
 PDF下载 ( 952 KB)
PDF下载 ( 952 KB)

睡眠障碍与非酒精性脂肪性肝病不同阶段的关联性分析
DOI: 10.12449/JCH240712
Association between sleep disorders and different stages of nonalcoholic fatty liver disease
-
摘要:
目的 探索睡眠障碍与非酒精性脂肪性肝病(NAFLD)发生发展的关系。 方法 选取2022年6月—2023年6月北京友谊医院健康体检队列和脂肪肝门诊队列共1 868例参与者。收集所有受试者年龄、性别、文化程度和慢性病史等一般资料及生化等实验室指标,受试者独立完成匹兹堡睡眠质量指数(PSQI)量表测评。根据诊断标准将受试者分为非脂肪肝组(non-NAFLD组)(n=1 122)和脂肪肝组(NAFLD组)(n=746),其中NAFLD组按照发展阶段分为单纯脂肪肝组(SFL组)(n=624)和脂肪性肝炎组(NASH组)(n=122)。计量资料3组间比较采用单因素方差分析或Kruskal-Wallis H检验。计数资料3组间比较采用χ2检验。采用二元Logistic回归分析睡眠因素与NAFLD的关联性,采用多分类Logistic回归分析睡眠因素与NAFLD不同阶段的关联性,并构建两个多因素模型校正可能的混杂因素,包括年龄性别校正模型和多因素校正模型,多因素校正模型校正了年龄、性别、文化程度、吸烟、糖尿病、高血压、BMI、TG、HDL-C因素。 结果 non-NAFLD、SFL和NASH组在年龄、性别、BMI、文化程度、吸烟、糖尿病、高血压、ALT、TG、HDL-C的比较,差异均有统计学意义(P值均<0.05)。3组在PSQI量表总评分分级以及7个睡眠成分的0~3分分级中的人数比例比较,差异均有统计学意义(P值均<0.05)。在多因素校正模型中,尚无睡眠障碍成分与SFL患病相关,而入睡时间长(OR=4.04,95%CI:2.33~7.03,P<0.001)、睡眠时间短(OR=3.53,95%CI:1.83~6.82,P<0.001)和睡眠紊乱严重(OR=2.96,95%CI:1.48~5.93,P=0.002)与NASH的患病风险密切相关。 结论 睡眠整体状况和其包含的睡眠障碍成分与SFL的患病并无明显关联,而入睡时间长、睡眠时间短和睡眠紊乱可增加NASH的患病风险,需要加以关注。 Abstract:Objective To investigate the association of sleep disorders with the development and progression of nonalcoholic fatty liver disease (NAFLD). Methods A total of 1 868 participants from the health examination cohort and fatty liver cohort of Beijing Friendship Hospital from June 2022 to June 2023 were enrolled as subjects. Related data were collected from all subjects, including age, sex, education level, chronic medical history, and biochemical parameters, and all subjects completed Pittsburgh Sleep Quality Index (PSQI) scale independently. According to the diagnostic criteria, the subjects were divided into non-NAFLD group with 1 122 subjects and NAFLD group with 746 subjects, and according to the stage of progression, the patients in the NAFLD group were further divided into simple fatty liver group (SFL group with 624 subjects) and nonalcoholic steatohepatitis (NASH) group with 122 subjects. A one-way analysis of variance or the Kruskal-Wallis H test was used for comparison of continuous data between three groups. The chi-square test was used for comparison of categorical data between the three groups. The binary Logistic regression analysis was used to investigate the association between sleep factors and NAFLD, and the multinomial Logistic regression analysis was used to investigate the association between sleep factors and the different stages of NAFLD; two multivariate models were constructed for adjustment of potential confounding factors, i.e., an