
 PDF下载 ( 1711 KB)
PDF下载 ( 1711 KB)

经口胆胰管镜联合内镜逆行胰胆管造影经十二指肠乳头胆囊息肉切除的疗效及安全性分析
DOI: 10.12449/JCH250318
Efficacy and safety of endoscopic retrograde cholangiopancreatography combined with oral cholangiopancreatography in the treatment of duodenal papilla cholecystectomy
-
摘要:
目的 探讨通过内镜逆行胰胆管造影(ERCP)联合经口胆胰管镜行经十二指肠乳头胆囊息肉切除治疗的可行性和安全性。 方法 回顾性分析2022年5月—2024年6月于吉林市人民医院消化内镜中心采用ERCP联合经口胆胰管镜行经十二指肠乳头胆囊息肉切除的8例胆总管结石合并胆囊息肉患者的临床资料,收集手术成功率和胆囊息肉清除技术成功率,胆囊管超选方式、整体手术时间、胆囊息肉切除时间、手术并发症等指标。 结果 手术成功率及胆囊息肉切除技术成功率为100%,其中3例患者通过导丝引导直视进入胆囊,5例通过经口胆胰管镜直接进入胆囊;整体手术时间为(51.88±12.34)min,胆囊息肉切除时间为(23.13±10.94)min;胆囊息肉病变直径为2~8 mm;病理结果为3例炎性息肉,1例腺瘤性息肉,4例胆固醇性息肉;术中及术后无并发症,术后随访2~27个月,胆囊无息肉复发。 结论 经口胆胰管镜在内镜下经十二指肠乳头胆囊息肉切除的临床应用,技术上相对安全可行。 -
关键词:
- 胆囊疾病 /
- 息肉 /
- 肝胰管壶腹 /
- 胰胆管造影术, 内窥镜逆行 /
- 经口胆胰管镜
Abstract:Objective To investigate the feasibility and safety of endoscopic retrograde cholangiopancreatography (ERCP) combined with oral cholangiopancreatography in the treatment of major duodenal papilla gallbladder polyps. Methods A retrospective analysis was performed for the clinical data of eight patients with choledocholithiasis and gallbladder polyps who underwent ERCP and combined with oral cholangiopancreatography for major duodenal papilla cholecystectomy in Center of Digestive Endoscopy, Jilin People’s Hospital, from May 2022 to June 2024, and related data were collected, including the success rate of surgery, the technical success rate of gallbladder polyp removal, the superselective method of cystic duct, the time of operation, the time of gallbladder polyp removal, and surgical complications. Results Both the success rate of surgery and the technical success rate of gallbladder polyp removal reached 100%, and of all eight patients, three patients used guide wire to enter the gallbladder under direct view, while five patients received oral cholangiopancreatography to directly enter the gallbladder. The time of operation was 51.88±12.34 minutes, and the time of gallbladder polyp removal was 23.13±10.94 minutes. The diameter of gallbladder polyp was 2 — 8 mm, and pathological examination showed inflammatory polyps in three patients, adenomatous polyps in one patient, and cholesterol polyps in four patients. There were no complications during or after surgery. The patients were followed up for 2 — 27 months after surgery, and no recurrence of gallbladder polyp was observed. Conclusion Oral cholangiopancreatography is technically safe and feasible in endoscopic major duodenal papilla cholecystectomy. -

