
 PDF下载 ( 1318 KB)
PDF下载 ( 1318 KB)

失代偿期肝硬化合并急性肾损伤患者入院后30天内死亡的危险因素及列线图预测模型构建
DOI: 10.12449/JCH241115
Risk factors for death within 30 days after admission in patients with decompensated liver cirrhosis and acute kidney injury and construction of a nomogram model
-
摘要:
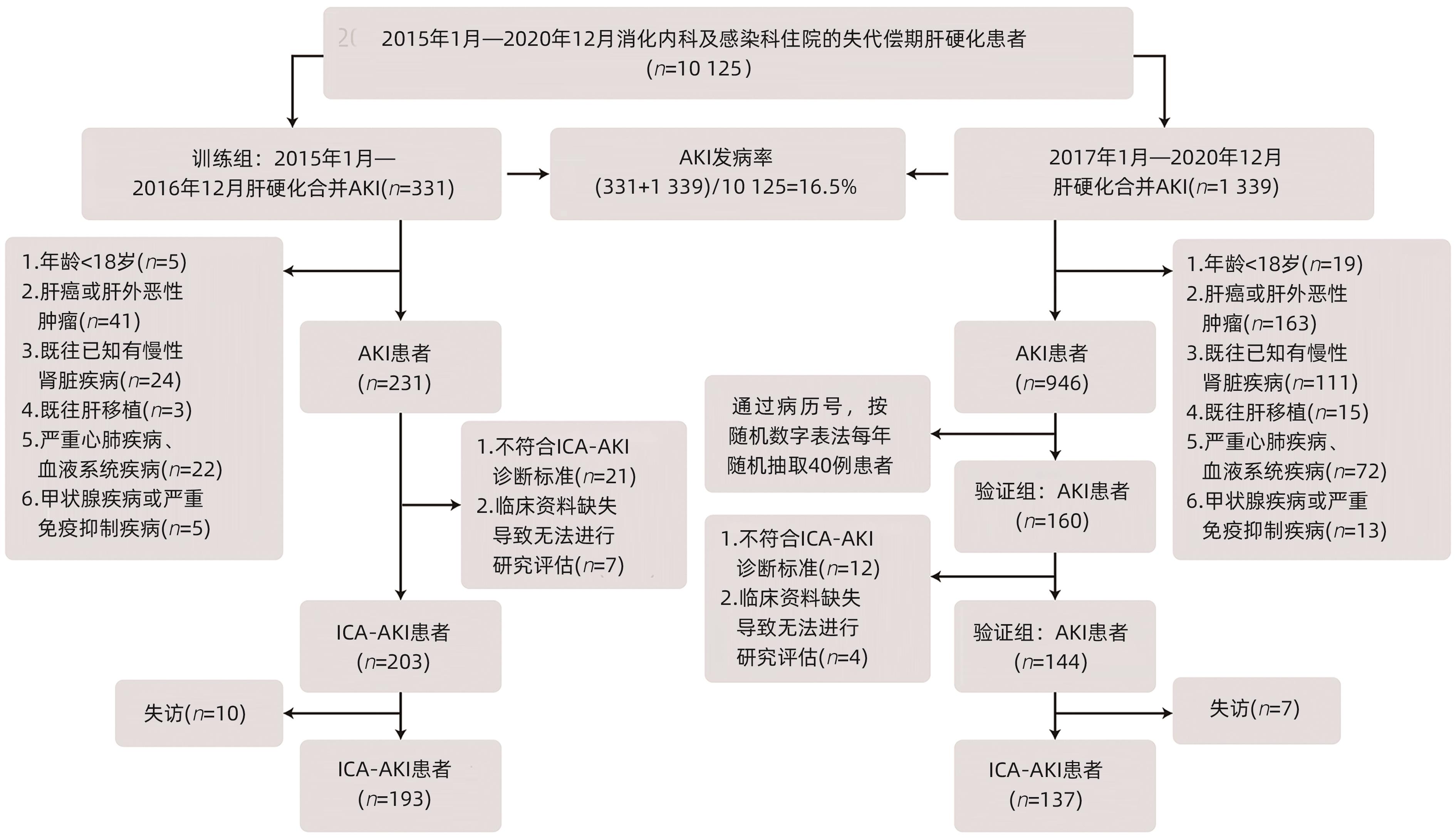
目的 分析失代偿期肝硬化合并急性肾损伤(AKI)的患者入院后30天内死亡预测因素,同时建立并验证列线图预测模型。 方法 通过南昌大学第一附属医院联众病案管理系统,筛查2015年1月—2020年12月在消化内科和感染科住院的失代偿期肝硬化患者,纳入符合2015年国际腹水俱乐部AKI诊断标准的患者330例,其中训练组193例,验证组137例,通过Cox回归分析影响其死亡的预测因素,建立并验证入院后30天内的死亡风险列线图预测模型。符合正态分布的计量资料2组间比较采用成组t检验,多组间比较采用单因素方差分析,进一步两两比较采用LSD-t检验;不符合正态分布的计量资料2组间比较采用Mann-Whitney U检验,多组间比较采用Kruskal-Wallis H检验。计数资料组间比较采用χ2检验或Fisher精确检验。 结果 失代偿期肝硬化患者中AKI患病率为16.5%。纳入研究的330例患者平均年龄(53.6±12.4)岁,男性占79.1%,入院后30天病死率为50.0%,训练组和验证组病死率分别为46.6%和54.7%。入院时存在慢加急性肝衰竭(ACLF)是AKI 1期进展的独立危险因素(OR=2.571,95%CI: 1.143~5.780, P=0.022)。基于入院时白细胞计数、国际标准化比值、是否有肝性脑病及AKI分期所建立的列线图能较好预测入院后30天死亡风险,训练组和验证组C指数分别为0.680和0.683,且不劣于CTP评分和MELD评分。 结论 ACLF是AKI 1期进展的独立危险因素,建立的列线图预测模型可有效预测患者入院后30天内死亡风险,对于早期识别和管理失代偿期肝硬化合并AKI患者有重要指导意义。 Abstract:Objective To investigate the predictive factors for death within 30 days after admission in patients with decompensated liver cirrhosis and acute kidney injury (AKI), and to establish and validate a nomogram prediction model. Methods The Joint Medical Record Management System of The First Affiliated Hospital of Nanchang University was used to obtain the patients with decompensated liver cirrhosis who were hospitalized in Department of Gastroenterology and Department of Infectious Diseases from January 2015 to December 2020, among whom 330 patients who met the 2015 International Club of Ascites diagnostic criteria for AKI were enrolled and divided into training group with 193 patients and validation group with 137 patients. A Cox regression analysis was used to investigate the predictive factors for death, and then a nomogram prediction model for the risk of death within 30 days after admission was established and validated. The independent-samples t-test was used for comparison of normally distributed continuous data between two groups, and a one-way analysis of variance was used for comparison between multiple