age-sex adjustment model and a multivariate adjustment model, and the multivariate adjustment model adjusted the factors of age, sex, education level, smoking, diabetes, hypertension, body mass index (BMI), triglyceride (TG), and high-density lipoprotein cholesterol (HDL-C). Results There were significant differences in age, sex, BMI, education level, smoking, diabetes, hypertension, alanine aminotransferase, TG, and HDL-C between the non-NAFLD, SFL, and NASH groups (all P<0.05). There were also significant differences between the three groups in the total score of PSQI scale and the proportion of subjects with a score of 0 — 3 points for the 7 sleep components (all P<0.05). The multivariate adjustment model showed no significant association between sleep disorders and SFL, while long sleep latency (odds ratio [OR]=4.04, 95% confidence interval [CI]: 2.33 — 7.03, P<0.001), short sleep duration (OR=3.53, 95%CI: 1.83 — 6.82, P<0.001), and severe sleep disorders (OR=2.96, 95%CI: 1.48 — 5.93, P=0.002) were closely associated with the risk of NASH. Conclusion Overall sleep condition and its components of sleep disorders are not significantly associated with the simple fatty liver; however, long sleep latency, short sleep duration, and severe sleep disorders can increase the risk of NASH, which should be taken seriously in clinical practice. -
Key words:
- Non-alcoholic Fatty Liver Disease /
- Sleep Disorders /
- Regression Analysis
-
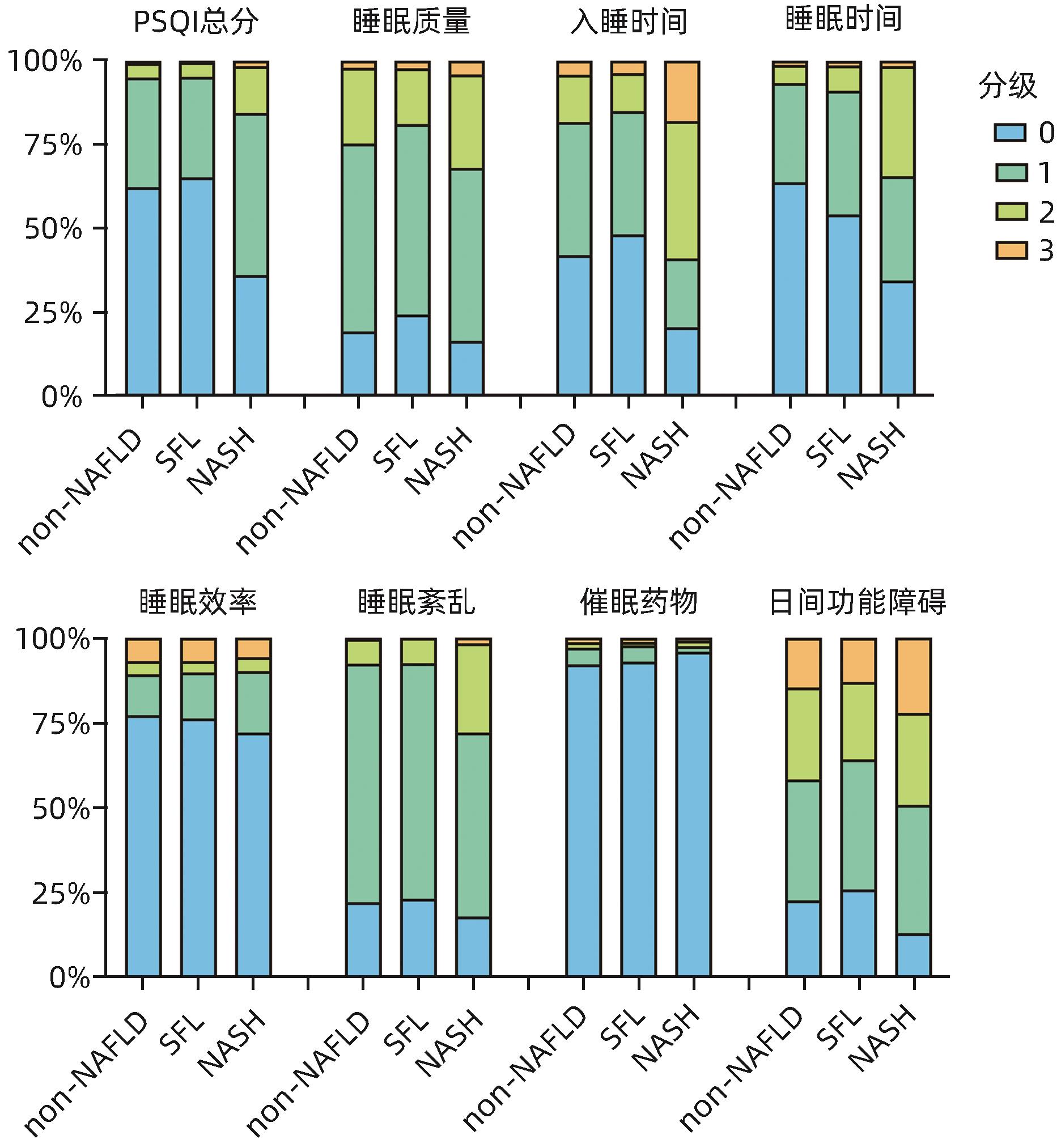
图 1 3组PSQI量表总分及因子分比较
Figure 1. The comparison of the PSQI total score and each factor scores in three groups
表 1 3组间一般资料比较
Table 1. The comparison of general information in three groups
指标 non-NAFLD组(n=1 122) SFL组(n=624) NASH组(n=122) 统计值 P值 年龄(岁) 39.58±7.71 42.78±7.74 38.94±10.04 F=35.88 <0.001 男[例(%)] 550(49.02) 506(81.09) 82(67.21) χ2=175.40 <0.001 本科以上学历[例(%)] 721(64.26) 335(53.69) 35(28.69) χ2=65.90 <0.001 吸烟[例(%)] 87(7.75) 131(20.99) 25(20.49) χ2=68.57 <0.001 糖尿病[例(%)] 12(1.07) 58(9.29) 22(18.03) χ2=105.83 <0.001 高血压[例(%)] 72(6.42) 147(23.56) 36(29.51) χ2=127.79 <0.001 BMI(kg/m2) 22.88±2.74 27.11±3.19 31.94±10.04 F=639.40 <0.001 ALT(U/L) 16.00(12.00~22.00) 27.00(19.00~39.00) 94.00(83.00~115.00) χ2=649.38 <0.001 TG(mmol/L) 0.89(0.69~1.22) 1.65(1.18~2.36) 1.84(1.34~2.30) χ2=552.89 <0.001 HDL-C(mmol/L) 1.41(1.21~1.63) 1.13(1.01~1.29) 1.15(0.97~1.29) χ2=383.33 0.002  下载: 导出CSV
下载: 导出CSV
表 2 睡眠情况与NAFLD的关联分析
Table 2. The association between sleep condition and NAFLD
