
 PDF下载 ( 27884 KB)
PDF下载 ( 27884 KB)

基于Laennec膜的肝蒂CT三维重建及肝蒂鞘外分离阻闭钳的研发与验证
DOI: 10.12449/JCH251023
Three-dimensional CT reconstruction of the hepatic pedicle based on the Laennec’s capsule and the development and validation of extra-sheath dissection/occlusion clamp
-
摘要:
目的 探讨基于Laennec膜的肝蒂三维重建解剖特征,及其在鞘外分离阻闭钳研发和精准肝切除中的应用价值。 方法 回顾性分析2021年1月—2024年6月中国人民解放军西部战区总医院100例无肝蒂解剖异常患者的腹部增强CT资料,采用Hisense CAS系统结合3D U-net深度学习算法进行Laennec膜层面肝蒂三维重建,测量肝蒂主干及分支的长度、外径及角度。基于测量数据研发肝蒂鞘外分离阻闭钳,并纳入30例拟行右半肝切除患者,随机分为器械组(n=15)和对照组(n=15),比较两组肝蒂处理时间、手术时间、术中出血量及胆道损伤发生率。计量资料两组间比较采用成组t检验,计数资料两组间比较采用Fisher精确检验。 结果 三维重建显示肝蒂主干分支存在4种变异,其中Ⅰ型(左右分支型)占88%(88/100),Ⅱ型(三叉分支型)占5%(5/100),Ⅲ型(右前型)占5%(5/100),Ⅳ型(特殊型)占2%(2/100)。主肝蒂外径(24.10±6.16) mm,左支主干长度(20.59±6.38) mm,右支主干长度(21.99±7.98) mm。器械组肝蒂处理时间[(14.10±1.30) min vs (17.50±2.00) min, t=-5.620, P=0.001]及手术时间[(217.00±28.28) min vs (241.87±19.49) min, t=-2.804, P=0.009]显著短于对照组。器械组胆道损伤发生率显著低于对照组(0 vs 20%,P=0.031)。 结论 Laennec膜三维重建可精准呈现肝蒂解剖变异,基于该数据研发的鞘外分离阻闭钳可优化肝蒂处理流程,提高手术安全性,具有临床推广价值。 Abstract:Objective To investigate the anatomical features of three-dimensional (3D) reconstruction of the hepatic pedicle based on the Laennec’s capsule, as well as its application value in the development of extra-sheath dissection/occlusion clamp and precise hepatectomy. Methods A retrospective analysis was performed for the abdominal contrast-enhanced CT data of 100 patients without anatomical abnormalities of the hepatic pedicle in The General Hospital of Western Theater Command from January 2021 to June 2024. The Hisense CAS system combined with the 3D U-net deep learning algorithm was used for 3D reconstruction of the hepatic pedicle at the level of Laennec’s capsule, and the hepatic pedicle was measured in terms of the length, outer diameter, and angle of the main trunk and branches. An extra-sheath hepatic pedicle dissection/occlusion clamp was developed based on the above measurements, and a total of 30 patients scheduled for right hemihepatectomy were enrolled and randomly divided into device group and control group, with 15 patients in each group. The two groups were compared in terms of hepatic pedicle handling time, time of operation, intraoperative blood