
 PDF下载 ( 771 KB)
PDF下载 ( 771 KB)

甲胎蛋白和甲胎蛋白异质体比率(AFP-L3%)对HBV相关早期肝细胞癌的诊断效能分析
DOI: 10.3969/j.issn.1001-5256.2023.11.014
Diagnostic efficacy of alpha-fetoprotein and alpha-fetoprotein L3% in hepatitis B virus-related early-stage hepatocellular carcinoma
-
摘要:
目的 探讨甲胎蛋白(AFP)、AFP异质体L3(AFP-L3)在HBV相关早期肝细胞癌(HCC)中的诊断效能及最佳截断值。 方法 纳入2019年1月—2022年7月在中山大学附属第三医院就诊的首次诊断且尚未治疗的HBV相关HCC患者(HCC组)共1 080例(其中中国肝癌分期Ⅰa~Ⅱa期肝癌620例),346例慢性乙型肝炎患者(CHB组)和293例HBV相关肝硬化患者(LC组)为对照组,分析AFP和AFP-L3%筛查HBV相关早期HCC的诊断效能,包括灵敏度、特异度、受试者工作特征曲线下面积(AUC)等。偏态分布的计量资料两组间比较采用Mann-Whitney U检验,多组间比较采用Kruskal-Wallis H检验,进一步两两比较采用Bonferroni法。 结果 HCC组AFP、AFP-L3%水平显著高于CHB组和LC组(H分别为542.479、418.974,P值均<0.001)。在早期HCC中,AFP和AFP-L3%最佳截断值分别为8.7 ng/mL和5%,AFP单用时AUC最高,为0.816,灵敏度和特异度分别为66.9%、85.1%;联合使用AFP-L3%与单用AFP的AUC无明显差异(Z=0.609,P=0.543),但均显著高于单用AFP-L3%(AFP vs AFP-L3%:Z=8.173,P<0.001;AFP+AFP-L3% vs AFP-L3%:Z=8.802,P<0.001)。 结论 AFP对HBV相关早期HCC有较好的诊断价值,并且优于AFP-L3%,为了提高早期HCC的检出率,应该下调AFP的筛查截断值。 Abstract:Objective To investigate the diagnostic efficacy and optimal cut-off values of alpha-fetoprotein (AFP) and alpha-fetoprotein variant L3 (AFP-L3) in hepatitis B virus (HBV)-related early-stage hepatocellular carcinoma (HCC). Methods A total of 1 080 patients with HBV-related HCC (HBV-HCC) who were diagnosed for the first time and not yet treated in The Third Affiliated Hospital of Sun Yat-Sen University from January 2019 to July 2022 were enrolled as HCC group in the study, among whom there were 620 patients with CNLC Ⅰa-Ⅱa HCC, and in addition, 346 patients with HBV-related chronic hepatitis B (CHB group) and 293 patients with HBV-related liver cirrhosis (LC group) were enrolled as controls. The diagnostic efficacy of AFP and AFP-L3% in screening for HBV-related early-stage HCC was analyzed, including sensitivity, specificity, and the area under the ROC curve (AUC). The Mann-Whitney U test was used for comparison of continuous data with skewed distribution between two groups; the Kruskal-Wallis H test was used for comparison between multiple groups, and the Bonferroni method was