, 北京高血压防治协会, 国家老年疾病临床医学研究中心. 中国老年高血压管理指南2023[J]. 中华高血压杂志, 2023, 31( 6): 508- 538. DOI: 10.16439/j.issn.1673-7245.2023.06.003. [22] DENG J, QI Q, WU XY, et al. Cohort study on the association between the atherogenic index of plasma and the risk of incident heart failure in a physical examination population[J]. Chin Gen Pract, 2025, 28( 29): 3645- 3652. DOI: 10.12114/j.issn.1007-9572.2025.0087.邓洁, 齐祺, 吴欣雨, 等. 血浆致动脉硬化指数与体检人群新发心力衰竭风险的队列研究[J]. 中国全科医学, 2025, 28( 29): 3645- 3652. DOI: 10.12114/j.issn.1007-9572.2025.0087. [23] WANG XY, ZHANG RS, MAN S, et al. Metabolic-associated fatty liver disease in relation to site-specific and multiple-site subclinical atherosclerosis[J]. Liver Int, 2023, 43( 8): 1691- 1698. DOI: 10.1111/liv.15591. [24] CHEN Y, LU C, JU HN, et al. Elevated AIP is associated with the prevalence of MAFLD in the US adults: Evidence from NHANES 2017-2018[J]. Front Endocrinol(Lausanne), 2024, 15: 1405828. DOI: 10.3389/fendo.2024.1405828. [25] LIU SH, LIU Q, HAN X, et al. Association of trajectories of atherogenic index of plasma with atherosclerotic cardiovascular disease[J]. Chin Circ J, 2024, 39( 7): 676- 681. DOI: 10.3969/j.issn.1000-3614.2024.07.004.刘士贺, 刘倩, 韩旭, 等. 血浆致动脉粥样硬化指数轨迹与动脉粥样硬化性心血管疾病的关联[J]. 中国循环杂志, 2024, 39( 7): 676- 681. DOI: 10.3969/j.issn.1000-3614.2024.07.004. [26] LYU SJ, WU SL, LI JF, et al. Impact of the atherogenic index of plasma on new-onset ischemic stroke[J]. Chin J Cardiov Med, 2024, 29( 3): 198- 204. DOI: 10.3969/j.issn.1007-5410.2024.03.002.吕素洁, 吴寿岭, 李金锋, 等. 血浆致动脉粥样硬化指数对新发缺血性脑卒中的影响[J]. 中国心血管杂志, 2024, 29( 3): 198- 204. DOI: 10.3969/j.issn.1007-5410.2024.03.002. [27] DUAN SJ, REN ZY, ZHENG T, et al. Atherogenic index of plasma combined with waist circumference and body mass index to predict metabolic-associated fatty liver disease[J]. World J Gastroenterol, 2022, 28( 36): 5364- 5379. DOI: 10.3748/wjg.v28.i36.5364. [28] FERNÁNDEZ-MACÍAS JC, OCHOA-MARTÍNEZ AC, VARELA-SILVA JA, et al. Atherogenic index of plasma: Novel predictive biomarker for cardiovascular illnesses[J]. Arch Med Res, 2019, 50( 5): 285- 294. DOI: 10.1016/j.arcmed.2019.08.009. [29] WON KB, HEO R, PARK HB, et al. Atherogenic index of plasma and the risk of rapid progression of coronary atherosclerosis beyond traditional risk factors[J]. Atherosclerosis, 2021, 324: 46- 51. DOI: 10.1016/j.atherosclerosis.2021.03.009. [30] ZHU XW, YU LG, ZHOU H, et al. Atherogenic index of plasma is a novel and better biomarker associated with obesity: A population-based cross-sectional study in China[J]. Lipids Health Dis, 2018, 17( 1): 37. DOI: 10.1186/s12944-018-0686-8. [31] LI YW, KAO TW, CHANG PK, et al. Atherogenic index of plasma as predictors for metabolic syndrome, hypertension and diabetes mellitus in Taiwan citizens: A 9-year longitudinal study[J]. Sci Rep, 2021, 11( 1): 9900. DOI: 10.1038/s41598-021-89307-z. [32] DONGIOVANNI P, PAOLINI E, CORSINI A, et al. Nonalcoholic