loss, and the incidence rate of bile duct injury. The independent-samples t test was used for comparison of continuous data between two groups, and the Fisher’s exact test was used for comparison of categorical data between two groups. Results The results of 3D reconstruction revealed four variants in the main trunk branches of the hepatic pedicle, with type Ⅰ (left-right branching) accounting for 88% (88/100), type Ⅱ (trifurcation type) accounting for 5% (5/100), type Ⅲ (right anterior branching) accounting for 5% (5/100), and type Ⅳ (special type) accounting for 2% (2/100). The outer diameter of the main hepatic pedicle was 24.10±6.16 mm, the length of the left main branch was 20.59±6.38 mm, and the length of the right main branch was 21.99±7.98 mm. Compared with the control group, the device group had significantly shorter hepatic pedicle handling time (14.10±1.30 minutes vs 17.50±2.00 minutes, t=-5.620, P=0.001) and time of operation (217.00±28.28 minutes vs 241.87±19.49 minutes, t=-2.804, P=0.009). The device group had a significantly lower incidence rate of bile duct injury than the control group (0 vs 20%, P=0.031). Conclusion 3D reconstruction based on the Laennec’s capsule can accurately display the anatomical variations of the hepatic pedicle. The extra-sheath hepatic pedicle dissection/occlusion clamp developed based on such data can optimize the process of hepatic pedicle management and improve surgical safety, and therefore, it holds promise for clinical application. -
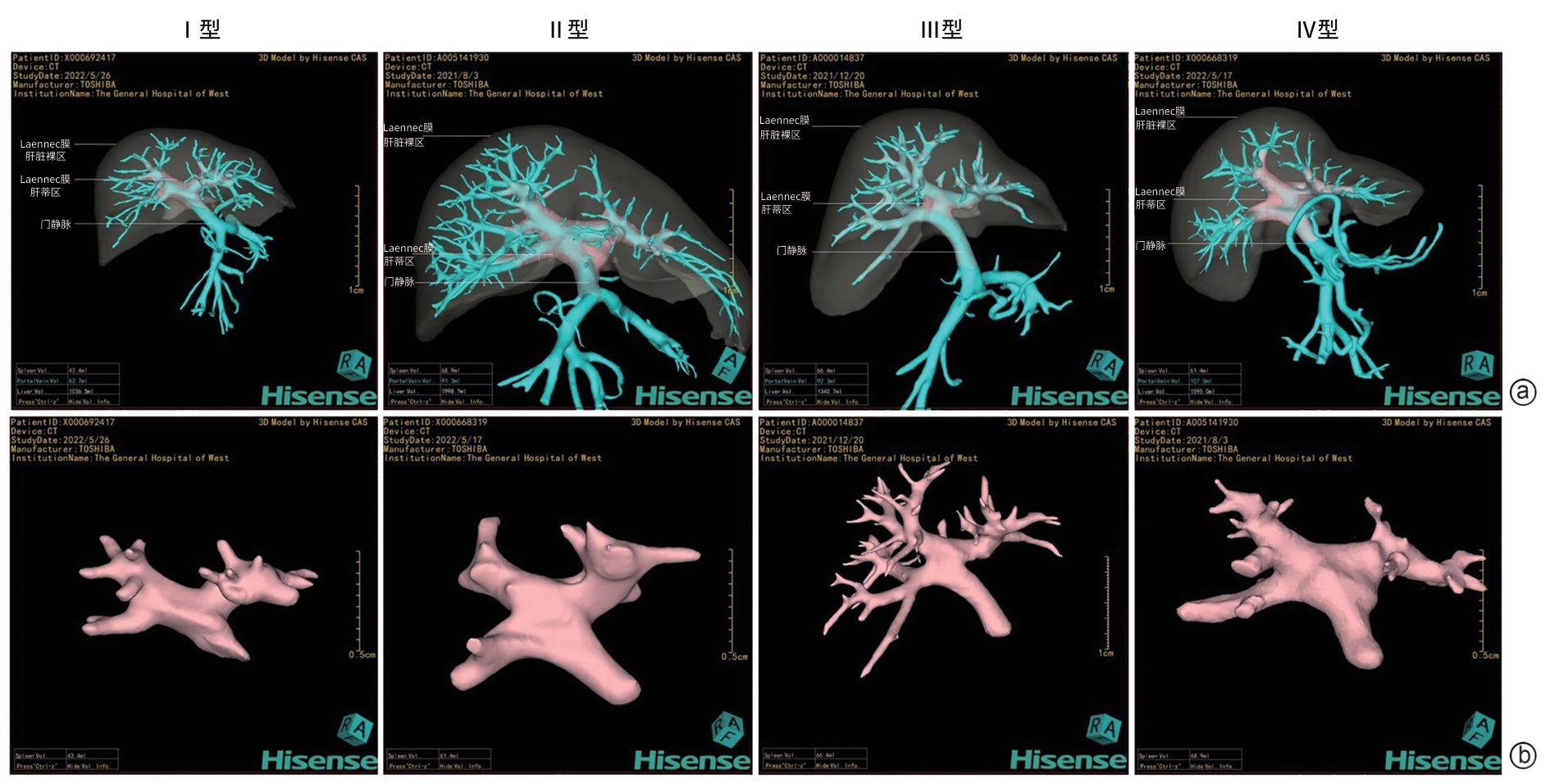
注: a,蓝色管道为重建的入肝门静脉系统;b,粉色为肝脏Laennec膜,包括肝脏裸区及肝蒂区,静脉、动脉及胆管均包绕于其中。
图 1 基于Laennec膜的肝蒂分支模式分类
Figure 1. Classification of hepatic pedicle branching patterns based on Laennec’s capsule

注: a,定钳头;b,动钳头;c,分离阻闭钳。
图 2 肝蒂鞘外解剖分离阻闭钳设计图
Figure 2. Design drawing of extrahepatic pedide dissection and occlusion clamp
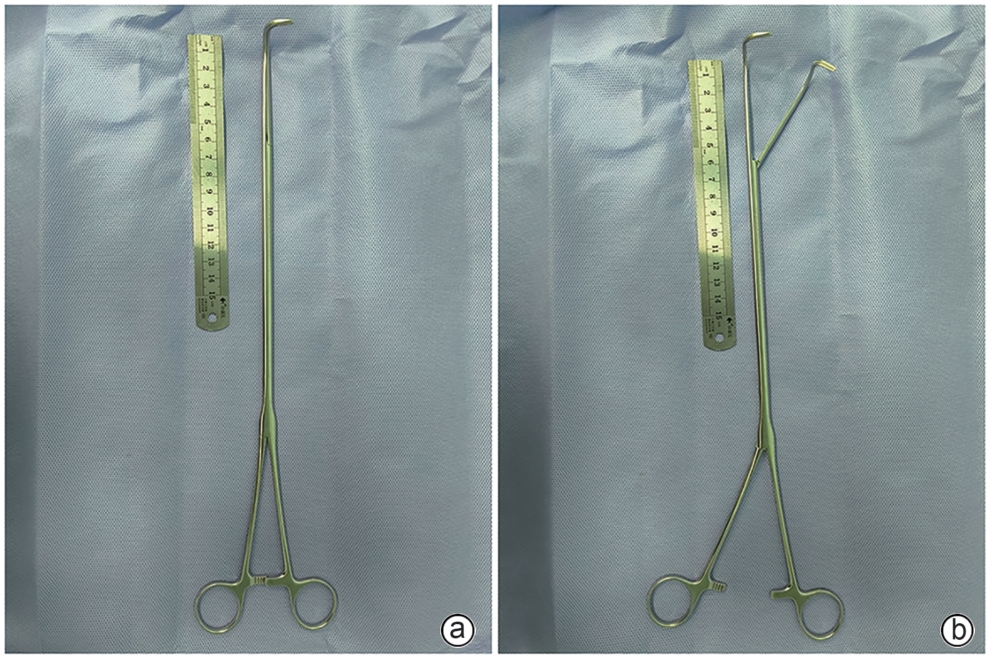
注: a,钳夹状态;b,分离状态。
图 3 肝蒂鞘外解剖分离阻闭钳实物图
Figure 3. Physical image of extrahepatic pedicle dissection and occlusion clamp

图 4 肝蒂鞘外解剖分离阻闭钳术中使用
Figure 4. Intraoperative use of the extrahepatic pedicle dissection and occlusion clamp
表 1 基于Laennec膜三维重建的100例肝蒂长度和外径
