
 PDF下载 ( 968 KB)
PDF下载 ( 968 KB)

血小板-白蛋白-胆红素评分对肝细胞癌患者肝切除术后教科书式结局的影响
DOI: 10.12449/JCH250519
Influence of platelet-albumin-bilirubin score on textbook outcome of patients with hepatocellular carcinoma after hepatectomy
-
摘要:
目的 血小板-白蛋白-胆红素(PALBI)评分对肝细胞癌(HCC)患者肝切除术后获得教科书式结局(TO)的影响尚不清楚。拟探索术前不同PALBI评分分级与HCC患者肝切除术后获得TO的关系。 方法 回顾性收集四川大学华西医院和资阳市中心医院2013年1月—2022年1月行肝切除术的HCC患者资料。TO定义为无术后30 d内严重并发症、无90 d内患者死亡、无出院后30 d内再住院、无围手术期输血、R0切除、无住院时间延长。计数资料两组间比较采用χ2检验。单因素和多因素Logistic回归分析HCC患者肝切除术后获得TO的影响因素。采用Kaplan-Meier法绘制HCC患者生存曲线,并通过Log-rank检验进行比较。 结果 共3 599例患者纳入研究,其中2 369例(65.8%)患者获得TO。多因素Logistic回归分析结果显示,PALBI评分分级(PALBI 2级:OR=1.562,95%CI:1.308~1.864,P<0.001;PALBI 3级:OR=2.216,95%CI:1.463~3.359,P<0.001)是影响HCC患者术后获得TO的独立危险因素。随着PALBI分级增加,患者获得TO的比率降低。PALBI 1级、2级和3级患者获得TO的比率分别为70.2%、54.2%和38.4%,差异有统计学意义(χ2=106.295,P<0.001)。30 d内严重并发症发生率、术后90 d内患者病死率、出院后30 d内再住院率、围手术期输血率、住院时间延长率均随着PALBI评分分级的增加而增加(P值均<0.05)。获得TO患者术后1、3、5年无复发生存率分别为79.5%、60.6%和51.5%,总生存率分别为92.1%、80.0%和71.1%;未获得TO患者术后1、3、5年无复发生存率分别为68.5%、52.7%和46.2%,总生存率分别为83.3%、66.0%和57.1%。获得TO的患者无复发生存率和总生存率均显著好于未获得TO的患者(χ2值分别为18.936、79.371,P值均<0.001)。 结论 术前PALBI评分分级影响HCC患者肝切除术后获得TO,PALBI分级越高的患者术后越不易获得TO。通过术前PALBI评分评估,有利于早期发现术后并发症发生的高危人群,提早干预,加强围手术期管理,从而提高患者围手术期安全性和长期预后。 -
关键词:
- 癌, 肝细胞 /
- 血小板-白蛋白-胆红素评分 /
- 教科书式结局
Abstract:Objective To investigate the influence of platelet-albumin-bilirubin (PALBI) score on the textbook outcome (TO) of patients with hepatocellular carcinoma (HCC) after hepatectomy, as well as the association of different PALBI scores before surgery with the achievement of TO after hepatectomy in HCC patients. Methods A retrospective analysis was performed for the data of HCC patients who underwent hepatectomy in West China Hospital of Sichuan University and Ziyang Central Hospital from January 2013 to January 2022. TO was defined as no serious complication within 30 days after surgery, no death within 90 days, no rehospitalization within 30 days after discharge, no blood transfusion in the perioperative period, RO resection, and no prolongation of hospital stay. The chi-square test was used for comparison of categorical data between two groups. The univariate and multivariate Logistic regression analyses were used to investigate the influencing factors for the achievement of TO after hepatectomy in HCC patients. The Kaplan-Meier method was used to plot the survival curves of HCC patients, and the Log-rank test was used for comparison. Results A total of 3 599 patients were included in this study, among whom 2 369 (65.8%) achieved TO. The multivariate Logistic regression analysis showed that PALBI grade (PALBI grade 2: odds ratio [OR]=1.562, 95% confidence interval [CI]: 1.308 — 1.864, P<0.001; PALBI grade 3: OR=2.216, 95%CI: 1.463 — 3.359, P<0.001) was an independent risk factor for achievement of TO after surgery in HCC patients. The proportion of patients achieving TO decreased with the increase in PALBI grade. Among the patients with PALBI grade 1, 2 or 3, the patients achieving TO accounted for 70.2%, 54.2%, and 38.4%, respectively (χ2=106.295, P<0.001). The incidence rate of serious complications within 30 days, the mortality rate of patients within 90 days after hepatectomy, readmission rate within 30 days after discharge, perioperative blood transfusion rate, and the rate of prolonged hospital stay all increased with the increase in PALBI grade (all P<0.05). For the patients achieving TO, the 1-, 3-, and 5-year relapse-free survival rates were 79.5%, 60.6%, and 51.5%, respectively, and the overall survival rates were 92.1%, 80.0%, and 71.1%, respectively; for those who did not achieve TO, the 1-, 3-, and 5-year relapse-free survival rates were 68.5%, 52.7%, and 46.2%, respectively, and the overall survival rates were 83.3%, 66.0%, and 57.1%, respectively. The patients who achieved TO had significantly better relapse-free survival rate and overall survival rate than those who did not achieve TO (χ2=18.936 and 79.371, both P<0.001). Conclusion Preoperative PALBI grade can affect the achievement of TO after hepatectomy in HCC patients, and it is more difficult for patients with a higher PALBI grade to achieve TO. Preoperative PALBI score can be used to early identify the patients with a high risk of postoperative complications, provide early intervention, and enhance perioperative management, thereby improving the perioperative safety and long-term prognosis of HCC patients after hepatectomy. -
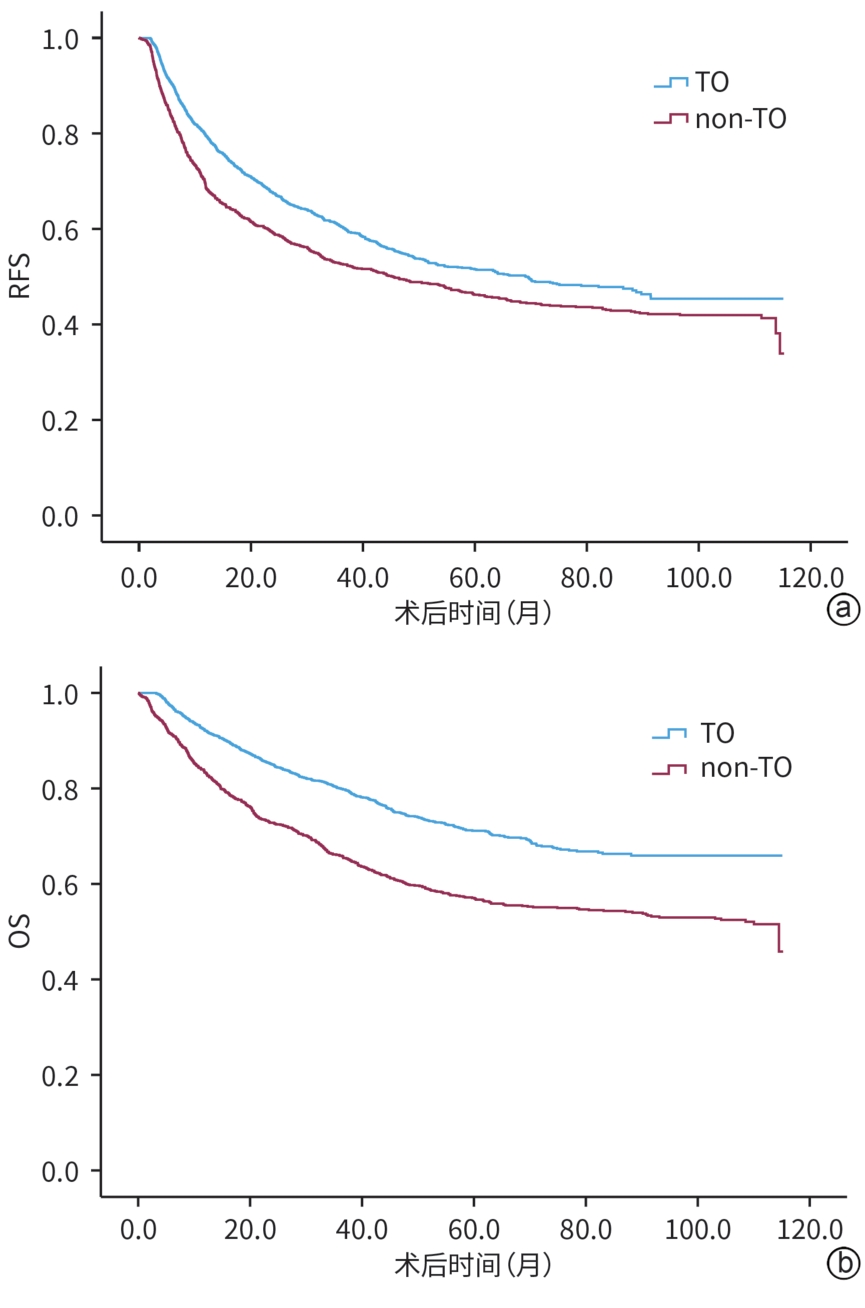
图 1 TO与非TO患者RFS及OS的比较
Figure 1. Comparison of recurrence-free survival and overall survival between TO and non-TO patients
表 1 不同PALBI评分分级患者基线临床病理特征比较
Table 1. Comparison of the baseline clinicopathological characteristics of patients with different PALBI grades
项目 PALBI 1级(n=2 730) PALBI 2级(n=757) PALBI 3级(n=112) χ2值 P值 男[例(%)] 2 314(84.8) 656(86.7) 98(87.5) 2.161 0.339 年龄>65岁[例(%)] 474(17.4) 130(17.2) 17(15.2) 0.364 0.834 AFP>400 ng/mL[例(%)] 939(34.4) 315(41.6) 59(52.7) 26.403 <0.001 PNI<45[例(%)] 247(9.0) 258(34.1) 75(67.0) 495.853 <0.001 HBV DNA阳性[例(%)] 1 025(37.5) 343(45.3) 67(59.8) 34.093 <0.001 肿瘤直径>5 cm[例(%)] 1 164(42.6) 451(59.6) 84(75.0) 104.069 <0.001 肝内多发肿瘤[例(%)] 276(10.1) 74(9.8) 19(17.0) 5.731 0.057 ALBI 2级[例(%)] 420(15.4) 489(64.6) 107(95.5) 966.901 <0.001 MVI阳性[例(%)] 936(34.3) 309(40.8) 62(55.4) 29.061 <0.001 肿瘤低分化[例(%)] 276(10.1) 113(14.9) 20(17.9) 18.493 <0.001 BCLC B/C期[例(%)] 433(15.9) 157(20.7) 32(28.6) 20.173 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 肝切除术后影响HCC患者获得TO的危险因素分析
