
 PDF下载 ( 1401 KB)
PDF下载 ( 1401 KB)

高血糖对慢性乙型肝炎合并脂肪性肝病患者肝纤维化及终末期肝病的影响
DOI: 10.12449/JCH260411
Impact of hyperglycemia on liver fibrosis and end-stage liver disease in patients with comorbidities of chronic hepatitis B and steatotic liver disease
-
摘要:
目的 分析慢性乙型肝炎(CHB)合并脂肪性肝病(SLD)患者的临床病理特征,探讨血糖升高对肝纤维化及终末期肝病发生风险的影响,为此类人群的临床管理提供依据。 方法 纳入2011年1月—2019年12月中国人民解放军总医院第五医学中心经肝活检确诊的成人CHB-SLD患者668例,以肝穿刺时间为起点、终末期肝病发生为终点,随访至2024年3月31日。采用1∶4倾向性评分匹配(PSM)平衡组间基线差异,最终纳入高血糖组患者82例,无高血糖组患者281例。比较两组患者的代谢特征、实验室指标及肝组织病理特征。非正态分布的计量资料2组间比较采用Mann-Whitney U检验;计数资料2组间比较采用χ2检验或Fisher精确检验。通过多因素Logistic回归分析进展期肝纤维化的影响因素,运用Kaplan-Meier生存分析及Cox比例风险回归模型评估终末期肝病发生的影响因素。 结果 与无高血糖组相比,高血糖组患者代谢紊乱因素更多,肝脂肪变性程度更重,进展期肝纤维化的检出率更高(P值均<0.05)。多因素Logistic回归分析显示,高血糖是进展期肝纤维化的危险因素(比值比=1.753,95%置信区间:1.017~3.023,P=0.043)。生存分析显示,高血糖增加了终末期肝病的发生风险(χ2=4.340,P=0.037)。多因素Cox回归证实,高血糖是进展期肝纤维化人群发生终末期肝病的代谢危险因素(校正风险比=3.208,95%置信区间:1.201~8.568,P=0.020)。 结论 高血糖可增加CHB-SLD患者进展期肝纤维化及终末期肝病的发生风险。对已合并进展期肝纤维化且高血糖水平的患者,应加强临床监测和管理。 Abstract:Objective To analyze the clinicopathological features of patients with comorbidities of chronic hepatitis B (CHB) and steatotic liver disease (SLD), to investigate the impact of hyperglycemia on the risk of liver fibrosis and end-stage liver diseases (ESLD), and to provide a basis for the clinical management of such population. Methods A total of 668 adult patients with CHB-SLD confirmed by liver biopsy in The Fifth Medical Center of Chinese PLA General Hospital from January 2011 to December 2019 were enrolled, and a retrospective cohort was established with the time of liver biopsy as the baseline and the onset of ESLD as the endpoint. All patients were followed up to March 31, 2024. Propensity score matching (PSM) was performed at a ratio of 1∶4 to balance baseline features between groups, resulting in 82 patients in the hyperglycemia group and 281 in the non-hyperglycemia group. The two groups were compared in terms of metabolic profiles, laboratory markers, and histopathological features. The Mann-Whitney U test was used for comparison of non-normally distributed quantitative data between two groups. The chi-square test or Fisher exact test was used for comparison of categorical data between two groups. A multivariate Logistic regression analysis was used to investigate the influencing factors for advanced fibrosis (AF), and the Kaplan-Meier survival