Table 1. Three-dimensional reconstruction-based measure‑ments of hepatic pedicle length and outer diameter in 100 cases using Laennec’s membrane
项目 数值(mm) 标准误 主干 外径 24.10±6.16 0.69 左支主干 长度 20.59±6.38 0.72 外径 18.04±4.48 0.50 右支主干 长度 21.99±7.98 0.97 外径 21.18±4.23 0.52 右前主干 长度 13.20±5.43 0.68 外径 15.25±3.39 0.39 右后主干 长度 12.03±4.13 0.63 外径 13.01±2.80 0.40  下载: 导出CSV
下载: 导出CSV
表 2 基于Laennec膜三维重建的100例肝蒂角度
Table 2. Hepatic pedicle angle measurements based on Laennec’s membrane 3D reconstruction in 100 cases
项目 数值 标准误 ALM 114.35°±22.91° 2.61 ARM 140.81°±16.72° 2.49 ALR 142.63°±15.66° 1.89 注:ALM,肝蒂与左主干夹角;ARM,肝蒂与右主干夹角;ALR,左右主支夹角。
下载: 导出CSV
表 3 两组患者术中的统计结果对比
Table 3. Comparison of intraoperative outcomes between the two groups
项目 器械组(n=15) 对照组(n=15) 统计值 P值 肝蒂处理时间(min) 14.10±1.30 17.50±2.00 t=-5.620 0.001 手术时间(min) 217.00±28.28 241.87±19.49 t=-2.804 0.009 出血量(mL) 333.30±97.59 353.30±99.04 t=-0.557 0.582 胆道损伤[例(%)] 0(0) 3(20) 0.031
下载: 导出CSV
-
[1] COUINAUD C. Liver lobes and segments: Notes on the anatomical architecture and surgery of the liver[J]. Presse Med( 1893), 1954, 62( 33): 709- 712. [2] MORIMOTO M, MATSUO Y, NONOYAMA K, et al. Glissonean pedicle isolation focusing on the laennec’s capsule for minimally invasive anatomical liver resection[J]. J Pers Med, 2023, 13( 7): 1154. DOI: 10.3390/jpm13071154. [3] EGUCHI S, KANEMATSU T, ARII S, et al. Comparison of the outcomes between an anatomical subsegmentectomy and a non-anatomical minor hepatectomy for single hepatocellular carcinomas based on a Japanese nationwide survey[J]. Surgery, 2008, 143( 4): 469- 475. DOI: 10.1016/j.surg.2007.12.003. [4] WANG K, SUN SB, LI ZX, et al. Application value of cystic plate approach for extrahepatic right hepatic pedicle dissection in minimally invasive anatomic liver resection[J]. Chin J Dig Surg, 2023, 22( 4): 489- 496. DOI: 10.3760/cma.j.cn115610-20230321-00119.王恺, 孙世波, 李芷西, 等. 胆囊板入路右肝蒂鞘外解剖法在微创解剖性肝切除术中的应用价值[J]. 