used for further comparison between two groups. Results The HCC group had significantly higher levels of AFP and AFP-L3% than the CHB group and the LC group (H=542.479 and 418.974, both P<0.001). In early-stage HCC, AFP and AFP-L3% had an optimal cut-off value of 8.7 ng/mL and 5%, respectively, and AFP alone had the largest AUC of 0.816, with a sensitivity of 66.9% and a specificity of 85.1%. There was no significant difference in AUC between AFP-L3%+AFP and AFP alone (Z=0.609, P=0.543), but both AFP-L3%+AFP and AFP alone had a significantly larger AUC than AFP-L3% alone (AFP vs AFP-L3%: Z=8.173, P<0.001; AFP+AFP-L3% vs AFP-L3%: Z=8.802, P<0.001). Conclusion AFP has a good value and is superior to AFP-L3% in the diagnosis of HBV-related early-stage HCC, and the screening cut-off value of AFP should be lowered in order to improve the detection rate of early-stage HCC. -
Key words:
- Hepatitis B virus /
- Liver Cirrhosis /
- Carcinoma, Hepatocellular /
- alpha-Fetoproteins /
- Diagnosis
-
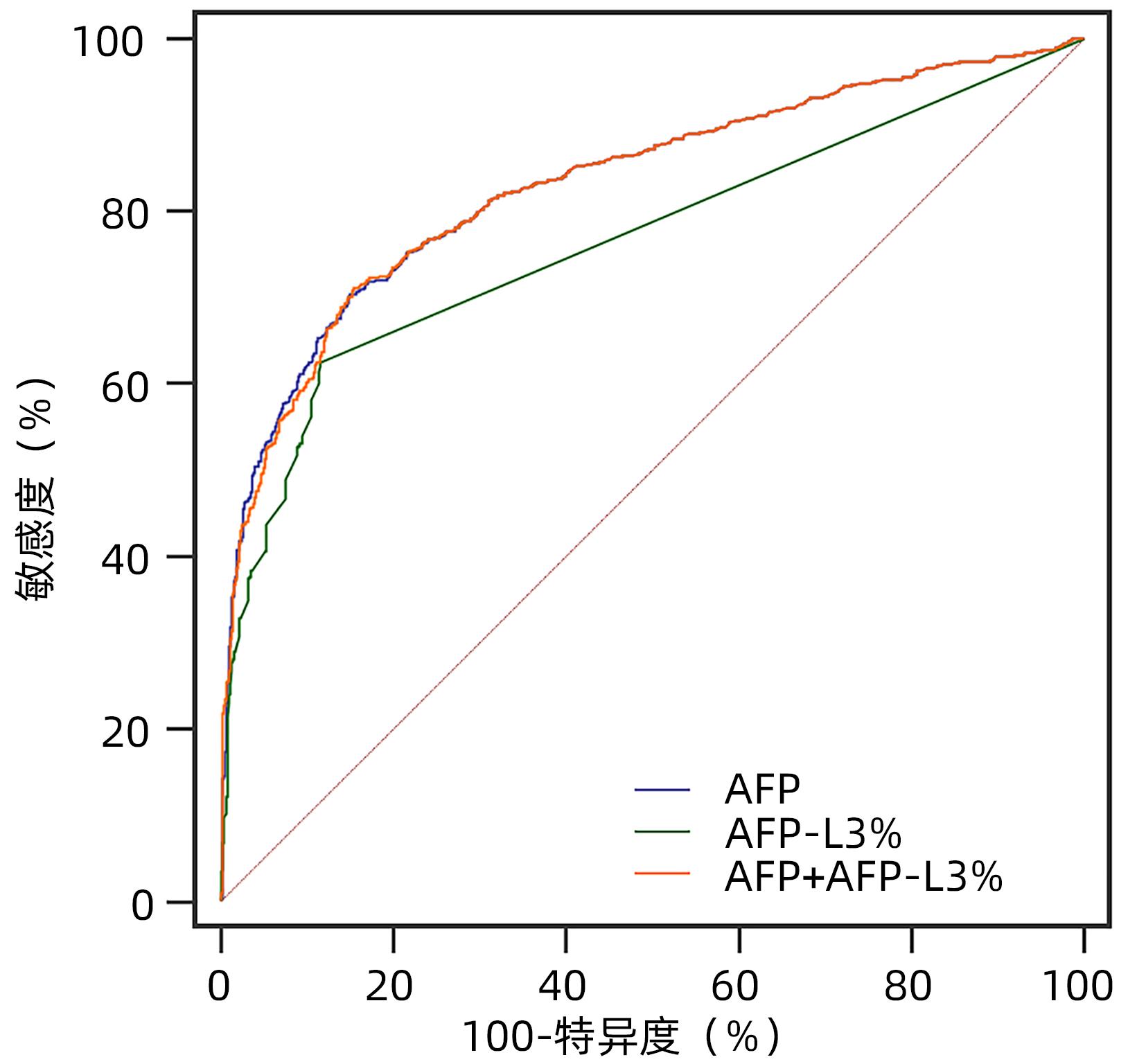
图 1 AFP、AFP-L3%单独及联合诊断总体HCC的ROC曲线
Figure 1. ROC curve of AFP, AFP-L3% alone and combined about the diagnosis of total HCC
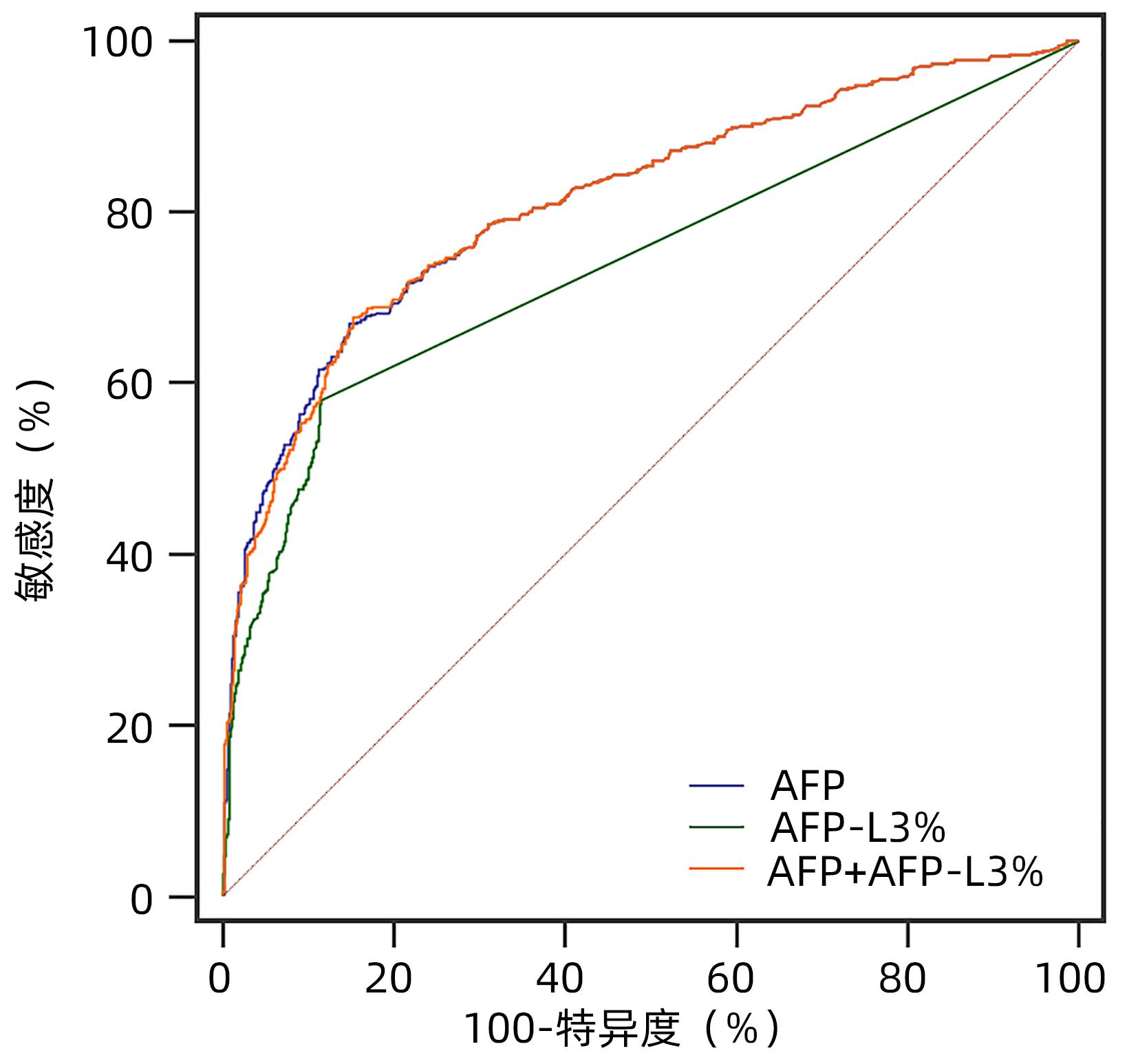
图 2 AFP、AFP-L3%单独及联合诊断早期HCC的ROC曲线
Figure 2. ROC curve of AFP, AFP-L3% alone and combined about diagnosis of CNLC early stage HCC
表 1 3组患者临床基线特点及AFP、AFP-L3、AFP-L3%的比较
Table 1. Comparison of clinical baseline characteristics and distribution of AFP, AFP-L3 and AFP-L3% in three groups
项目 CHB组(n=346) LC组(n=293) HCC组(n=1 080) 统计值 P值 年龄(岁) 43.0(34.8~50.0) 52.0(45.0~59.0) 55.5(48.0~63.0) H=248.327 <0.001 男/女(例) 249/97 236/57 969/111 χ2=67.783 <0.001 HBeAg阳性1)[例(%)] 86/333(25.8) 47/283(16.6) 229/1 068(21.4) χ2=20.143 <0.001 HBV DNA≥100 IU/mL1)[例(%)] 110/341(32.3) 68/290(23.4) 569/1 029(55.3) χ2=136.770 <0.001 ALT(U/L) 24.0(18.0~30.0) 25.0(19.0~31.0) 33.0(24.0~51.0) H=208.268 <0.001 Child-Pugh分级(A/B/C,例) 333/13/0 183/86/24 848/195/37 χ2=115.502 <0.001 AFP(ng/mL) 3.2(2.4~4.7) 3.9(2.4~7.2) 25.8(6.7~176.6) H=542.497 <0.001 AFP-L3(ng/mL) 0.6(0.6~0.6) 0.6(0.6~0.6) 2.7(0.6~23.4) H=456.749 <0.001 AFP-L3(%) 5.0(5.0~5.0) 5.0(5.0~5.0) 9.0(5.0~14.2) H=418.974 <0.001 注:1)部分指标的观察例数有缺失,原因为部分患者住院期间未能完善相关检查。  下载: 导出CSV