变量 患病率 单因素模型 年龄性别校正模型 多因素校正模型 OR(95%CI) P值 OR(95%CI) P值 OR(95%CI) P值 PSQI总分 697/1 763 Ref Ref Ref 49/105 1.34(0.90~1.99) 0.148 1.67(1.09~2.56) 0.019 0.75(0.41~1.38) 0.360 睡眠质量 590/1 435 Ref Ref Ref 156/433 0.81(0.65~1.01) 0.058 0.90(0.71~1.13) 0.357 0.67(0.48~0.93) 0.017 入睡时间 580/1 497 Ref Ref Ref 166/371 1.28(1.02~1.61) 0.035 1.61(1.26~2.07) <0.001 1.02(1.00~1.04) 0.414 睡眠时间 648/1 695 Ref Ref Ref 98/173 2.11(1.54~2.90) <0.001 2.19(1.56~3.08) <0.001 1.05(0.65~1.70) 0.834 睡眠效率 670/1 671 Ref Ref Ref 76/197 0.94(0.69~1.27) 0.683 0.93(0.67~1.29) 0.655 0.71(0.46~1.11) 0.133 睡眠紊乱 665/1 701 Ref Ref Ref 81/167 1.47(1.07~2.02) 0.018 1.69(1.20~2.39) 0.003 1.03(0.64~1.67) 0.903 催眠药物使用 729/1 818 Ref Ref Ref 17/50 0.77(0.43~1.39) 0.386 0.92(0.49~1.74) 0.806 0.65(0.28~1.51) 0.317 日间功能障碍 463/1 117 Ref Ref Ref 283/751 0.85(0.71~1.03) 0.103 1.02(0.83~1.25) 0.862 0.85(0.65~1.12) 0.241
下载: 导出CSV
表 3 睡眠情况与NAFLD不同程度的关联分析
Table 3. The association between sleep condition and different severity in NAFLD
变量 患病率 单因素模型 年龄性别校正模型 多因素校正模型 OR(95%CI) P值 OR(95%CI) P值 OR(95%CI) P值 SFL vs non-NAFLD PSQI总分 594/1 763 Ref Ref Ref 30/105 0.96(0.61~1.52) 0.865 1.14(0.70~1.86) 0.600 0.67(0.36~1.25) 0.208 睡眠质量 507/1 435 Ref Ref Ref 117/433 0.70(0.55~0.90) 0.005 0.78(0.60~1.00) 0.054 0.63(0.45~0.89) 0.008 入睡时间 507/1 497 Ref Ref Ref 94/371 0.79(0.61~1.04) 0.089 0.96(0.72~1.28) 0.769 0.84(0.74~1.43) 0.059 睡眠时间 568/1 695 Ref Ref Ref 56/173 1.38(0.96~1.98) 0.083 1.29(0.88~1.90) 0.199 0.83(0.50~1.37) 0.470 睡眠效率 560/1 671 Ref Ref Ref 64/197 0.95(0.69~1.30) 0.731 0.91(0.64~1.29) 0.601 0.74(0.47~1.15) 0.181 睡眠紊乱 577/1 701 Ref Ref Ref 47/167 0.98(0.68~1.42) 0.920 1.06(0.72~1.58) 0.760 0.83(0.50~1.38) 0.466 催眠药物使用 610/1 818 Ref Ref Ref 14/50 0.76(0.40~1.43) 0.390 0.90(0.46~1.78) 0.769 0.68(0.29~1.59) 0.378 日间功能障碍 401/1 117 Ref Ref Ref 223/751 0.78(0.64~0.95) 0.055 0.94(0.76~1.17) 0.562 0.81(0.61~1.07) 0.140 NASH vs non-NAFLD PSQI总分 103/1 763 Ref Ref Ref 19/105 3.51(2.01~6.14) <0.001 4.16(2.35~7.37) <0.001 1.31(0.54~3.15) 0.547 睡眠质量 83/1 435 Ref Ref Ref 39/433 1.43(0.96~2.15) 0.081 1.53(1.02~2.30) 0.042 1.02(0.59~1.78) 0.938 入睡时间 50/1 497 Ref Ref Ref 72/371 6.44(4.36~9.53) <0.001 7.35(4.92~10.99) <0.001 4.04(2.33~7.03) <0.001 睡眠时间 80/1 695 Ref Ref Ref 42/173 7.33(4.72~11.39) <0.001 8.54(5.40~13.52) <0.001 3.53(1.83~6.82) <0.001 睡眠效率 110/1 671 Ref Ref Ref 12/197 0.90(0.48~1.69) 0.748 0.98(0.52~1.84) 0.953 0.42(0.17~1.03) 0.058 睡眠紊乱 88/1 701 Ref Ref Ref 34/167 4.65(2.96~7.32) <0.001 5.06(3.19~8.03) <0.001 2.96(1.48~5.93) 0.002 催眠药物使用 119/1 818 Ref Ref Ref 3/50 0.83(0.25~2.75) 0.763 1.05(0.31~3.52) 0.939 0.42(0.07~2.45) 0.335 日间功能障碍 62/1 117 Ref Ref Ref 60/751 1.35(0.93~1.97) 0.114 1.45(0.99~2.11) 0.056 1.23(0.75~2.01) 0.412