注: a,超声内镜提示胆囊壁可见强回声光团,后不伴声影;b,经口胆胰管镜进入胆总管,直视观察胆囊管开口,在导丝引导下尝试进镜;c,胆囊颈部应用球囊扩张;d,扩张后的胆囊颈部,经口胆胰管镜直视通过;e,胆囊壁可见息肉样隆起;f,应用电圈套器尝试套取胆囊息肉;g,电圈套器套住息肉根部,电凝切除;h,切除后的创面电凝止血,电圈套器进行电凝止血,可以直视观察到该处创面电凝后发白的状态;i,胆道内留置塑料支架引流,乳头上方应用1枚钛夹夹闭(钛夹是为了预防穿孔和迟发性出血)。
图 1 经口胆胰管镜在内镜下经十二指肠乳头胆囊息肉切除的治疗过程
Figure 1. Endoscopic Major duodenal papilla cholecystectomy with oral cholangiopancreatography
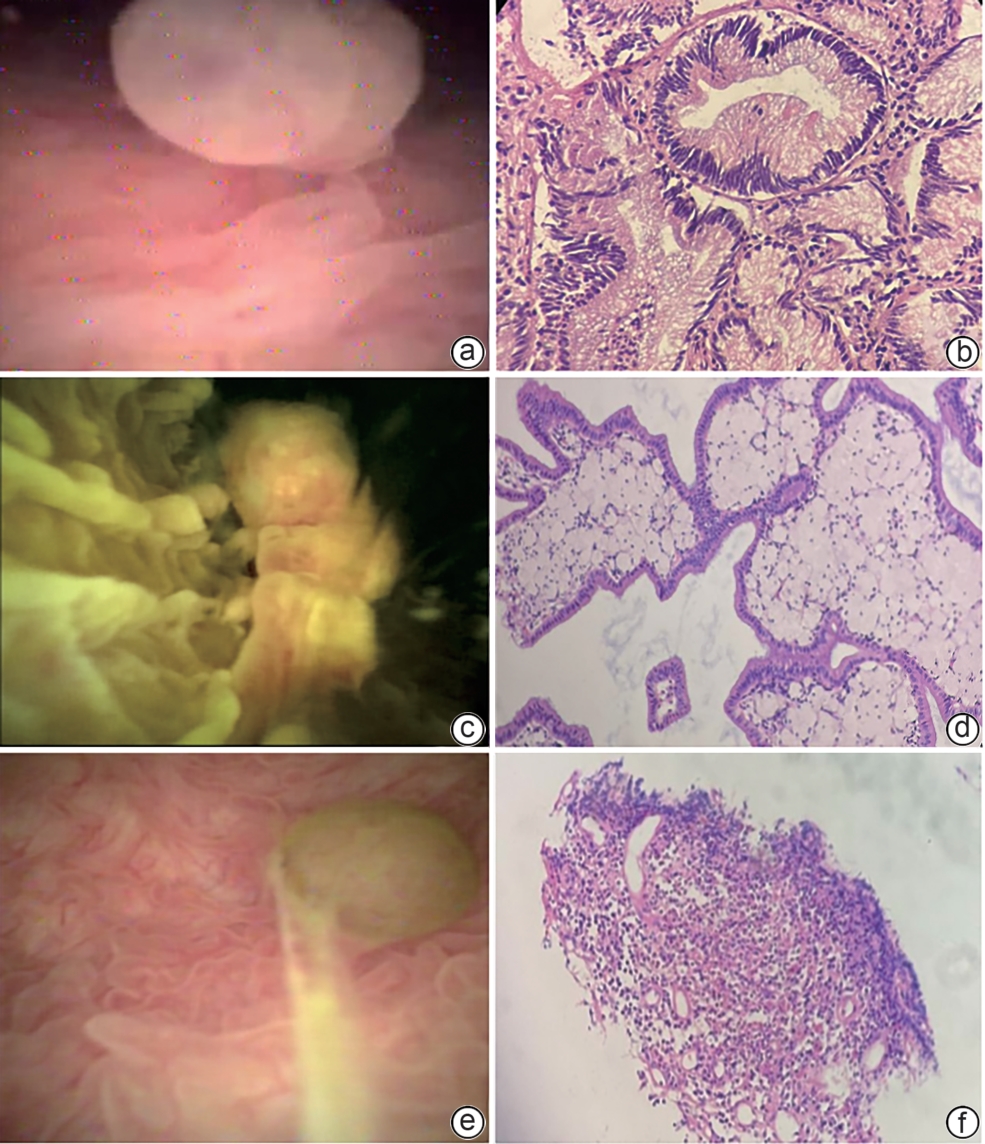
注: a,胆囊腺瘤性息肉;b,符合腺瘤性息肉(HE染色,×40);c,胆固醇性息肉;d,符合胆固醇性息肉,部分上皮细胞不典型增生(HE染色,×40);e,胆囊炎性息肉;f,可见慢性急性炎细胞浸润,部分血管内皮细胞增生(HE染色,×40)。
图 2 胆囊息肉内镜图像及病理
Figure 2. Endoscopic image and pathology of gallbladder polyp
表 1 8例患者的一般资料及手术情况
Table 1. General information and surgical findings of eight patients
序号 性别 年龄(岁) 病变大小(mm) 进入胆囊的方式 手术时间(min) 胆囊息肉切除时间(min) 切胆囊息肉器械 并发症 术后病理 随访时间(月) 1 女 76 2 导丝引导 47 17 热活检 无 炎性息肉 27 2 男 76 3.6 导丝引导 45 12 热活检 无 炎性息肉 24 3 女 53 6 导丝引导 65 42 电圈套 无 腺瘤性息肉 22 4 男 56 2 直视 27 10 热活检 无 炎性息肉 14 5 女 61 8 直视 53 35 电圈套 高淀粉酶血症 胆固醇性息肉 12 6 男 76 5 直视 57 17 热活检 无 胆固醇性息肉 6 7 男 39 4 直视+扩张 70 20 热活检 无 胆固醇性息肉 4 8 男 63 5 直视 51 32 电圈套 无 胆固醇性息肉 2 注:手术时间指十二指肠镜进镜至退镜时间。
 下载: 导出CSV
下载: 导出CSV
-
[1] LIU HR, SUN JN, XU LN, et al. Methods and prospects of gallbladder-preserving minimally invasive treatment for gallbladder polyps[J]. Chin J Dig Endosc, 2023, 40( 6): 501- 504. DOI: 10.3760/cma.j.cn321463-20220530-00184.刘浩然, 孙家宁, 徐林宁, 等. 胆囊息肉的保胆微创治疗方法与展望[J]. 中华消化内镜杂志, 2023, 40( 6): 501- 504. DOI: 10.3760/cma.j.cn321463-20220530-00184. [2] TAO LY, WANG HG, GUO QM, et al. Endoscopic retrograde cholangiopancreatography combined with peroral choledochoscopy in treatment of common bile duct stones with gallbladder neck stones and gallbladder polyps: A case report[J]. J Clin Hepatol, 2023, 39( 5): 1157- 1161. DOI: 10.3969/j.issn.1001-5256.2023.05.024.陶丽莹, 王宏光, 郭庆梅, 等. 内镜逆行胰胆管造影联合经口子母胆道镜治疗胆总管结石合并胆囊颈部结石及胆囊息肉1例报告[J]. 临床肝胆病杂志, 2023, 39( 5): 1157- 1161. DOI: 10.3969/j.issn.1001-5256.2023.05.024. [3] TAO LY, WANG HG, GUO QM. Single-operator cholangioscopy system for management of acute cholecystitis secondary to choledocholithiasis[J]. Endosc Int Open, 2023, 11( 12): E1138- E1142. DOI: 10.1055/a-2201-6871. [4] LEE J, CHOE S, PARK JW, et al. The risk of colorectal cancer after cholecystectomy