下载: 导出CSV
表 2 对照组与早期HCC组AFP、AFP-L3、AFP-L3%水平比较
Table 2. Comparison of AFP, AFP-L3 and AFP-L3% levels between the control group and the early stage HCC
项目 对照组(n=639) 早期HCC组(n=620) Z值 P值 AFP(ng/mL) 3.5(2.4~5.9) 18.7(5.5~121.4) -19.381 <0.001 AFP-L3(ng/mL) 0.6(0.6~0.6) 1.9(0.6~14.7) -18.352 <0.001 AFP-L3(%) 5.0(5.0~5.0) 8.0(5.0~13.1) -17.475 <0.001
下载: 导出CSV
表 3 ALT正常对照组与ALT正常HCC组的AFP、AFP-L3、AFP-L3%水平比较
Table 3. Comparison of AFP, AFP-L3 and AFP-L3% levels between the control group with normal ALT and the HCC group with normal ALT
项目 ALT正常对照组(n=597) ALT正常HCC组(n=598) Z值 P值 AFP(ng/mL) 3.4(2.4~5.7) 19.6(5.2~162.4) -18.654 <0.001 AFP-L3(ng/mL) 0.6(0.6~0.6) 2.3(0.6~23.5) -18.512 <0.001 AFP-L3(%) 5.0(5.0~5.0) 8.7(5.0~14.2) -17.816 <0.001
下载: 导出CSV
表 4 不同ALT水平的HCC组的AFP、AFP-L3、AFP-L3%水平比较
Table 4. Comparison of AFP, AFP-L3 and AFP-L3% levels among HCC groups with different ALT levels
项目 ALT正常HCC组(n=598) ALT升高HCC组(n=482) Z值 P值 AFP(ng/mL) 19.6(5.2~162.4) 32.7(9.1~190.4) -2.961 0.003 AFP-L3(ng/mL) 2.3(0.6~23.5) 3.2(0.6~22.8) -1.854 0.064 AFP-L3(%) 8.7(5.0~14.2) 9.4(5.0~14.2) -1.499 0.134
下载: 导出CSV
表 5 AFP、AFP-L3%在总体HCC中的诊断效能分析
Table 5. Analysis of the diagnostic efficacy of AFP and AFP-L3% in overall HCC
指标 AUC(95%CI) 截断值 敏感度(%) 特异度(%) 约登指数 阳性预测值(%) 阴性预测值(%) AFP(ng/mL) 0.834(0.815~0.853) 8.5 70.4 85.0 0.554 88.8 62.9 AFP-L3%(%) 0.766(0.748~0.785) 5.0 62.4 88.4 0.508 90.1 58.2 AFP+AFP-L3% 0.833(0.814~0.852) NA 71.1 84.5 0.556 88.6 63.4 注:NA,无确切截断值。
下载: 导出CSV
表 6 AFP、AFP-L3%在早期HCC中的诊断性能及截断值比较
Table 6. Diagnostic performance analysis of AFP and AFP-L3% in early stage HCC and comparison of different cut-off points