Table 2. Risk factors affecting TO achievement in HCC patients after hepatectomy
项目 单因素分析 多因素分析 OR 95%CI P值 OR 95%CI P值 男性 1.110 0.912~1.351 0.299 年龄>65岁 0.972 0.810~1.167 0.764 AFP>400 ng/mL 1.403 1.218~1.617 <0.001 HBV DNA阳性 1.089 0.946~1.253 0.234 血小板计数<50×109/L 1.365 1.010~1.864 0.043 1.507 1.096~2.072 0.012 PNI<45 2.346 1.960~2.810 <0.001 1.696 1.387~2.073 <0.001 ALBI 2级 1.994 1.717~2.316 <0.001 肿瘤直径>5 cm 2.290 1.989~2.636 <0.001 1.889 1.622~2.200 <0.001 多发肿瘤 1.067 0.852~1.337 0.571 MVI阳性 1.712 1.486~1.973 <0.001 1.293 1.107~1.510 0.001 肿瘤低分化 1.244 1.006~1.538 0.044 BCLC分期(B/C vs 0/A) 1.848 1.550~2.202 <0.001 1.398 1.158~1.687 <0.001 PALBI 1级 1.000 1.000 PALBI 2级 1.992 1.689~2.349 <0.001 1.562 1.308~1.864 <0.001 PALBI 3级 3.777 2.558~5.576 <0.001 2.216 1.463~3.359 <0.001
下载: 导出CSV
表 3 不同PALBI评分分级患者非TO指标情况的比较
Table 3. Comparison of each type of non-TO among patients with different PALBI grades
项目 PALBI 1级(n=2 730) PALBI 2级(n=757) PALBI 3级(n=112) χ2值 P值 术后90 d内死亡 32(1.2) 21(2.8) 4(3.6) 12.688 0.002 非R0切除 108(4.0) 28(3.7) 6(5.4) 0.711 0.701 围手术期输血 151(5.5) 88(11.6) 28(25.0) 84.065 <0.001 术后30 d内严重并发症 123(4.5) 54(7.1) 18(16.1) 33.588 <0.001 出院后30 d内再住院 15(0.5) 7(0.9) 3(2.7) 7.806 0.020 住院时间延长 600(22.0) 269(35.5) 49(43.8) 77.574 <0.001
下载: 导出CSV
-
[1] SAYINER M, GOLABI P, YOUNOSSI ZM. Disease burden of hepatocellular carcinoma: A global perspective[J]. Dig Dis Sci, 2019, 64( 4): 910- 917. DOI: 10.1007/s10620-019-05537-2. [2] RUMGAY H, ARNOLD M, FERLAY J, et al. Global burden of primary liver cancer in 2020 and predictions to 2040[J]. J Hepatol, 2022, 77( 6): 1598- 1606. DOI: 10.1016/j.jhep.2022.08.021. [3] D’ASSIGNIES G, FAYARD C, LEITAO H, et al. Liver steatosis assessed by preoperative MRI: An independent risk factor for severe complications after major hepatic resection[J]. Surgery, 2016, 159( 4): 1050- 1057. DOI: 10.1016/j.surg.2015.10.008. [4] PECQUEUX M, BRÜCKNER F, BOGNER A, et al. Interleukin-8 is superior to CRP for the prediction of severe complications in a prospective cohort of patients undergoing major liver resection[J]. Langenbecks Arch Surg, 2023, 408( 1): 377. DOI: 10.1007/s00423-023-03041-w. [5] KIM BJ, TZENG CD, COOPER AB, et al. Borderline operability in hepatectomy patients is associated with higher rates of failure to rescue after severe complications[J]. J Surg Oncol, 2017, 115( 3): 337- 343. DOI: 10.1002/jso.24506. [6] WANG FM, LU JM, YANG T, et al. Perioperative changes in serum transaminase levels: Impact on postoperative morbidity following liver resection of hepatocellular carcinoma[J]. Ann Surg, 2025, 281( 4): 624- 631. DOI: 10.1097/SLA.0000000000006235. [7] LI LQ, LIANG L, SUN LY, et al. Postoperative morbidity