analysis and the Cox proportional-hazards regression model were used to determine the influencing factors for the development of ESLD. Results Compared with the non-hyperglycemia group, the hyperglycemia group had a significantly higher number of factors for metabolic disorders, a significantly higher degree of hepatic steatosis, and a significantly higher detection rate of AF (all P<0.05). The multivariate Logistic regression analysis showed that hyperglycemia was a risk factor for AF (odds ratio = 1.753, 95% confidence interval [CI]: 1.017 — 3.023, P=0.043). The survival analysis showed that hyperglycemia increased the risk of ESLD (χ2=4.340, P=0.037). The multivariate Cox regression analysis confirmed that hyperglycemia was a significant metabolic risk factor for ESLD in patients with AF (adjusted hazard ratio=3.208, 95%CI: 1.201 — 8.568, P=0.020). Conclusion Hyperglycemia can increase the risk of AF and ESLD in CHB-SLD patients. Clinical monitoring and active management should be strengthened for patients who have already developed AF and hyperglycemia. -
Key words:
- Hepatitis B, Chronic /
- Fatty Liver /
- Diabetes Mellitus /
- Hyperglycemia /
- End Stage Liver Disease /
- Root Cause Analysis
-
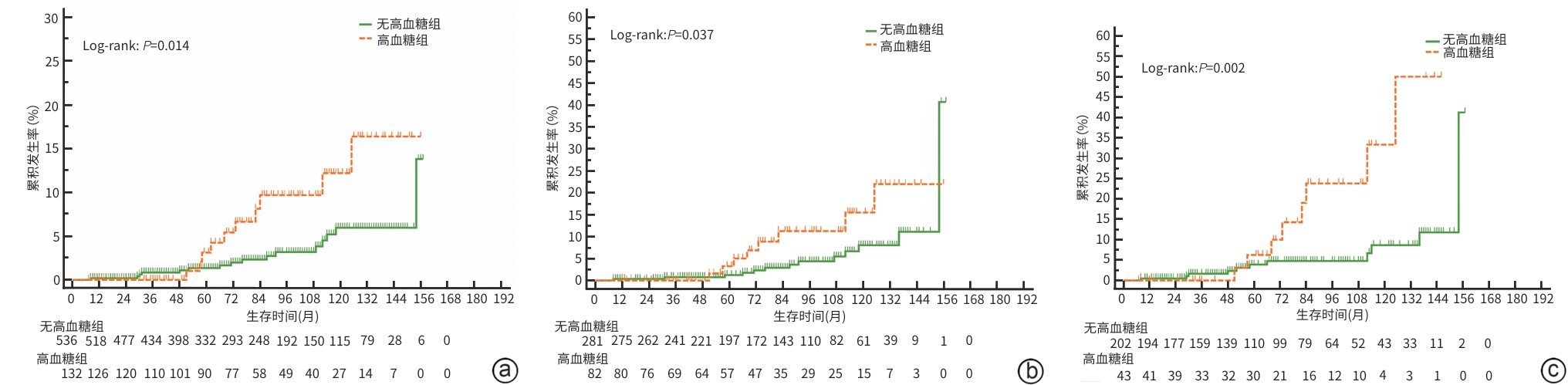
注: a,PSM前高血糖组与无高血糖组患者生存分析;b,PSM后高血糖组与无高血糖组患者生存分析;c,PSM前高血糖组与无高血糖组进展期肝纤维化人群生存分析。
图 1 生存分析
Figure 1. Survival analysis
表 1 CHB-SLD患者的基线特征
Table 1. Baseline characteristics of CHB-SLD patients
项目 PSM前 PSM后 高血糖组(n=83) 无高血糖组(n=585) P值 高血糖组(n=82) 无高血糖组(n=281) P值 年龄(岁) 44.0(39.0~48.5) 37.0(30.0~44.0) <0.001 44.0(39.0~47.0) 43.0(38.0~47.0) 0.315 男[例(%)] 69(83.1) 479(81.9) 0.900 68(82.9) 224(79.7) 0.519 饮酒史[例(%)] 0.115 0.502 无 41(49.4) 383(65.5) 41(50.0) 165(58.7) 偶尔1) 19(22.9) 121(20.7) 19(23.2) 60(21.4) 有2) 23(27.7) 81(13.8) 22(26.8) 56(19.9) BMI(kg/m2) 27.3(25.5~29.4) 26.2(24.2~28.4) 0.007 27.4(25.6~29.4) 26.2(24.5~28.2) 0.006 超重/肥胖[例(%)]3) 74(89.2) 448(76.6) 0.014 74(90.2) 220(78.3) 0.015 空腹血糖(mmol/L) 6.60(6.18~7.65) 4.80(4.50~5.20) <0.001 6.60(6.20~7.68) 4.80(4.50~5.20) <0.001 高血压[例(%)]4) 22(26.5) 61(10.4) <0.001 21(25.6) 24(8.5) <0.001 高甘油三酯血症[例(%)]5) 44(53.0) 184(31.5) <0.001 43(52.4) 100(35.6) 0.006 总胆固醇(mmol/L) 4.35(3.82~5.02) 4.25(3.75~4.95) 0.237 4.36(3.82~5.02) 4.32(3.83~4.98) 0.465 高密度脂蛋白降低[例(%)]6) 59(71.1) 371(63.4) 0.172 58(70.7) 175(62.3) 0.160 低密度脂蛋白(mmol/L) 3.05(2.65~3.55) 