项目 截断值 敏感度(%) 特异度(%) 阳性预测值 (%) 阴性预测值 (%) Kappa值 AUC(95%CI) AFP(ng/mL) 8.7 66.9 85.1 81.4 72.6 0.522 0.816(0.792~0.839) 20 48.5 94.5 89.6 65.4 0.434 200 20.2 99.2 96.2 56.2 0.196 400 11.6 99.5 96.0 53.7 0.113 AFP-L3%(%) 5 58.1 88.4 82.9 68.5 0.467 0.741(0.718~0.764) 10 40.3 93.4 85.6 61.7 0.340 15 17.9 99.2 95.7 55.5 0.173 AFP+AFP-L3% AFP 8.7+AFP-L3% 5 67.7 84.7 81.1 73.0 0.525 0.814(0.790~0.838) AFP 20+AFP-L3% 10 56.9 90.6 85.5 68.4 0.478 AFP 20+AFP-L3% 15 51.5 94.1 89.4 66.6 0.458 AFP 200+AFP-L3% 10 46.3 93.0 86.4 64.1 0.395 AFP 200+AFP-L3% 15 29.4 98.6 95.3 59.0 0.282 AFP 400+AFP-L3% 10 43.5 93.1 86.0 63.0 0.369 AFP 400+AFP-L3% 15 24.2 98.9 95.5 57.4 0.234
下载: 导出CSV
-
[1] SUNG H, FERLAY J, SIEGEL RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71( 3): 209- 249. DOI: 10.3322/caac.21660. [2] ALLEMANI C, MATSUDA T, DI CARLO V, et al. Global surveillance of trends in cancer survival 2000-14(CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries[J]. Lancet, 2018, 391( 10125): 1023- 1075. DOI: 10.1016/S0140-6736(17)33326-3. [3] TSILIMIGRAS DI, BAGANTE F, SAHARA K, et al. Prognosis after resection of Barcelona clinic liver cancer(BCLC) stage 0, A, and B hepatocellular carcinoma: A comprehensive assessment of the current BCLC classification[J]. Ann Surg Oncol, 2019, 26( 11): 3693- 3700. DOI: 10.1245/s10434-019-07580-9. [4] HEIMBACH JK, KULIK LM, FINN RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma[J]. Hepatology, 2018, 67( 1): 358- 380. DOI: 10.1002/hep.29086. [5] Professional Committee for Prevention and Control of Hepatobiliary and Pancreatic Diseases of Chinese Preventive Medicine Association; Professional Committee for Hepatology, Chinese Research Hospital Association; Chinese Society of Hepatology, Chinese Medical Association, et al. Guideline for stratified screening and surveillance of primary liver cancer(2020 edition)[J]. J Clin Hepatol, 2021, 37( 2): 286- 295. DOI: 10.3969/j.issn.1001-5256.2021.02.009.中华预防医学会肝胆胰疾病预防与控制专业委员会, 中国研究型医院学会肝病专业委员会, 中华医学会肝病学分会, 等. 原发性肝癌的分层筛查与监测指南(2020版)[J]. 