groups, while the least significant difference t-test was used for further comparison between two groups; The Mann-Whitney U test was used for comparison of non-normally distributed continuous data between two groups, while the Kruskal-Wallis H test was used for comparison between multiple groups. The chi-square test or the Fisher’s exact test was used for comparison of categorical data between groups. Results The prevalence rate of AKI was 16.5% in patients with decompensated liver cirrhosis. The 330 patients included in the study had a mean age of 53.6±12.4 years, and male patients accounted for 79.1%. The mortality rate was 50.0% within 30 days after admission, with a mortality rate of 46.6% in the training group and 54.7% in the validation group. The presence of acute-on-chronic liver failure (ACLF) on admission was an independent risk factor for the progression of AKI into stage 1 (odds ratio=2.571, 95% confidence interval: 1.143 — 5.780, P=0.022). The nomogram based on white blood cell count, international normalized ratio, presence or absence of hepatic encephalopathy, and AKI stage on admission could well predict the risk of death with 30 days after admission, with a C-index of 0.680 in the training group and 0.683 in the validation group, and it was not inferior to CTP score and MELD score. Conclusion ACLF is an independent risk factor for the progression of AKI into stage 1. The nomogram prediction model established in this study can effectively predict the risk of death within 30 days after admission and thus has important guiding significance for the early identification and management of patients with decompensated liver cirrhosis and AKI. -
Key words:
- Liver Cirrhosis /
- Acute Kidney Injury /
- Nomograms
-
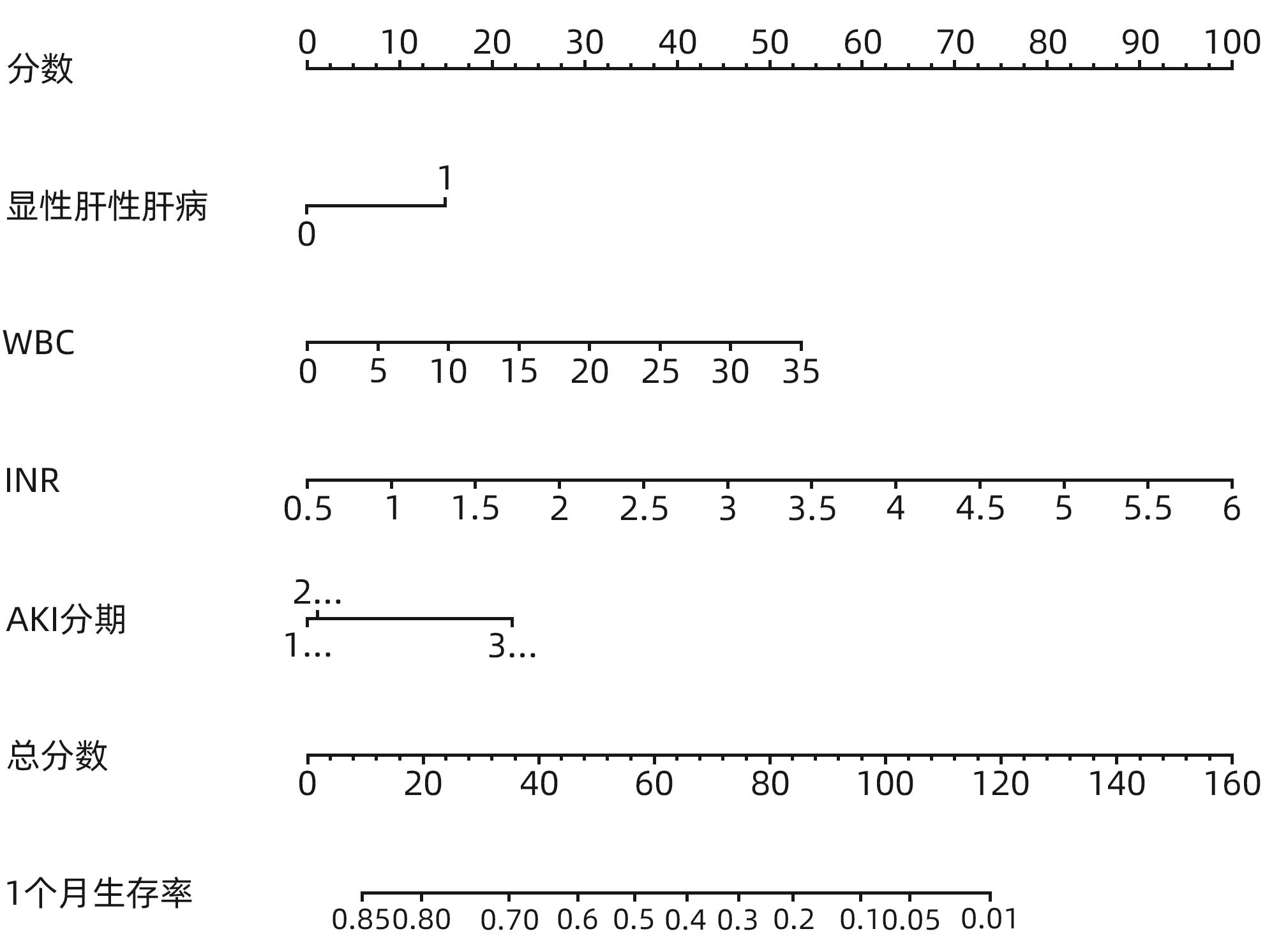
图 2 失代偿期肝硬化并发AKI患者入院后30天死亡预测列线图模型
Figure 2. A 30-day mortality prediction model for patients with decompensated cirrhosis complicated with AKI after admission
表 1 失代偿期肝硬化合并AKI不同分期患者入院后的基线特征
Table 1. Baseline characteristics of patients with decompensated cirrhosis and AKI at different stages after admission