3.00(2.55~3.44) 0.243 3.06(2.72~3.55) 3.00(2.62~3.43) 0.326 代谢危险因素数量[例(%)] <0.001 <0.001 0~1个 0(0.0) 214(36.6) 0(0.0) 102(36.3) 2~3个 49(59.0) 364(62.2) 49(59.8) 174(61.9) 4~5个 34(41.0) 7(1.2) 33(40.2) 5(1.8) 生化指标 Hb(g/L) 153(144~163) 153(143~161) 0.720 154(145~163) 151(142~160) 0.135 PLT(×109/L) 187(141~218) 194(160~233) 0.038 188(142~218) 183(149~220) 0.742 Alb(g/L) 42.0(39.0~43.0) 42.0(40.0~44.0) 0.081 42.0 (39.0~43.3) 41.0(38.0~44.0) 0.960 ALT(U/L) 48.0(34.5~90.0) 46.0(29.0~71.0) 0.151 48.0(34.2~90.2) 41.0(27.0~67.0) 0.027 AST(U/L) 33.0(25.0~54.5) 31.0(23.0~48.0) 0.248 33.0(25.0~52.2) 31.0(23.0~47.0) 0.253 病毒相关指标[例(%)] HBV DNA≤2 000 IU/mL 31(37.3) 175(29.9) 0.213 52(63.4) 194(69.0) 0.338 HBsAg≥1 000 COI 68(81.9) 436(74.5) 0.184 67(81.7) 214(76.2) 0.290 HBeAg阳性 38(45.8) 350(58.8) 0.021 38(46.3) 148(52.7) 0.313 注:1)不规律或偶有饮酒,饮酒量未达酒精性肝病诊断要求;2)饮酒量男性≥40 g/d或女性≥20 g/d,按照《酒精性肝病防治指南(2018年更新版)》换算乙醇量,换算公式=饮酒量(mL)×乙醇含量(%)×0.8;3)体重指数≥24 kg/m2;4)血压≥130/85 mmHg,或正在接受抗高血压药物治疗;5)空腹血清甘油三酯≥1.70 mmol/L,或正在接受降脂药物治疗;6)血清高密度脂蛋白≤1.0 mmol/L(男)和≤1.3 mmol/L(女),或正在接受降脂药物治疗。PSM,倾向评分匹配;BMI,体重指数;Hb,血红蛋白;PLT,血小板;Alb,白蛋白;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;HBV,乙型肝炎病毒;HBsAg,乙型肝炎病毒表面抗原;HBeAg,乙型肝炎病毒e抗原;CHB-SLD,慢性乙型肝炎合并脂肪性肝病。
 下载: 导出CSV
下载: 导出CSV
表 2 CHB-SLD患者的肝组织学特征
Table 2. Histological characteristics of CHB-SLD patients
项目 PSM前 PSM后 高血糖组(n=83) 无高血糖组(n=585) P值 高血糖组(n=82) 无高血糖组(n=281) P值 脂肪变性程度[例(%)] 0.013 0.003 轻度 50(60.2) 433(74.0) 49(59.8) 215(76.5) 中重度 33(39.8) 152(26.0) 33(40.2) 66(23.5) 气球样变[例(%)] 0.012 0.112 无 65(78.3) 519(88.7) 64(78.0) 240(85.4) 有 18(21.7) 66(11.3) 18(22.0) 41(14.6) 小叶内炎症[例(%)] 0.761 0.999 <2个/20倍镜 68(81.9) 491(83.9) 68(82.9) 233(82.9) ≥2个/20倍镜 15(18.1) 94(16.1) 14(17.1) 48(17.1) 汇管区炎症[例(%)] 0.346 0.392 无/轻度 35(42.2) 283(48.4) 35(42.7) 135(48.0) 中重度 48(57.8) 302(51.6) 47(57.3) 146(52.0) 界面炎[例(%)] 0.051 0.124 无 40(48.2) 352(60.2) 40(48.8) 164(58.4) 有 43(51.8) 233(39.8) 42(51.2) 117(41.6) 融合坏死[例(%)] >0.05 0.182 无或偶见 82(98.8) 573(97.9) 82(100.0) 275(97.9) 可见 1(1.2) 12(2.1) 0(0.0) 6(2.1) 炎症活动度[例(%)] >0.05 0.657 G0~1 57(68.7) 405(69.2) 57(69.5) 188(66.9) G2~4 26(31.3) 180(30.8) 25(30.5) 93(33.1) 肝纤维化分期[例(%)] 0.002 0.009 F0~2 40(48.2) 383(65.5) 40(48.8) 182(64.8) F3~4 43(51.8) 202(34.5) 42(51.2) 99(35.2) 窦周纤维化[例(%)] 0.003 0.017 无 71(85.5) 554(94.7) 70(85.4) 263(93.6) 有 12(14.5) 31(5.3) 12(14.6) 18(6.4) NAS[例(%)] 0.006 0.012 0~2分 38(45.8) 374(63.9) 38(46.3) 180(64.1) 3~4分 38(45.8) 176(30.1) 37(45.1) 80(28.5) 5~8分 7(8.4) 35(6.0) 7(8.5) 21(7.4) 注:PSM,倾向评分匹配;NAS,非酒精性脂肪性肝病活动度评分系统;CHB-SLD,慢性乙型肝炎合并脂肪性肝病。