临床肝胆病杂志, 2021, 37( 2): 286- 295. DOI: 10.3969/j.issn.1001-5256.2021.02.009. [6] TZARTZEVA K, OBI J, RICH NE, et al. Surveillance imaging and alpha fetoprotein for early detection of hepatocellular carcinoma in patients with cirrhosis: A meta-analysis[J]. Gastroenterology, 2018, 154( 6): 1706- 1718.e1. DOI: 10.1053/j.gastro.2018.01.064. [7] SUGIYAMA H, TAKESHITA H, TACHibANA K, et al. Lens culinaris agglutinin-reactive fraction of alpha-fetoprotein as a tumor marker in a patient with nonseminomatous germ cell tumor with normal alpha-fetoprotein level[J]. Clin Genitourin Cancer, 2020, 18( 3): e309- e311. DOI: 10.1016/j.clgc.2019.12.013. [8] Bureau of Medical Administration, National Health Commission of the People’s Republic of China. Guidelines for diagnosis and treatment of primary liver cancer in China(2019 edition)[J]. J Clin Hepatol, 2020, 36( 2): 277- 292. DOI: 10.3969/j.issn.1001-5256.2020.02.007.中华人民共和国国家卫生健康委员会医政医管局. 原发性肝癌诊疗规范(2019年版)[J]. 临床胆病杂志, 2020, 36( 2): 277- 292. DOI: 10.3969/j.issn1001-5256.2020.02.007. [9] Chinese Society of Hepatology, Chinese Medical Association; Chinese Society of Infectious Diseases, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B(version 2019)[J]. J Clin Hepatol, 2019, 35( 12): 2648- 2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.中华医学会感染病学分会, 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35( 12): 2648- 2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007. [10] Chinese Society of Hepatology, Chinese Medical Association. Chinese guidelines on the management of liver cirrhosis[J]. J Clin Hepatol, 2019, 35( 11): 2408- 2425. DOI: 10.3969/j.issn.1001- 5256.2019.11.006.中华医学会肝病学分会. 肝硬化诊治指南[J]. 临床肝胆病杂志, 2019, 35( 11): 2408- 2425. DOI: 10.3969/j.issn.1001-5256.2019.11.006. [11] WANG XP, WANG QX. Alpha-fetoprotein and hepatocellular carcinoma immunity[J]. Can J Gastroenterol Hepatol, 2018, 2018: 9049252. DOI: 10.1155/2018/9049252. [12] SAUZAY C, PETIT A, BOURGEOIS AM, et al. Alpha-foetoprotein(AFP): A multi-purpose marker in hepatocellular carcinoma[J]. Clin Chim Acta, 2016, 463: 39- 44. DOI: 10.1016/j.cca.2016.10.006. [13] SINGAL AG, HAALAND B, PARIKH ND, et al. Comparison of a multitarget blood test to ultrasound and alpha-fetoprotein for hepatocellular carcinoma surveillance: Results of a network