项目 总计(n=330) AKI 1期(n=198) AKI 2期(n=64) AKI 3期(n=68) 统计值 P值 年龄(岁) 53.6±12.4 54.2±12.3 52.7±11.6 52.6±13.6 F=0.625 0.536 男性[例(%)] 261(79.1) 158(79.8) 51(79.7) 52(76.5) 0.837 糖尿病[例(%)] 46(13.9) 30(15.2) 9(14.1) 7(10.3) 0.608 肝硬化病因[例(%)] 乙型肝炎 262(79.4) 159(80.3) 51(79.7) 52(76.5) 0.795 酒精性 48(14.5) 27(13.6) 9(14.1) 12(17.6) 0.715 自身免疫性 6(1.8) 2(1.0) 2(3.1) 2(2.9) 0.403 血吸虫性 13(3.9) 8(4.0) 3(4.7) 2(2.9) 0.870 其他 29(8.8) 19(9.6) 4(6.3) 6(8.8) 0.713 MAP(mmHg) 87.5±14.3 86.8±14.7 88.3±13.0 88.7±14.2 F=0.583 0.559 心率(次/min) 88.5±15.8 87.3±16.0 91±15.6 89.8±15.0 F=1.630 0.198 WBC(×109/L) 6.6(4.7~9.8) 6.7(4.8~9.6) 6.7(4.9~9.7) 6.3(4.3~9.9) 0.837 Hb(g/L) 106.2±26.7 106.0±28.0 108.2±23.8 104.4±25.6 F=0.338 0.713 PLT(×109/L) 79(50~123) 79(50~120) 76(50~116) 85(50~148) 0.439 Alb(g/L) 29.1±5.1 29.3±5.1 29.6±5.4 28.0±4.7 F=2.014 0.135 ALT(U/L) 89.0(32.0~271.0) 89.0(31.0~238.8) 93.4(43.3~342.8) 78.9(27.3~310.5) 0.568 AST(U/L) 130.5(64.8~291.3) 131.5(58.8~263.0) 126.0(89.5~361.8) 132.5(65.5~339.3) 0.539 TBil(μmol/L) 248.7±188.1 242.4±188.4 293.0±187.0 225.6±184.2 F=2.418 0.091 Na+(mmol/L) 134.4(130.0~138.0) 134.5(130.0~137.9) 134.2(129.6~138.0) 134.0(130.0~138.4) 0.920 INR 1.9(1.4~2.4) 1.9(1.4~2.5) 1.9(1.5~2.3) 1.7(1.3~2.2) 0.272 SCr(mg/dL) 1.3±0.9 1.2±0.6 0.9±0.5 1.8±1.5 F=19.718 <0.001 MELD评分(分) 22.6±8.9 22.6±8.5 21.8±7.3 23.5±11.2 F=0.616 0.541 Child-Pugh评分(分) 11.1±2.0 10.8±2.1 11.4±2.01) 11.6±1.81) F=5.469 0.005 并发症[例(%)] 腹水 311(94.2) 186(93.9) 58(90.6) 67(98.5) 0.144 EGVB 35(10.6) 24(12.1) 5(7.8) 6(8.8) 0.540 SBP 119(36.1) 72(36.4) 24(37.5) 23(33.8) 0.899 显性肝性脑病 96(29.1) 42(21.2) 27(42.2)1) 27(39.7)2) 0.001 ACLF 205(62.1) 118(59.6) 49(76.6)1) 38(55.9)2) 0.026 注:MAP,平均动脉压;EGVB,食管胃静脉曲张破裂出血;SBP,自发性细菌性腹膜炎。与AKI 1期比较,1) P<0.05;与AKI 2期比较,2) P<0.05。
 下载: 导出CSV
下载: 导出CSV
表 2 失代偿期肝硬化合并AKI 1期患者住院期间好转或进展基线资料
Table 2. Baseline data on improvement or progression during hospitalization in patients with decompensated cirrhosis and AKI stage 1