下载: 导出CSV
表 3 Logistic回归分析进展期肝纤维化的影响因素
Table 3. Logistic regression analysis of metabolic, viral, and histological factors associated with advanced fibrosis
变量 B值 标准误 Wald χ2值 OR 95%CI P值 性别1) 0.097 0.275 0.126 1.102 0.643~1.889 0.723 年龄(岁) 0.025 0.011 4.936 1.025 1.003~1.048 0.026 高血糖 0.561 0.278 4.079 1.753 1.017~3.023 0.043 高甘油三酯血症 -0.395 0.207 3.650 0.674 0.449~1.010 0.056 BMI(kg/m2) 0.266 0.238 1.249 1.305 0.818~2.082 0.264 脂肪变性2) -0.023 0.213 0.012 0.977 0.644~1.482 0.913 炎症活动度3) 1.665 0.219 57.807 5.288 3.442~8.123 <0.001 HBeAg4) 0.053 0.219 0.060 1.055 0.687~1.620 0.807 HBV DNA5) -0.353 0.231 2.326 0.703 0.447~1.106 0.807 HBsAg6) 0.445 0.238 3.501 1.560 0.979~2.486 0.061 PLT(×109/L) -0.009 0.002 25.360 0.991 0.987~0.994 <0.001 Alb(g/L) -0.042 0.027 2.429 0.959 0.909~1.011 0.119 ALT(U/L) -0.004 0.002 3.792 0.996 0.992~1.000 0.051 AST(U/L) 0.005 0.004 1.779 1.005 0.997~1.014 0.182 注:BMI,体重指数;HBV,乙型肝炎病毒;HBeAg,乙型肝炎病毒e抗原;HBsAg,乙型肝炎病毒表面抗原;PLT,血小板;Alb,白蛋白;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;OR,比值比;95%CI,95%置信区间。计数资料赋值情况如下:1)性别:女=0,男=1;2)脂肪变性:轻度=0,中重度=1;3)炎症活动度:G0~1=0,G2~4=1;4)HBeAg:阴性=0,阳性=1;5)HBV DNA定量:≤2 000 IU/mL=0,>2 000 IU/mL=1;6)HBsAg:<1 000 COI=0,≥1 000 COI=1。
下载: 导出CSV
表 4 CHB-SLD患者发生终末期肝病的Cox回归分析
Table 4. Cox proportional-hazards regression for ESLD among the entire cohort
变量 PSM前单因素分析 PSM前多因素分析 PSM后单因素分析 PSM后多因素分析 HR(95%CI) P值 aHR(95%CI) P值 HR(95%CI) P值 aHR(95%CI) P值 基本特征 年龄(岁) 1.06(1.02~1.10) 0.006 1.02(0.97~1.06) 0.515 1.03(0.97~1.09) 0.388 性别1) 0.62(0.25~1.56) 0.313 0.71(0.26~1.96) 0.509 代谢特征 超重/肥胖2) 0.84(0.29~2.45) 0.754 0.71(0.26~1.95) 0.503 高血糖3) 2.59(1.17~5.73) 0.019 2.21(0.97~5.06) 0.061 2.31(0.96~5.59) 0.062 高血压4) 1.85(0.64~5.37) 0.260 0.94(0.27~3.31) 0.927 高甘油三酯血症5) 0.69(0.29~1.64) 0.397 0.62(0.24~1.59) 0.317 高密度脂蛋白 降低6) 1.09(0.49~2.45) 0.830 1.10(0.45~2.74) 0.832 生化指标 Hb(g/L) 0.98(0.96~1.01) 0.137 0.99(0.96~1.01) 0.319 PLT(×109/L) 0.98(0.98~0.99) <0.001 0.99(0.98~0.99) 0.003 0.99(0.98~0.99) 0.001 0.99(0.98~0.99) 0.014 Alb(g/L) 0.83(0.76~0.91) <0.001 0.88(0.80~0.97) 0.011 0.85(0.76~0.94) 0.002 0.88(0.79~0.99) 0.029 ALT(U/L) 1.00(1.00~1.00) 0.701 1.00(0.99~1.00) 0.680 AST(U/L) 1.00(1.00~1.01) 