中华消化外科杂志, 2023, 22( 4): 489- 496. DOI: 10.3760/cma.j.cn115610-20230321-00119. [5] SHIRATA C, KOKUDO T, GILLET M, et al. Reappraisal of laennec’s capsule[J]. Surg Oncol, 2020, 33: 222- 223. DOI: 10.1016/j.suronc.2019.08.004. [6] SUGIOKA A, KATO Y, TANAHASHI Y. Systematic extrahepatic Glissonean pedicle isolation for anatomical liver resection based on Laennec’s capsule: Proposal of a novel comprehensive surgical anatomy of the liver[J]. J Hepatobiliary Pancreat Sci, 2017, 24( 1): 17- 23. DOI: 10.1002/jhbp.410. [7] MONDEN K, OHNO K, HAYASHI S, et al. Hepatic vein anatomy related to Laennec’s capsule for liver resection[J]. J Hepatobiliary Pancreat Sci, 2023, 30( 5): 551- 557. DOI: 10.1002/jhbp.1250. [8] SHENG WW, YUAN CD, WU LQ, et al. Clinical application of a three-dimensional reconstruction technique for complex liver cancer resection[J]. Surg Endosc, 2022, 36( 5): 3246- 3253. DOI: 10.1007/s00464-021-08636-2. [9] LAI JL, WU JY, BAI YN, et al. A novel Laennec’s capsule tunnel approach for pure laparoscopic left hemihepatectomy: A propensity score matching study[J]. Front Surg, 2023, 10: 1136908. DOI: 10.3389/fsurg.2023.1136908. [10] ZHANG H, ZHOU TY, LIU H, et al. Clinical application of hepatic portal vein anatomy and three-dimensional reconstruction of images[J]. Acta Anat Sin, 2020, 51( 6): 919- 923. DOI: 10.16098/j.issn.0529-1356.2020.06.017.张慧, 周庭永, 刘晖, 等. 肝门静脉解剖和影像三维重建的临床应用[J]. 解剖学报, 2020, 51( 6): 919- 923. DOI: 10.16098/j.issn.0529-1356.2020.06.017. [11] HONG HY, CHEN ZJ, CHI XB, et al. Comparative study of extrathecal and intrathecal Glisson’s pedicle transection in laparoscopic anatomic hepatectomy[J/OL]. Chin J Hepatic Surg Electron Ed, 2024, 13( 1): 21- 26.洪汉崟, 陈志坚, 池小斌, 等. 鞘外法和鞘内法Glisson蒂阻断在腹腔镜解剖性肝切除中应用的对比研究[J/OL]. 中华肝脏外科手术学电子杂志, 2024, 13( 1): 21- 26. [12] KIGUCHI G, SUGIOKA A, KATO Y, et al. Use of the inter-Laennec approach for laparoscopic anatomical right posterior sectionectomy in semi-prone position[J]. Surg Oncol, 2019, 29: 140- 141. DOI: 10.1016/j.suronc.2019.05.001. [13] MONDEN K, SADAMORI H, HIOKI M, et al. Laparoscopic anatomic segmentectomy 8 using the outer-Laennec approach[J]. Surg Oncol, 2020, 35: 299- 300. DOI: 10.1016/j.suronc.2020.08.029. [14] HU W, ZHANG GM, CHEN M, et al. Laennec’s approach for laparoscopic anatomical hemihepatectomy[J]. World J Surg Oncol, 2021, 19( 1): 295. DOI: 10.1186/s12957-021-02404-1. [15] ZHANG CH, MA JL, ZHOU Y. Laparoscopic dissection of the first and second porta hepatis along