adversely impacts long-term oncologic prognosis following hepatectomy for hepatocellular carcinoma: A multicenter observational study[J]. Eur J Surg Oncol, 2021, 47( 10): 2551- 2560. DOI: 10.1016/j.ejso.2021.04.027. [8] LIU ZP, YAO LQ, DIAO YK, et al. Association of preoperative body mass index with surgical textbook outcomes following hepatectomy for hepatocellular carcinoma: A multicenter study of 1 206 patients[J]. Ann Surg Oncol, 2022, 29: 4278- 4286. DOI: 10.1245/s10434-022-11721-y. [9] KOLFSCHOTEN NE, KIEVIT J, GOOIKER GA, et al. Focusing on desired outcomes of care after colon cancer resections; hospital variations in‘textbook outcome’[J]. Eur J Surg Oncol, 2013, 39( 2): 156- 163. DOI: 10.1016/j.ejso.2012.10.007. [10] Oesophago-Gastric Anastomotic Audit(OGAA) Collaborative. Textbook outcome following oesophagectomy for cancer: International cohort study[J]. Br J Surg, 2022, 109( 5): 439- 449. DOI: 10.1093/bjs/znac016. [11] BONNET J, SCATTON O, GOUMARD C, et al. Patients’ perceptions of the definition of a textbook outcome following liver transplantation[J]. HPB(Oxford), 2023, 25( 12): 1523- 1530. DOI: 10.1016/j.hpb.2023.07.905. [12] van ROESSEL S, MACKAY TM, van DIEREN S, et al. Textbook outcome: Nationwide analysis of a novel quality measure in pancreatic surgery[J]. Ann Surg, 2020, 271( 1): 155- 162. DOI: 10.1097/SLA.0000000000003451. [13] LIU PH, HSU CY, HSIA CY, et al. ALBI and PALBI grade predict survival for HCC across treatment modalities and BCLC stages in the MELD Era[J]. J Gastroenterol Hepatol, 2017, 32( 4): 879- 886. DOI: 10.1111/jgh.13608. [14] HE LY, XIA ZJ, ZHANG XY, et al. Tenofovir versus entecavir on the prognosis of hepatitis B-related hepatocellular carcinoma after surgical resection: A randomised controlled trial[J]. Int J Surg, 2023, 109( 10): 3032- 3041. DOI: 10.1097/JS9.0000000000000554. [15] QI WL, SHEN JY, ZHANG Y, et al. Effects of viral load on tenofovir vs. entecavir efficacy in recurrence prevention of hepatitis B virus-related hepatocellular carcinoma[J]. Chin Med J(Engl), 2023, 136( 19): 2362- 2364. DOI: 10.1097/CM9.0000000000002433. [16] JOHNSON PJ, BERHANE S, KAGEBAYASHI C, et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade[J]. J Clin Oncol, 2015, 33( 6): 550- 558. DOI: 10.1200/JCO.2014.57.9151. [17] YU JJ, LIANG L, LU L, et al. Association between body mass index and postoperative morbidity after liver resection of hepatocellular carcinoma: A multicenter study of 1,324 patients[J]. HPB(Oxford), 2020, 22( 2): 289- 297. DOI: 10.1016/j.hpb.2019.06.021. [18] QIU ZC, DAI JL, ZHANG Y, et al. Association of the number of concurrent metabolic syndrome risk factors with textbook outcomes following liver resection for patients with