0.758 1.00(0.99~1.01) 0.603 病毒学相关指标 HBV DNA7) 0.68(0.31~1.50) 0.343 1.11(0.43~2.86) 0.831 HBsAg8) 1.88(0.65~5.45) 0.246 1.10(0.37~3.31) 0.863 HBeAg9) 0.41(0.18~0.90) 0.026 0.52(0.24~1.13) 0.100 0.69(0.29~1.64) 0.400 肝组织学特征 脂肪变性程度10) 1.46(0.66~3.22) 0.350 1.54(0.64~3.67) 0.333 气球样变11) 1.75(0.66~4.66) 0.264 2.07(0.80~5.39) 0.136 小叶内炎症12) 1.72(0.64~4.61) 0.280 1.09(0.32~3.74) 0.887 汇管区炎症13) 3.49(1.32~9.27) 0.012 2.92(0.98~8.75) 0.055 3.02(1.01~9.00) 0.048 2.19(0.70~6.91) 0.180 界面炎14) 2.43(1.10~5.35) 0.028 0.80(0.32~1.98) 0.623 1.33(0.56~3.14) 0.516 融合坏死15) 2.55(0.34~18.86) 0.361 0.05(0.00~18.80) 0.765 肝纤维化分期16) 5.10(2.36~11.00) <0.001 3.60(1.50~8.60) 0.004 3.75(1.59~8.87) 0.003 3.01(1.22~7.40) 0.016 窦周纤维化17) 1.53(0.36~6.48) 0.566 1.32(0.31~5.67) 0.714 炎症活动度18) 2.94(1.36~6.35) 0.006 2.02(0.86~4.76) 0.109 NAS 0.077 0.107 0~2分 1.00 1.00 3~4分 1.89 (0.85~4.22) 0.118 1.39(0.53~3.61) 0.502 5~8分 3.34(1.08~10.39) 0.037 3.58(1.10~11.66) 0.035 注:PSM,倾向评分匹配;Hb,血红蛋白;PLT,血小板;Alb,白蛋白;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;HBV,乙型肝炎病毒;HBsAg,乙型肝炎病毒表面抗原;HBeAg,乙型肝炎病毒e抗原;NAS,非酒精性脂肪性肝病活动度评分系统;HR,风险比;aHR,校正风险比;95%CI,95%置信区间;CHB-SLD,慢性乙型肝炎合并脂肪性肝病。计数资料赋值情况如下:1)性别:女=0,男=1;2)超重/肥胖:否=0,是=1;3)高血糖:无=0,有=1;4)高血压:无=0,有=1;5)高甘油三酯血症:无=0,有=1:6)高密度脂蛋白:正常=0,降低=1;7)HBV DNA定量:≤2 000 IU/mL=0,>2 000 IU/mL=1;8)HBsAg:<1 000 COI=0,≥1 000 COI=1;9)HBeAg:阴性=0,阳性=1;10)脂肪变性程度:轻度=0,中重度=1;11)气球样变:无=0,有=1;12)小叶内炎症:<2个/20倍镜=0,≥2个/20倍镜=1;13)汇管区炎症:无或轻度=0,中重度=1;14)界面炎:无=0,有=1;15)融合坏死:无=0,有=1;16)肝纤维化分期:≤F2=0,≥F3=1;17)窦周纤维化:无=0,有=1;18)炎症活动度:G0~1=0,G2~4=1。
下载: 导出CSV
表 5 CHB-SLD F3~4亚组人群发生终末期肝病的Cox回归分析
Table 5. Cox proportional-hazards regression for ESLD among subgroup of F3-4 patients
变量 单因素分析 多因素分析 HR(95%CI) P值 aHR(95%CI) P值 基本特征 年龄(岁) 1.032(0.985~1.081) 0.184 性别1) 0.707(0.204~2.447) 0.584 代谢特征 超重/肥胖2) 0.681(0.224~2.071) 0.499 高血糖3) 4.081(1.598~10.426) 0.003 3.208(1.201~8.568) 0.020 高血压4) 1.537(0.444~5.325) 0.498 高甘油三酯血症5) 0.851(0.306~2.366) 0.757 高密度脂蛋白降低6) 1.227(0.437~3.445) 0.698 生化指标 Hb(g/L) 0.987(0.961~1.012) 0.302 PLT(×109/L) 0.987(0.978~0.996) 0.005 0.994(0.984~1.004) 0.207 Alb(g/L) 0.865(0.783~0.955) 0.004 0.896(0.802~1.002) 0.054 ALT(U/L) 0.997(0.989~1.005) 0.500 AST(U/L) 1.004(0.995~1.013) 0.388 病毒学指标 HBV DNA7) 0.396(0.158~0.992) 0.048 0.388(0.149~1.009) 0.052 HBsAg8) 1.721(0.395~7.491) 0.469 HBeAg9) 0.638(0.252~1.617) 0.899 肝组织学特征 脂肪变性程度10) 1.044(0.396~2.751) 