Laennec’s capsule via“Hepatic Serosal Incision” approach: How I do it[J]. World J Surg, 2024, 48( 8): 1967- 1972. DOI: 10.1002/wjs.12255. [16] YANG Y, YU CY, LIN F, et al. Application of Laennec extrathecal blockade combined with indocyanine green fluorescence imaging in laparoscopic anatomic hepatectomy[J]. ANZ J Surg, 2024, 94( 4): 655- 659. DOI: 10.1111/ans.18907. [17] LI BH, YIN DL, ZHANG QF, et al. Laennec approach for anatomical liver resection assisted by laparoscopy or robotics: A multicenter cohort study[J]. Int J Surg, 2025, 111( 2): 1929- 1938. DOI: 10.1097/JS9.0000000000002212. [18] JIANG C, WANG HJ, REN L, et al. Application status of three- dimensional CT reconstruction in hepatobiliary surgery[J]. J Clin Hepatol, 2017, 33( 2): 389- 393. DOI: 10.3969/j.issn.1001-5256.2017.02.041.姜超, 王海久, 任利, 等. CT三维重建在肝胆外科的应用现状[J]. 临床肝胆病杂志, 2017, 33( 2): 389- 393. DOI: 10.3969/j.issn.1001-5256.2017.02.041. [19] ZHANG YP, SHI N, ZOU YP, et al. The characteristics of Laennec’s capsule around the hepatic veins: A histological study based on 71 liver surgical specimens[J]. Ann Gastroenterol Surg, 2022, 7( 2): 287- 294. DOI: 10.1002/ags3.12618. [20] HU Y, SHI J, WANG SH, et al. Laennec’s approach for laparoscopic anatomic hepatectomy based on Laennec’s capsule[J]. BMC Gastroenterol, 2019, 19( 1): 194. DOI: 10.1186/s12876-019-1107-9. [21] CAO SD, LI H, DONG SY, et al. Feasibility study of intelligent three-dimensional accurate liver reconstruction technology based on MRI data[J]. Front Med(Lausanne), 2022, 9: 834555. DOI: 10.3389/fmed.2022.834555. [22] HUANG XL, LU S. A Meta-analysis comparing the effect of anatomical resection vs. non-anatomical resection on the long-term outcomes for patients undergoing hepatic resection for hepatocellular carcinoma[J]. HPB(Oxford), 2017, 19( 10): 843- 849. DOI: 10.1016/j.hpb.2017.06.003. [23] KANG WH, KIM KH, JUNG DH, et al. Long-term results of laparoscopic liver resection for the primary treatment of hepatocellular carcinoma: Role of the surgeon in anatomical resection[J]. Surg Endosc, 2018, 32( 11): 4481- 4490. DOI: 10.1007/s00464-018-6194-0. -

 本文二维码
本文二维码
计量
- 文章访问数: 386
- HTML全文浏览量: 119
- PDF下载量: 90
- 被引次数: 0