项目 好转情况 进展情况 好转(n=75) 未好转(n=123) P值 进展(n=38) 未进展(n=160) P值 年龄(岁) 53.2±12.0 54.9±12.5 0.356 53.4±11.4 54.4±12.6 0.661 男性[例(%)] 57(76.0) 101(82.1) 0.299 32(84.2) 126(78.8) 0.451 糖尿病[例(%)] 7(9.3) 23(18.7) 0.075 8(21.1) 22(13.8) 0.259 肝硬化病因[例(%)] 乙型肝炎 61(81.3) 98(79.7) 0.776 33(86.8) 126(78.8) 0.260 酒精性 10(13.3) 17(13.8) 0.923 4(10.5) 23(14.4) 0.534 MAP(mmHg) 86.2±15.3 87.1±14.3 0.685 87.7±13.3 86.5±15.1 0.655 心率(次/min) 87.9±17.0 86.9±15.5 0.459 90.2±16.0 86.6±16.0 0.333 WBC(×109/L) 7.5±4.1 7.9±4.6 0.576 7.9±3.4 7.7±4.6 0.216 Hb(g/L) 104.4±29.5 107.4±27.2 0.468 109.4±20.4 105.5±29.6 0.338 PLT(×109/L) 84.2±44.0 91.0±62.6 0.361 98.6±53.7 86.8±56.9 0.317 Alb(g/L) 28.6±6.1 29.7±4.3 0.145 30.2±3.8 29.1±5.3 0.154 ALT(U/L) 68(31~237) 110(33~245) 0.285 148(69~393) 74(30~218) 0.053 AST(U/L) 119(62~232) 146(53~266) 0.583 211(92~304) 119(57~262) 0.032 TBil(μmol/L) 230.6±181.6 249.6±192.8 0.495 315.2±166.9 225.1±115.6 0.008 Na+(mmol/L) 133.7±6.2 134.1±5.3 0.491 134.2±4.7 133.9±5.9 0.690 INR 1.9(1.4~2.4) 1.8(1.4~2.5) 0.860 2.1(1.6~2.8) 1.8(1.4~2.4) 0.040 基线SCr>1.5 mg/L[例(%)] 17(22.7) 32(26) 0.596 5(13.2) 44(27.5) 0.066 Child-Pugh C级[例(%)] 58(77.3) 90(73.2) 0.513 31(81.6) 117(73.1) 0.281 Child-Pugh评分(分) 10.9±2.0 10.7±2.1 0.420 11.0±1.9 10.7±2.1 0.497 MELD评分(分) 22.7±7.7 22.5±9.0 0.870 23.9±8.5 22.2±8.5 0.204 并发症[例(%)] 腹水 72(96.0) 114(92.7) 0.343 35(92.1) 151(94.4) 0.598 EGVB 9(12.0) 15(12.2) 0.967 4(10.5) 20(12.5) 0.738 SBP 25(33.3) 47(38.2) 0.489 16(42.1) 56(35.0) 0.413 显性肝性脑病 17(22.7) 25(20.3) 0.696 8(21.1) 34(21.3) 0.979 ACLF 44(58.7) 74(60.2) 0.835 29(76.3) 89(55.6) 0.019
下载: 导出CSV
表 3 训练组和验证组基线资料特征
Table 3. Baseline data characteristics of training group and validation group
项目 训练组(n=193) 验证组(n=137) 死亡组(n=90) 生存组(n=103) P值 死亡组(n=75) 生存组(n=62) P值 年龄(岁) 53.9±13.1 52.7±12.9 0.541 53.8±10.0 54.4±13.4 0.761 男性[例(%)] 73(81.1) 75(72.8) 0.174 63(84.0) 59(80.6) 0.607 糖尿病[例(%)] 9(10.0) 10(9.7) 0.946 14(18.7) 13(21.0) 0.736 MAP(mmHg) 85.2±13.0 88.9±14.8 0.067 89.4±13.8 85.9±15.4 0.150 心率(次/min) 89.7±14.3 86.8±14.5 0.011 92.0±16.7 85.4±17.9 0.025 WBC(×109/L) 7.9(5.3~11.2) 6.1(3.8~8.3) 0.003 7.5(5.2~10.0) 6.6(4.5~9.0) 0.219 Hb(g/L) 104.2±27.3 106.4±25.9 0.568 112.1±26.0 101.9±27.5 0.027 PLT(×109/L) 66(47~122) 79(48~119) 0.522 91(62~136) 76(51~117) 0.199 Alb(g/L) 28.0±4.7 29.4±5.6 0.143 29.4±4.3 29.7±5.4 0.657 ALT(U/L) 105(52~287) 89(28~265) 0.121 187(54~473) 34(20~127) <0.001 AST(U/L) 160(90~368) 122(62~260) 0.046 166(99~471) 66(37~159) <0.001 TBil(μmol/L) 