0.930 气球样变11) 1.338(0.477~3.758) 0.580 小叶内炎症12) 1.626(0.531~4.982) 0.395 汇管区炎症13) 5.947(0.791~44.718) 0.083 界面炎14) 1.633(0.528~5.045) 0.394 融合坏死15) 2.811(0.364~21.657) 0.322 窦周纤维化16) 0.727(0.097~5.470) 0.757 炎症活动度17) 2.117(0.801~5.594) 0.130 NAS 0.698 0~2分 1.000 3~4分 1.280(0.476~3.447) 0.625 5~8分 1.758(0.472~6.546) 0.401 注:Hb,血红蛋白;PLT,血小板;Alb,白蛋白;ALT,丙氨酸氨基转移酶;AST,天冬氨酸氨基转移酶;HBV,乙型肝炎病毒;HBsAg,乙型肝炎病毒表面抗原;HBeAg,乙型肝炎病毒e抗原;NAS,非酒精性脂肪性肝病活动度评分系统;HR,风险比;aHR,校正风险比;95%CI,95%置信区间;CHB-SLD,慢性乙型肝炎合并脂肪性肝病。计数资料赋值情况如下:1)性别:女=0,男=1;2)超重/肥胖:否=0,是=1;3)高血糖:否=0,是=1;4)高血压:否=0,是=1;5)高甘油三酯血症:否=0,是=1;6)高密度脂蛋白降低:否=0,是=1;7)HBV DNA定量:≤2 000 IU/mL=0,>2 000 IU/mL=1;8)HBsAg:<1 000 COI=0,≥1 000 COI=1;9)HBeAg:阴性=0,阳性=1;10)脂肪变性程度:轻度=0,中重度=1;11)气球样变:无=0,有=1;12)小叶内炎症:<2个/20倍镜=0,≥2个/20倍镜=1;13)汇管区炎症:无或轻度=0,中重度=1;14)界面炎:无=0,有=1;14)融合坏死:无=0,有=1;16)窦周纤维化:无=0,有=1;17)炎症活动度:G0~1=0,G2~4=1。
下载: 导出CSV
-
[1] Chinese Society of Hepatology, Chinese Medical Association; Chinese Society of Infectious Diseases, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B(version 2022)[J]. Infect Dis Info, 2023, 36( 1): 1- 17. DOI: 10.3969/j.issn.1007-8134.2023.01.01.中华医学会肝病学分会, 中华医学会感染病学分会. 慢性乙型肝炎防治指南(2022年版)[J]. 传染病信息, 2023, 36( 1): 1- 17. DOI: 10.3969/j.issn.1007-8134.2023.01.01. [2] RINELLA ME, LAZARUS JV, RATZIU V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature[J]. J Hepatol, 2023, 79( 6): 1542- 1556. DOI: 10.1016/j.jhep.2023.06.003. [3] LOU TW, YANG RX, FAN JG. The global burden of fatty liver disease: The major impact of China[J]. Hepatobiliary Surg Nutr, 2024, 13( 1): 119- 123. DOI: 10.21037/hbsn-23-556. [4] HUANG WS. The prevalence of metabolic dysfunction-associated fatty liver disease in Asia[J]. J Clin Hepatol, 2025, 41( 9): 1721- 1724. DOI: 10.12449/JCH250901.黄炜燊. 亚洲地区代谢相关脂肪性肝病流行情况[J]. 临床肝胆病杂志, 2025, 41( 9): 1721- 1724. DOI: 10.12449/JCH250901. [5] VITALE A, SVEGLIATI-BARONI G, ORTOLANI A, et al. Epidemiological trends and trajectories of MAFLD-associated hepatocellular carcinoma 2002-2033: The ITA.LI.CA database[J]. Gut, 2023, 72( 1): 141- 152. DOI: 10.1136/gutjnl-2021-324915. [6] YANG RX, QI MH. Antiviral strategy of patients with chronic hepatitis B and concomitant metabolic-dysfunction-related fatty liver diseases[J]. J Pract Hepatol, 2023, 26( 6): 773- 776. DOI: 10.3969/j.issn.1672-5069.2023.06.002.杨蕊旭, 齐明华. 慢性HBV感染合并代谢相关性脂肪性肝病患者抗病毒治疗对策[J]. 