hepatocellular carcinoma: A multicenter study[J]. Ann Surg Oncol, 2025, 32( 1): 399- 407. DOI: 10.1245/s10434-024-16343-0.X [19] QIN L, LI C, XIE F, et al. Combination of albumin-bilirubin grade and clinically significant portal hypertension predicts the prognosis of patients with hepatocellular carcinoma after liver resection[J]. Biosci Trends, 2021, 15( 1): 41- 49. DOI: 10.5582/bst.2021.01064. [20] CHEN ZX, CHEN JM, GUO Q, et al. Influencing factors analysis of textbook outcome after hepatectomy for hepatolithiasis[J]. Chin J Dig Surg, 2023, 22( S1): 28- 33. DOI: 10.3760/cma.j.cn115610-20230906-00061.陈子祥, 陈江明, 郭旗, 等. 肝胆管结石病肝切除术后教科书式结局的影响因素分析[J]. 中华消化外科杂志, 2023, 22( S1): 28- 33. DOI: 10.3760/cma.j.cn115610-20230906-00061. [21] LIN GT, CHEN JY, SHANG-GUAN ZX, et al. Robot-assisted versus laparoscopic-assisted gastrectomy among malnourished patients with gastric cancer based on textbook outcome[J]. Surg Endosc, 2024, 38( 5): 2666- 2676. DOI: 10.1007/s00464-024-10769-z. [22] XU SJ, LIN LQ, CHEN TY, et al. Nomogram for prognosis of patients with esophageal squamous cell cancer after minimally invasive esophagectomy established based on non-textbook outcome[J]. Surg Endosc, 2022, 36( 11): 8326- 8339. DOI: 10.1007/s00464-022-09290-y. [23] LIU H, DIAO YK, WEI F, et al. Stratifying risk of failure to achieve textbook outcomes among patients undergoing hepatectomy for hepatocellular carcinoma: A multicenter score validation study[J]. Eur J Surg Oncol, 2024, 50( 9): 108477. DOI: 10.1016/j.ejso.2024.108477. [24] TSILIMIGRAS DI, MEHTA R, MERATH K, et al. Hospital variation in textbook outcomes following curative-intent resection of hepatocellular carcinoma: An international multi-institutional analysis[J]. HPB(Oxford), 2020, 22( 9): 1305- 1313. DOI: 10.1016/j.hpb.2019.12.005. [25] XU FQ, YE TW, WANG DD, et al. Association of preoperative albumin-bilirubin with surgical textbook outcomes following laparoscopic hepatectomy for hepatocellular carcinoma[J]. Front Oncol, 2022, 12: 964614. DOI: 10.3389/fonc.2022.964614. [26] KANEKO K, SHIRAI Y, WAKAI T, et al. Low preoperative platelet counts predict a high mortality after partial hepatectomy in patients with hepatocellular carcinoma[J]. World J Gastroenterol, 2005, 11( 37): 5888- 5892. DOI: 10.3748/wjg.v11.i37.5888. [27] KONDO K, CHIJIIWA Y, OTANI K, et al. Characteristics and surgical outcome of HCC patients with low platelet count[J]. Hepatogastroenterology, 2012, 59( 119): 2269- 2272. DOI: 10.5754/hge10649. [28] LESURTEL M, RAPTIS DA, MELLOUL E, et al. Low platelet counts after liver transplantation predict early posttransplant survival: The 60-5 criterion[J]. Liver Transpl, 2014, 20( 2): 147- 155. DOI: 10.1002/lt.23759. [29] ENDO Y, TSILIMIGRAS