262.3±182.2 245.5±191.0 0.536 334.0(151.2~417.9) 87.6(19.5~298.2) <0.001 Na+(mmol/L) 131.7±5.8 133.7±5.9 0.039 134.2±5.4 136.4±4.9 0.014 INR 1.9(1.5~2.8) 1.7(1.4~2.2) <0.001 2.1(1.7~2.6) 1.5(1.3~2.0) <0.001 基线SCr>1.5 mg/L[例(%)] 29(32.2) 27(26.2) 0.359 12(16.0) 11(17.7) 0.786 Child-Pugh评分(分) 12.1±1.7 11.2±1.8 <0.001 10.9±1.7 9.5±2.2 <0.001 MELD评分(分) 24.9±9.5 21.9±7.7 0.015 24.6±8.7 18.0±8.5 <0.001 并发症[例(%)] 腹水 86(95.6) 97(94.2) 0.666 70(93.3) 58(93.5) 0.960 EGVB 6(6.7) 5(4.9) 0.588 12(16.0) 12(19.4) 0.607 SBP 25(27.8) 23(22.3) 0.382 48(64.0) 23(37.1) 0.002 显性肝性脑病 46(51.1) 32(31.1) 0.005 15(20.0) 3(4.8) 0.009 ACLF 61(67.8) 62(60.2) 0.274 59(78.7) 23(37.1) <0.001 AKI分期[例(%)] 1期 39(43.3) 60(58.3) 0.039 47(62.7) 52(83.9) 0.006 2期 19(21.1) 19(18.4) 0.642 19(25.3) 7(11.3) 0.037 3期 32(35.6) 24(23.3) 0.061 9(12.0) 3(4.8) 0.140
下载: 导出CSV
表 4 训练组和验证组不同预测模型的预测准确性比较
Table 4. Comparison of prediction accuracy of different prediction models between the training group and the verification group
项目 Cut-off 敏感度(%) 特异度(%) 约登指数 AUC 95%CI 训练组 列线图 0.358 75.56 60.19 0.358 0.702 0.632~0.765 Child-Pugh评分 0.243 46.67 77.67 0.243 0.650 0.578~0.717 MELD评分 0.252 55.33 71.84 0.252 0.6161) 0.543~0.685 验证组 列线图 0.439 90.67 53.23 0.439 0.767 0.687~0.835 Child-Pugh评分 0.294 82.67 46.77 0.294 0.6741) 0.589~0.752 MELD评分 0.377 58.67 79.03 0.377 0.704 0.620~0.779 注:与列线图比较,P<0.05
下载: 导出CSV
-
[1] European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis[J]. J Hepatol, 2018, 69( 2): 406- 460. DOI: 10.1016/j.jhep.2018.03.024. [2] GUPTA K, BHURWAL A, LAW C, et al. Acute kidney injury and hepatorenal syndrome in cirrhosis[J]. World J Gastroenterol, 2021, 27( 26): 3984- 4003. DOI: 10.3748/wjg.v27.i26.3984. [3] NADIM MK, GARCIA-TSAO G. Acute kidney injury in patients with cirrhosis[J]. N Engl J Med, 2023, 388( 8): 733- 745. DOI: 10.1056/NEJMra2215289. [4] PATIDAR KR, BELCHER JM, REGNER KR, et al. Incidence and outcomes of acute kidney injury including hepatorenal syndrome in hospitalized patients with cirrhosis in the US[J]. J Hepatol, 2023, 79( 6): 1408- 1417. DOI: 10.1016/j.jhep.2023.07.010. [5] TARIQ R, HADI Y, CHAHAL K, et al. Incidence, mortality and predictors of acute kidney