meta-analysis[J]. Hepatol Commun, 2022, 6( 10): 2925- 2936. DOI: 10.1002/hep4.2045. [14] YI XY, YU S, BAO YX. Alpha-fetoprotein-L3 in hepatocellular carcinoma: A meta-analysis[J]. Clin Chim Acta, 2013, 425: 212- 220. DOI: 10.1016/j.cca.2013.08.005. [15] ZHOU JM, WANG T, ZHANG KH. AFP-L3 for the diagnosis of early hepatocellular carcinoma: A meta-analysis[J]. Medicine, 2021, 100( 43): e27673. DOI: 10.1097/MD.0000000000027673. [16] ZHANG ZG, ZHANG YY, WANG YY, et al. Alpha-fetoprotein-L3 and Golgi protein 73 may serve as candidate biomarkers for diagnosing alpha-fetoprotein-negative hepatocellular carcinoma[J]. Onco Targets Ther, 2016, 9: 123- 129. DOI: 10.2147/OTT.S90732. [17] CHOI JY, JUNG SW, KIM HY, et al. Diagnostic value of AFP-L3 and PIVKA-II in hepatocellular carcinoma according to total-AFP[J]. World J Gastroenterol, 2013, 19( 3): 339- 346. DOI: 10.3748/wjg.v19.i3.339. [18] STERLING RK, JEFFERS L, GORDON F, et al. Utility of Lens culinaris agglutinin-reactive fraction of α-fetoprotein and des-gamma-carboxy prothrombin, alone or in combination, as biomarkers for hepatocellular carcinoma[J]. Clin Gastroenterol Hepatol, 2009, 7( 1): 104- 113. DOI: 10.1016/j.cgh.2008.08.041. [19] CHOI J, KIM GA, HAN S, et al. Longitudinal assessment of three serum biomarkers to detect very early-stage hepatocellular carcinoma[J]. Hepatology, 2019, 69( 5): 1983- 1994. DOI: 10.1002/hep.30233. [20] LOK AS, STERLING RK, EVERHART JE, et al. Des-gamma-carboxy prothrombin and alpha-fetoprotein as biomarkers for the early detection of hepatocellular carcinoma[J]. Gastroenterology, 2010, 138( 2): 493- 502. DOI: 10.1053/j.gastro.2009.10.031. [21] MARRERO JA, FENG ZD, WANG YH, et al. Alpha-fetoprotein, des-gamma carboxyprothrombin, and lectin-bound alpha-fetoprotein in early hepatocellular carcinoma[J]. Gastroenterology, 2009, 137( 1): 110- 118. DOI: 10.1053/j.gastro.2009.04.005. [22] KUDO M, KAWAMURA Y, HASEGAWA K, et al. Management of hepatocellular carcinoma in Japan: JSH consensus statements and recommendations 2021 update[J]. Liver Cancer, 