or appendectomy: A population-based cohort study in Korea[J]. J Prev Med Public Health, 2018, 51( 6): 281- 288. DOI: 10.3961/jpmph.18.105. [5] HOUSSET C, CHRÉTIEN Y, DEBRAY D, et al. Functions of the gallbladder[J]. Compr Physiol, 2016, 6( 3): 1549- 1577. DOI: 10.1002/cphy.c150050. [6] LEE SR, KIM HO, SHIN JH. Reasonable cholecystectomy of gallbladder polyp-10 years of experience[J]. Asian J Surg, 2019, 42( 1): 332- 337. DOI: 10.1016/j.asjsur.2018.03.005. [7] WANG WH, LI P, WANG YJ, et al. Application of negative pressure suction to endoscopic transpapillary gallbladder preserving cholecystolithotomy[J]. Chin J Dig Endosc, 2024, 41( 7): 566- 569. DOI: 10.3760/cma.j.cn321463-20231206-00364.王文海, 李鹏, 王拥军, 等. 负压吸引法在内镜下经十二指肠乳头保胆取石术中的应用研究[J]. 中华消化内镜杂志, 2024, 41( 7): 566- 569. DOI: 10.3760/cma.j.cn321463-20231206-00364. [8] TAO LY, WANG HG, GUO X, et al. Efficacy of endoscopic retrograde cholangiopancreatography combined with SpyGlass system in treatment of acute cholecystitis secondary to choledocholithiasis[J]. J Clin Hepatol, 2022, 38( 8): 1854- 1858. DOI: 10.3969/j.issn.1001-5256.2022.08.025.陶丽莹, 王宏光, 郭享, 等. 内镜逆行胰胆管造影联合SpyGlass系统治疗胆总管结石继发急性胆囊炎的效果观察[J]. 临床肝胆病杂志, 2022, 38( 8): 1854- 1858. DOI: 10.3969/j.issn.1001-5256.2022.08.025. [9] FU MC, WNG LH, WANG FC, et al. Clinical analysis of 14 patients with gallbladder cancer misdiagnosed[J]. Clin Misdiagn Misther, 2023, 36( 9): 18- 21. DOI: 10.3969/j.issn.1002.3429.2023.09.005.付明晨, 王丽红, 王福朝, 等. 胆囊癌误漏诊14例临床分析[J]. 临床误诊误治, 2023, 36( 9): 18- 21. DOI: 10.3969/j.issn.1002.3429.2023.09.005. [10] TAO LY, WANG HG, GUO QM, et al. Gallbladder polyp removal by hot biopsy forceps under direct visualization using a novel peroral choledochoscope[J]. Gastrointest Endosc, 2023, 98( 6): 1030- 1031. DOI: 10.1016/j.gie.2023.06.065. [11] ZHANG WG, CHAI NL, FENG YJ, et al. Cholangioscopy-assisted endoscopic mucosal resection for gallbladder polyp and stone extraction for cholecystocholedocholithiasis[J]. Endoscopy, 2024, 56(S 01): E303- E304. DOI: 10.1055/a-2281-9743. [12] CAO J, DING XW, WU H, et al. Classification of the cystic duct patterns and endoscopic transpapillary cannulation of the gallbladder to prevent post-ERCP cholecystitis[J]. BMC Gastroenterol, 2019, 19( 1): 139. DOI: 10.1186/s12876-019-1053-6. -

 本文二维码
本文二维码
计量
- 文章访问数: 1110
- HTML全文浏览量: 437
- PDF下载量: 111
- 被引次数: 0