injury in patients with cirrhosis: A systematic review and meta-analysis[J]. J Clin Transl Hepatol, 2020, 8( 2): 135- 142. DOI: 10.14218/JCTH.2019.00060. [6] BELCHER JM, GARCIA-TSAO G, SANYAL AJ, et al. Association of AKI with mortality and complications in hospitalized patients with cirrhosis[J]. Hepatology, 2013, 57( 2): 753- 762. DOI: 10.1002/hep.25735. [7] WONG F, BOYER TD, SANYAL AJ, et al. Reduction in acute kidney injury stage predicts survival in patients with type-1 hepatorenal syndrome[J]. Nephrol Dial Transplant, 2020, 35( 9): 1554- 1561. DOI: 10.1093/ndt/gfz048. [8] ANGELI P, GINÈS P, WONG F, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: Revised consensus recommendations of the International Club of Ascites[J]. J Hepatol, 2015, 62( 4): 968- 974. DOI: 10.1016/j.jhep.2014.12.029. [9] SARIN SK, KUMAR A, ANGUS PW, et al. Diagnosis and management of acute variceal bleeding: Asian Pacific Association for Study of the Liver recommendations[J]. Hepatol Int, 2011, 5( 2): 607- 624. DOI: 10.1007/s12072-010-9236-9. [10] European Association for the Study of the Liver. EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis[J]. J Hepatol, 2010, 53( 3): 397- 417. DOI: 10.1016/j.jhep.2010.05.004. [11] FERENCI P, LOCKWOOD A, MULLEN K, et al. Hepatic encephalopathy: Definition, nomenclature, diagnosis, and quantification: Final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998[J]. Hepatology, 2002, 35( 3): 716- 721. DOI: 10.1053/jhep.2002.31250. [12] ROSE CF, AMODIO P, BAJAJ JS, et al. Hepatic encephalopathy: Novel insights into classification, pathophysiology and therapy[J]. J Hepatol, 2020, 73( 6): 1526- 1547. DOI: 10.1016/j.jhep.2020.07.013. [13] SARIN SK, CHOUDHURY A, SHARMA MK, et al. Acute-on-chronic liver failure: Consensus recommendations of the Asian Pacific association for the study of the liver(APASL): An update[J]. Hepatol Int, 2019, 13( 4): 353- 390. DOI: 10.1007/s12072-019-09946-3. [14] PUGH RN, MURRAY-LYON IM, DAWSON JL, et al. Transection of the oesophagus for bleeding oesophageal varices[J]. Br J Surg, 1973, 60( 8): 646- 649. DOI: 10.1002/bjs.1800600817. [15] BOTTA F, GIANNINI E, ROMAGNOLI P, et al. MELD scoring