2021, 10( 3): 181- 223. DOI: 10.1159/000514174. [23] ZHANG JX, CHEN G, ZHANG P, et al. The threshold of alpha-fetoprotein(AFP) for the diagnosis of hepatocellular carcinoma: A systematic review and meta-analysis[J]. PLoS One, 2020, 15( 2): e0228857. DOI: 10.1371/journal.pone.0228857. [24] LI B, ZHAO YY, DUAN Y, et al. Diagnostic value of alpha-fetoprotein heterogeneity L3 on early primary liver cancer[J/CD]. Chin J Liver Dis(Electronic Version), 2018, 10( 4): 7- 11. DOI: 10.3969/j.issn.1674-7380.2018.04.002.李贲, 赵莹莹, 段英, 等. 甲胎蛋白异质体L3对早期原发性肝癌的诊断价值[J/CD]. 中国肝脏病杂志(电子版), 2018, 10( 4): 7- 11. DOI: 10.3969/j.issn.1674-7380.2018.04.002. [25] TIAN Z, ZHANG JH. A threshold analysis of alpha-fetoprotein in diagnosis and screening of hepatocellular carcinoma[J]. J Clin Hepatol, 2018, 34( 11): 2352- 2355. DOI: 10.3969/j.issn.1001-5256.2018.11.016.田州, 张建淮. 甲胎蛋白诊断和筛查原发性肝癌的阈值分析[J]. 临床肝胆病杂志, 2018, 34( 11): 2352- 2355. DOI: 10.3969/j.issn.1001-5256.2018.11.016. [26] Chinese Society of Hepatology, Chinese Medical Association. Consensus on the secondary prevention for primary liver cancer(2021 edition)[J]. J Clin Hepatol, 2021, 37( 3): 532- 542. DOI: 10.3969/j.issn.1001-5256.2021.03.008.中华医学会肝病学分会. 原发性肝癌二级预防共识(2021年版)[J]. 临床肝胆病杂志, 2021, 37( 3): 532- 542. DOI: 10.3969/j.issn.1001-5256.2021.03.008. [27] CHEN SY, LI JH, TAN XD, et al. Clinical role of combining alpha-fetoprotein and lens culinaris agglutinin-reactive fraction of alpha-fetoprotein for hepatocellular carcinoma: Evidence from literature and an original study[J]. J Clin Lab Anal, 2020, 34( 7): e23262. DOI: 10.1002/jcla.23262. [28] GUAN GW, YAO MJ, QIAN XJ, et al. Value of combined measurement of alpha-fetoprotein and alpha-fetoprotein L3% in the diagnosis of hepatocellular carcinoma[J]. J Clin Hepatol, 2019, 35( 7): 1514- 1519. DOI: 10.3969/j.issn.1001-5256.2019.07.019.关贵文, 姚明解, 钱相君, 等. AFP和AFP-L3%联合检测在肝细胞癌诊断中的应用价值[J]. 临床肝胆病杂志, 2019, 35( 7): 1514- 1519. DOI: 10.3969/j.issn.1001-5256.2019.07.019. -

 本文二维码
本文二维码
计量
- 文章访问数: 272
- HTML全文浏览量: 109
- PDF下载量: 41
- 被引次数: 0