DI, MUNIR MM, et al. Prognostic significance of postoperative complications for patients with hepatocellular carcinoma relative to alpha-feto protein and tumor burden score[J]. HPB(Oxford), 2024, 26( 8): 998- 1006. DOI: 10.1016/j.hpb.2024.04.013. [30] QI WL, DAI JL, QIU ZC, et al. Nomogram to predict liver surgery-specific complications for hepatocellular carcinoma: A multicenter study[J]. Eur J Surg Oncol, 2023, 49( 12): 107119. DOI: 10.1016/j.ejso.2023.107119. [31] MIYATA T, MATSUMOTO T, NAKAO Y, et al. Major postoperative complications are associated with early recurrence of hepatocellular carcinoma following hepatectomy[J]. Langenbecks Arch Surg, 2022, 407( 6): 2373- 2380. DOI: 10.1007/s00423-022-02513-9. [32] NAKAYAMA H, OKAMURA Y, HIGAKI T, et al. Effect of blood product transfusion on the prognosis of patients undergoing hepatectomy for hepatocellular carcinoma: A propensity score matching analysis[J]. J Gastroenterol, 2023, 58( 2): 171- 181. DOI: 10.1007/s00535-022-01946-9. [33] PENG T, WANG LM, CUI HY, et al. Impact of perioperative allogeneic blood transfusion on the long-term prognosis of patients with different stage tumors after radical resection for hepatocellular carcinoma[J]. Eur J Surg Oncol, 2021, 47( 3 Pt B): 620- 627. DOI: 10.1016/j.ejso.2020.09.021. [34] HAYASHI H, SHIMIZU A, KUBOTA K, et al. Combination of sarcopenia and prognostic nutritional index to predict long-term outcomes in patients undergoing initial hepatectomy for hepatocellular carcinoma[J]. Asian J Surg, 2023, 46( 2): 816- 823. DOI: 10.1016/j.asjsur.2022.07.122. [35] KORNBERG A, KASCHNY L, KORNBERG J, et al. Preoperative prognostic nutritional index may be a strong predictor of hepatocellular carcinoma recurrence following liver transplantation[J]. J Hepatocell Carcinoma, 2022, 9: 649- 660. DOI: 10.2147/JHC.S366107. [36] PAN JY, CHEN SC, TIAN G, et al. Preoperative albumin-bilirubin grade with prognostic nutritional index predicts the outcome of patients with early-stage hepatocellular carcinoma after percutaneous radiofrequency ablation[J]. Front Med(Lausanne), 2020, 7: 584871. DOI: 10.3389/fmed.2020.584871. [37] NAGATA S, MAEDA S, NAGAMATSU S, et al. Prognostic nutritional index considering resection range is useful for predicting postoperative morbidity of hepatectomy[J]. J Gastrointest Surg, 2021, 25( 11): 2788- 2795. DOI: 10.1007/s11605-020-04893-z. [38] HAO Y, XIE F, ZHOU YJ, et al. Neoadjuvant therapy of sequential TACE, camrelizumab, and apatinib for single huge hepatocellular carcinoma(NEO-START): Study protocol for a randomized controlled trial[J]. Trials, 2024, 25( 1): 490. DOI: 10.1186/s13063-024-08340-1. -

 本文二维码
本文二维码
计量
- 文章访问数: 2026
- HTML全文浏览量: 362
- PDF下载量: 106
- 被引次数: 0