system is useful for predicting prognosis in patients with liver cirrhosis and is correlated with residual liver function: A European study[J]. Gut, 2003, 52( 1): 134- 139. DOI: 10.1136/gut.52.1.134. [16] WIESNER R, EDWARDS E, FREEMAN R, et al. Model for end-stage liver disease(MELD) and allocation of donor livers[J]. Gastroenterology, 2003, 124( 1): 91- 96. DOI: 10.1053/gast.2003.50016. [17] DESAI AP, KNAPP SM, ORMAN ES, et al. Changing epidemiology and outcomes of acute kidney injury in hospitalized patients with cirrhosis-a US population-based study[J]. J Hepatol, 2020, 73( 5): 1092- 1099. DOI: 10.1016/j.jhep.2020.04.043. [18] ARORA MS, KAUSHIK R, AHMAD S, et al. Profile of acute kidney injury in patients with decompensated cirrhosis at a tertiary-care center in uttarakhand, India[J]. Dig Dis, 2020, 38( 4): 335- 343. DOI: 10.1159/000504836. [19] MICHELENA J, ALTAMIRANO J, ABRALDES JG, et al. Systemic inflammatory response and serum lipopolysaccharide levels predict multiple organ failure and death in alcoholic hepatitis[J]. Hepatology, 2015, 62( 3): 762- 772. DOI: 10.1002/hep.27779. [20] TANDON P, JAMES MT, ABRALDES JG, et al. Relevance of new definitions to incidence and prognosis of acute kidney injury in hospitalized patients with cirrhosis: A retrospective population-based cohort study[J]. PLoS One, 2016, 11( 8): e0160394. DOI: 10.1371/journal.pone.0160394. [21] WAN YP, WANG AJ, ZHANG W, et al. Development and validation of a nomogram for predicting overall survival in cirrhotic patients with acute kidney injury[J]. World J Gastroenterol, 2022, 28( 30): 4133- 4151. DOI: 10.3748/wjg.v28.i30.4133. [22] SCHACHER FC, MATTOS AA, MULAZZANI CM, et al. Impact of acute kidney injury staging on prognosis of patients with cirrhosis[J]. Arq Gastroenterol, 2020, 57( 3): 244- 248. DOI: 10.1590/S0004-2803.202000000-46. [23] DUAH A, DUAH F, AMPOFO-BOOBI D, et al. Acute kidney injury in patients with liver cirrhosis: Prevalence, predictors, and In-hospital mortality at a district hospital in Ghana[J]. Biomed Res Int, 2022, 2022: 4589767. DOI: 10.1155/2022/4589767. [24] PATIDAR KR, CULLARO G, NAVED MA, et al. Prognostic significance of acute kidney