fatty liver disease or metabolic dysfunction-associated fatty liver disease diagnoses and cardiovascular diseases: From epidemiology to drug approaches[J]. Eur J Clin Invest, 2021, 51( 7): e13519. DOI: 10.1111/eci.13519. [33] DEPRINCE A, HAAS JT, STAELS B. Dysregulated lipid metabolism links NAFLD to cardiovascular disease[J]. Mol Metab, 2020, 42: 101092. DOI: 10.1016/j.molmet.2020.101092. [34] YONEDA M, YAMAMOTO T, HONDA Y, et al. Risk of cardiovascular disease in patients with fatty liver disease as defined from the metabolic dysfunction associated fatty liver disease or nonalcoholic fatty liver disease point of view: A retrospective nationwide claims database study in Japan[J]. J Gastroenterol, 2021, 56( 11): 1022- 1032. DOI: 10.1007/s00535-021-01828-6. [35] ZHANG C, ZHU PH, HE LL. Research progress on the correlation between metabolic associated fatty liver disease and cardiovascular disease risk[J/CD]. Chin J Liver Dis(Electronic Version), 2025, 17( 1): 12- 18. DOI: 10.3969/j.issn.1674-7380.2025.01.003.张成, 朱平辉, 何玲玲. 代谢相关脂肪性肝病与心血管疾病风险相关性研究现状[J/CD]. 中国肝脏病杂志(电子版), 2025, 17( 1): 12- 18. DOI: 10.3969/j.issn.1674-7380.2025.01.003. [36] Chinese Society of Cardiology, Chinese Medical Association; Cardiovascular Disease Prevention and Rehabilitation Committee of Chinese Association of Rehabilitation Medicine; Cardiovascular Disease Committee of Chinese Association of Gerontology and Geriatrics, et al. Chinese guideline on the primary prevention of cardiovascular diseases in primary health care[J]. Chin J Cardiol, 2023, 51( 4): 343- 363. DOI: 10.3760/cma.j.cn112148-20230106-00014.中华医学会心血管病学分会, 中国康复医学会心脏预防与康复专业委员会, 中国老年学和老年医学会心脏专业委员会, 等. 中国心血管病一级预防指南基层版[J]. 中华心血管病杂志, 2023, 51( 4): 343- 363. DOI: 10.3760/cma.j.cn112148-20230106-00014. [37] WANG LL, YI JY, GUO XL, et al. Associations between life's essential 8 and non-alcoholic fatty liver disease among US adults[J]. J Transl Med, 2022, 20( 1): 616. DOI: 10.1186/s12967-022-03839-0. [38] BIKOV A, MESZAROS M, KUNOS L, et al. Atherogenic index of plasma in obstructive sleep apnoea[J]. J Clin Med, 2021, 10( 3): 417. DOI: 10.3390/jcm10030417. [39] CHEN Y, XU LH, MAO YY, et al. Associations of lifestyle scores with nonalcoholic fatty liver disease[J]. Modern Preventive Medicine, 2024, 51( 4): 742- 747. DOI: 10.20043/j.cnki.MPM.202310283.陈颖, 徐柳红, 毛盈颖, 等. 生活方式评分与非酒精性脂肪肝的关联性研究[J]. 现代预防医学, 2024, 51( 4): 742- 747. DOI: 10.20043/j.cnki.MPM.202310283. [40] WEI YX, ZHOU XD, ZHENG MH. Heart and liver co-management:integrated management of metabolic dysfunction-associated steatotic liver disease with cardiovascular disease[J/CD]. Chin J Liver Dis(Electronic Version), 2025, 17( 3): 1- 9. DOI: 10.3969/j.issn.1674-7380.2025.03.001.韦艺轩, 周晓东, 郑明华. 心肝共治: 代谢相关脂肪性肝病合并心血管疾病风险的协同管理[J/CD]. 中国肝脏病杂志(电子版), 2025, 17( 3): 1- 9. DOI: 10.3969/j.issn.1674-7380.2025.03.001. -

 本文二维码
本文二维码
计量
- 文章访问数: 241
- HTML全文浏览量: 73
- PDF下载量: 79
- 被引次数: 0