实用肝脏病杂志, 2023, 26( 6): 773- 776. DOI: 10.3969/j.issn.1672-5069.2023.06.002. [7] Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of metabolic dysfunction-associated(non-alcoholic) fatty liver disease(Version 2024)[J]. J Pract Hepatol, 2024, 27( 4): 494- 510.中华医学会肝病学分会. 代谢相关(非酒精性)脂肪性肝病防治指南(2024年版)[J]. 实用肝脏病杂志, 2024, 27( 4): 494- 510. [8] Fatty Liver Expert Committee, Chinese Medical Doctor Association, National Workshop on Fatty Liver and Alcoholic Liver Disease, Chinese Society of Hepatology, Chinese Medical Association. Guidelines of prevention and treatment for alcoholic liver disease: a 2018 update[J]. J Clin Hepatol, 2018, 34( 5): 939- 946. DOI: 10.3969/j.issn.1001-5256.2018.05.006.中国医师协会脂肪性肝病专家委员会, 中华医学会肝病学分会脂肪肝和酒精性肝病学组. 酒精性肝病防治指南(2018年更新版)[J]. 临床肝胆病杂志, 2018, 34( 5): 939- 946. DOI: 10.3969/j.issn.1001-5256.2018.05.006. [9] ISHAK K, BAPTISTA A, BIANCHI L, et al. Histological grading and staging of chronic hepatitis[J]. J Hepatol, 1995, 22( 6): 696- 699. DOI: 10.1016/0168-8278(95)80226-6. [10] KLEINER DE, BRUNT EM, VAN NATTA M, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease[J]. Hepatology, 2005, 41( 6): 1313- 1321. DOI: 10.1002/hep.20701. [11] JIANG DX, CHEN C, LIU XX, et al. Concurrence and impact of hepatic steatosis on chronic hepatitis B patients: A systematic review and meta-analysis[J]. Ann Transl Med, 2021, 9( 23): 1718. DOI: 10.21037/atm-21-3052. [12] LE MH, LE DM, BAEZ TC, et al. Global incidence of non-alcoholic fatty liver disease: A systematic review and meta-analysis of 63 studies and 1, 201, 807 persons[J]. J Hepatol, 2023, 79( 2): 287- 295. DOI: 10.1016/j.jhep.2023.03.040. [13] NAKATSUKA T, TATEISHI R. Development and prognosis of hepatocellular carcinoma in patients with diabetes[J]. Clin Mol Hepatol, 2023, 29( 1): 51- 64. DOI: 10.3350/cmh.2022.0095. [14] LIU K, LI JX, MA C, et al. The influence of diabetes mellitus and high‑sensitivity C‑reactive protein on the risk of diges-tive system malignancy: a prospective cohort study[J]. Chin J Dig Surg, 2025, 24( 1): 93- 102. DOI: 10.3760/cma.j.cn115610-20241022-00461.刘款, 李佳兴, 马超, 等. 糖尿病和高敏C反应蛋白水平影响消化系统恶性肿瘤发生风险的前瞻性队列研究[J]. 中华消化外科杂志, 2025, 24( 1): 93- 102. DOI: 10.3760/cma.j.cn115610-20241022-00461. [15] LI J, XU L, RUI FJ, et al. Type 2 diabetes mellitus as an independent predictor of significant fibrosis in treatment-naïve chronic hepatitis B patients with concurrent hepatic steatosis[J]. Hepatology, 2025. DOI: 10.1097/HEP.0000000000001442.