injury stage 1B in hospitalized patients with cirrhosis: A US nationwide study[J]. Liver Transpl, 2024, 30( 3): 244- 253. DOI: 10.1097/LVT.0000000000000241. [25] PIANO S, ROSI S, MARESIO G, et al. Evaluation of the Acute Kidney Injury Network criteria in hospitalized patients with cirrhosis and ascites[J]. J Hepatol, 2013, 59( 3): 482- 489. DOI: 10.1016/j.jhep.2013.03.039. [26] MAIWALL R, SARIN SK, KUMAR S, et al. Development of predisposition, injury, response, organ failure model for predicting acute kidney injury in acute on chronic liver failure[J]. Liver Int, 2017, 37( 10): 1497- 1507. DOI: 10.1111/liv.13443. [27] GOMES CGO, De ANDRADE MVM, RESENDE GUEDES L, et al. Clinical aspects and prognosis evaluation of cirrhotic patients hospitalized with acute kidney injury[J]. Can J Gastroenterol Hepatol, 2019, 2019: 6567850. DOI: 10.1155/2019/6567850. [28] SCOTT RA, AUSTIN AS, KOLHE NV, et al. Acute kidney injury is independently associated with death in patients with cirrhosis[J]. Frontline Gastroenterol, 2013, 4( 3): 191- 197. DOI: 10.1136/flgastro-2012-100291. [29] MOGA L, ROBIC MA, BLASCO-PERRIN H, et al. Acute kidney injury in patients with cirrhosis: Prospective longitudinal study in 405 patients[J]. Clin Res Hepatol Gastroenterol, 2022, 46( 4): 101822. DOI: 10.1016/j.clinre.2021.101822. [30] ALESSANDRIA C, OZDOGAN O, GUEVARA M, et al. MELD score and clinical type predict prognosis in hepatorenal syndrome: Relevance to liver transplantation[J]. Hepatology, 2005, 41( 6): 1282- 1289. DOI: 10.1002/hep.20687. [31] BIGGINS SW, ANGELI P, GARCIA-TSAO G, et al. Diagnosis, evaluation, and management of ascites, spontaneous bacterial peritonitis and hepatorenal syndrome: 2021 practice guidance by the American association for the study of liver diseases[J]. Hepatology, 2021, 74( 2): 1014- 1048. DOI: 10.1002/hep.31884. [32] FLAMM SL, WONG F, AHN J, et al. AGA clinical practice update on the evaluation and management of acute kidney injury in patients with cirrhosis: Expert review[J]. Clin Gastroenterol Hepatol, 2022, 20( 12): 2707- 2716. DOI: 10.1016/j.cgh.2022.08.033. -

 本文二维码
本文二维码
计量
- 文章访问数: 973
- HTML全文浏览量: 438
- PDF下载量: 133
- 被引次数: 0