下载: 导出CSV
-
[1] RIAZI K, AZHARI H, CHARETTE JH, et al. The prevalence and incidence of NAFLD worldwide: A systematic review and meta-analysis[J]. Lancet Gastroenterol Hepatol, 2022, 7( 9): 851- 861. DOI: 10.1016/S2468-1253(22)00165-0. [2] PAIK JM, HENRY L, YOUNOSSI Y, et al. The burden of nonalcoholic fatty liver disease(NAFLD) is rapidly growing in every region of the world from 1990 to 2019[J]. Hepatol Commun, 2023, 7( 10): e0251. DOI: 10.1097/HC9.0000000000000251. [3] LING Z, ZHANG CC, HE J, et al. Association of healthy lifestyles with non-alcoholic fatty liver disease: A prospective cohort study in Chinese government employees[J]. Nutrients, 2023, 15( 3): 604. DOI: 10.3390/nu15030604. [4] HUANG DQ, NOUREDDIN N, AJMERA V, et al. Type 2 diabetes, hepatic decompensation, and hepatocellular carcinoma in patients with non-alcoholic fatty liver disease: An individual participant-level data meta-analysis[J]. Lancet Gastroenterol Hepatol, 2023, 8( 9): 829- 836. DOI: 10.1016/S2468-1253(23)00157-7. [5] JULIÁN MT, BALLESTA S, PERA G, et al. Abdominal obesity and dsyglycemia are risk factors for liver fibrosis progression in NAFLD subjects: A population-based study[J]. Front Endocrinol(Lausanne), 2022, 13: 1051958. DOI: 10.3389/fendo.2022.1051958. [6] DUAN D, KIM LJ, JUN JC, et al. Connecting insufficient sleep and insomnia with metabolic dysfunction[J]. Ann N Y Acad Sci, 2023, 1519( 1): 94- 117. DOI: 10.1111/nyas.14926. [7] National Workshop on Fatty Liver and Alcoholic Liver Disease, Chinese Society of Hepatology, Chinese Medical Association; Fatty Liver Expert Committee, Chinese Medical Doctor Association. Guidelines of prevention and treatment for nonalcoholic fatty liver disease: A 2018 update[J]. J Clin Hepatol, 2018, 34( 5): 947- 957. DOI: 10.3969/j.issn.1001-5256.2018.05.007.中华医学会肝病学分会脂肪肝和酒精性肝病学组, 中国医师协会脂肪性肝病专家委员会. 非酒精性脂肪性肝病防治指南(2018年更新版)[J]. 临床肝胆病杂志, 2018, 34( 5): 947- 957. DOI: 10.3969/j.issn.1001-5256.2018.05.007. [8] HU Y, LI HJ, ZHANG H, et al. ZSP1601, a novel pan-phosphodiesterase inhibitor for the treatment of NAFLD, A randomized, placebo-controlled phase Ib/IIa trial[J]. Nat Commun, 2023, 14( 1): 6409. DOI: 10.1038/s41467-023-42162-0. [9] ZHAO JJ, WANG QY, ZHAO XY, et al. Electro-acupuncture reduced steatosis on MRI-PDFF in patients with non-alcoholic steatohepatitis: A randomized controlled pilot clinical trial[J]. Chin Med, 2023, 18( 1): 19. DOI: 10.1186/s13020-023-00724-w. [10] MOLLAYEVA T, THURAIRAJAH P, BURTON K, et al. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis[J]. Sleep Med Rev, 2016, 25: 52- 73. DOI: 10.1016/j.smrv.2015.01.009. [11] NOBLE WS. How does multiple testing correction work?[J]. Nat Biotechnol, 2009, 27( 12): 1135- 1137. DOI: 10.1038/nbt1209-1135. [12] ZHOU JH, ZHOU F, WANG WX, et al. Epidemiological features of NAFLD from 1999 to 2018 in China[J]. Hepatology, 2020, 71( 5): 1851- 1864. DOI: 10.1002/hep.31150. [13] ZHOU F, ZHOU JH, WANG WX, et al. Unexpected rapid increase in the burden of NAFLD in China from 2008 to 2018: A systematic review and meta-analysis[J]. Hepatology, 2019, 70( 4): 1119- 1133. DOI: 10.1002/hep.30702. [14] YOUNOSSI ZM, COREY KE, LIM JK. AGA clinical practice update on lifestyle modification using diet and exercise to achieve weight loss in the management of nonalcoholic fatty liver disease: Expert review[J]. Gastroenterology, 2021, 160( 3): 912- 918. DOI: 10.1053/j.gastro.2020.11.051. [15] WANG CE, XU WT, GONG J, et al. Research progress in the treatment of non-alcoholic fatty liver disease[J]. Clin J Med Offic, 2022, 50( 9): 897- 899, 903. DOI: 10.16680/j.1671-3826.2022.09.06.王彩娥, 许文涛, 宫建, 等. 非酒精性脂肪性肝病治疗研究进展[J]. 临床军医杂志, 2022, 50( 9): 897- 899, 903. DOI: 10.16680/j.1671-3826.2022.09.06. [16] YU LB, LIN CL, CHEN XH, et al. A meta-analysis of sleep disorders and nonalcoholic fatty liver disease: Potential causality and symptom management[J]. Gastroenterol Nurs, 2022, 45( 5): 354- 363. DOI: 10.1097/SGA.0000000000000658. [17] MESARWI OA, LOOMBA R, MALHOTRA A. Obstructive sleep apnea, hypoxia, and nonalcoholic fatty liver disease[J]. Am J Respir Crit Care Med, 2019, 199( 7): 830- 841. DOI: 10.1164/rccm.201806-1109TR. [18] WANG HL, GU YQ, ZHENG LX, et al. Association between bedtime and the prevalence of newly diagnosed non-alcoholic fatty liver disease in adults[J]. Liver Int, 2018, 38( 12): 2277- 2286. DOI: 10.1111/liv.13896. [19] ZAREAN E, LOOHA MA, AMINI P, et al. Sleep characteristics of middle-aged adults with non-alcoholic fatty liver disease: Findings from the Shahrekord PERSIAN cohort study[J]. BMC Public Health, 2023, 23( 1): 312. DOI: 10.1186/s12889-023-15251-4. [20] LIU HW, HUANG SL, XU MD, et al. The association between sleep duration, quality, and nonalcoholic fatty liver disease: A cross-sectional study[J]. Open Med(Wars), 2023, 18( 1): 20230670. DOI: 10.1515/med-2023-0670. -

 本文二维码
本文二维码
计量
- 文章访问数: 1317
- HTML全文浏览量: 479
- PDF下载量: 139
- 被引次数: 0