[ Epub ahead of print] [16] PANG YJ, KARTSONAKI C, TURNBULL I, et al. Diabetes, plasma glucose, and incidence of fatty liver, cirrhosis, and liver cancer: A prospective study of 0.5 million people[J]. Hepatology, 2018, 68( 4): 1308- 1318. DOI: 10.1002/hep.30083. [17] PLAZ TORRES MC, JAFFE A, PERRY R, et al. Diabetes medications and risk of HCC[J]. Hepatology, 2022, 76( 6): 1880- 1897. DOI: 10.1002/hep.32439. [18] AJMERA V, CEPIN S, TESFAI K, et al. A prospective study on the prevalence of NAFLD, advanced fibrosis, cirrhosis and hepatocellular carcinoma in people with type 2 diabetes[J]. J Hepatol, 2023, 78( 3): 471- 478. DOI: 10.1016/j.jhep.2022.11.010. [19] HSIANG JC, GANE EJ, BAI WW, et al. Type 2 diabetes: A risk factor for liver mortality and complications in hepatitis B cirrhosis patients[J]. J Gastroenterol Hepatol, 2015, 30( 3): 591- 599. DOI: 10.1111/jgh.12790. [20] JIANG LN, ZHAO JM. Pathological mechanism of multi-organ injuries in metabolic dysfunction-associated fatty liver disease[J]. J Clin Hepatol, 2025, 41( 9): 1729- 1736. DOI: 10.12449/JCH250903.蒋丽娜, 赵景民. 代谢相关脂肪性肝病多器官损伤的病理机制[J]. 临床肝胆病杂志, 2025, 41( 9): 1729- 1736. DOI: 10.12449/JCH250903. [21] BYRNE CD, ARMANDI A, PELLEGRINELLI V, et al. Metabolic dysfunction-associated steatotic liver disease: A condition of heterogeneous metabolic risk factors, mechanisms and comorbidities requiring holistic treatment[J]. Nat Rev Gastroenterol Hepatol, 2025, 22( 5): 314- 328. DOI: 10.1038/s41575-025-01045-z. [22] RUGIVARODOM M, PONGPAIBUL A, CHAINUVATI S, et al. Prognostic relevance of metabolic dysfunction-associated steatohepatitis for patients with chronic hepatitis B[J]. J Clin Transl Hepatol, 2023, 11( 1): 76- 87. DOI: 10.14218/JCTH.2022.00055. [23] MAK LY, HUI RW, FUNG J, et al. Reduced hepatic steatosis is associated with higher risk of hepatocellular carcinoma in chronic hepatitis B infection[J]. Hepatol Int, 2021, 15( 4): 901- 911. DOI: 10.1007/s12072-021-10218-2. [24] LEE YB, HA Y, CHON YE, et al. Association between hepatic steatosis and the development of hepatocellular carcinoma in patients with chronic hepatitis B[J]. Clin Mol Hepatol, 2019, 25( 1): 52- 64. DOI: 10.3350/cmh.2018.0040. -

 本文二维码
本文二维码
计量
- 文章访问数: 175
- HTML全文浏览量: 64
- PDF下载量: 70
- 被引次数: 0

