
 PDF下载 ( 907 KB)
PDF下载 ( 907 KB)

改良BISAP评分系统的建立及其在重症急性胰腺炎早期诊断和预后评估中的意义
DOI: 10.3969/j.issn.1001-5256.2023.10.022
Establishment of a modified BISAP scoring system and its clinical significance in the early diagnosis and prognostic evaluation of severe acute pancreatitis
-
摘要:
目的 建立改良BISAP评分系统,比较并分析BISAP评分系统与改良BISAP评分系统对急性胰腺炎(AP)严重程度及病情评估的价值。 方法 新系统的建立:回顾性收集2019年1月—2021年12月中南大学湘雅三医院收治的1 033例AP患者的临床资料。根据修订版Atlanta分级将其分为轻症急性胰腺炎(MAP)组(n=827)和重症急性胰腺炎(SAP)组(n=206),比较两组患者临床特征、实验室指标及影像学资料的差异,将差异有统计学意义的指标进行二元Logistic回归分析,筛选出SAP的独立危险因素,利用受试者特征曲线(ROC曲线)得出各独立危险因素的最大约登指数对应的最佳截断值,并根据不同情况分别赋值为0或1分,结合BISAP评分系统,建立改良BISAP评分系统。新系统验证:回顾性收集2017年1月—2018年12月中南大学湘雅三医院收治的473例AP患者的临床资料,对其进行BISAP评分与改良BISAP评分,利用ROC曲线下面积(AUC)分析比较两个评分系统对AP病情严重程度、预后的预测价值。计数资料应用χ²检验或Fisher精确检验进行两组间比较;计量资料两组间比较采用成组t检验和Mann-Whitney U检验。 结果 新系统的建立:MAP组与SAP组患者在入院方式、住院天数、是否入住ICU、死亡人数、合并基础疾病、出现并发症方面差异均有统计学意义(P值均<0.05)。二元Logistic回归分析显示,体温、NLR、CRP、Alb、TG、D二聚体、纤维蛋白原、MCTSI评分为SAP的独立危险因素(P值均<0.05)。ROC曲线分析显示CRP(AUC=0.921)、NLR(AUC=0.798)、D二聚体(AUC=0.768)及MCTSI评分(AUC=0.931)对SAP有较好的预测价值,且上述四项指标联合预测的AUC为0.976,与单个指标、两项指标联合及三项指标联合相比,其诊断效能更高,且差异有统计学意义(P值均<0.05)。新评分系统验证:共纳入473例患者,其中MAP组408例,SAP组65例。两组患者在入院方式、住院天数、是否入住ICU、死亡人数、出现并发症方面差异有统计学意义(P值均<0.05)。在预测SAP方面,改良BISAP评分优于BISAP评分(AUC:0.972 vs 0.887,P<0.05),改良BISAP评分>3为最佳临界值。改良BISAP评分在预测AP患者死亡方面也有较高价值(AUC=0.910),但与BISAP评分系统(AUC=0.896)比较差异无统计学意义(P=0.707)。 结论 改良BISAP评分在预测AP严重程度方面优于BISAP评分,在预测AP患者死亡方面也有较高的价值,可以比较准确、客观且在早期评估AP患者病情。 Abstract:Objective To establish a modified BISAP scoring system, and to investigate the value of the BISAP scoring system versus the modified BISAP scoring system in assessing the severity and condition of acute pancreatitis (AP). Methods For the establishment of the new scoring system, a retrospective analysis was performed for the clinical data of 1 033 patients with AP who were admitted to Third Xiangya hospital of central South University from January 2019 to December 2021, and according to the revised Atlanta classification, they were divided into mild acute pancreatitis (MAP) group with 827 patients and severe acute pancreatitis (SAP) group with 206 patients. The two groups were compared in terms of clinical features, laboratory markers, and imaging data. A binary logistic regression analysis was performed for the statistically significant indicators to screen for the independent risk factors for SAP. The receiver operating characteristic (ROC) curve was used to obtain the optimal cut-off value corresponding to the maximum Youden index for each independent risk factor, and a score of 0 or 1 was assigned depending on different situations, which was integrated into the BISAP scoring system to establish a modified BISAP scoring system. For the validation of the new scoring system, a retrospective analysis was performed for the clinical data of 473 patients with AP who were admitted to Third Xiangya hospital of central South University from January 2017 to December 2018. BISAP score and modified BISAP score were determined for each patient, and the area under the ROC curve (AUC) was used to compare the value of the two scoring systems in predicting the severity and prognosis of AP. The chi-square test or the Fisher’s exact test was used for comparison of categorical data between two groups, and the independent-samples t test and the Mann-Whitney U test were used for comparison of continuous data between two groups. Results For the establishment of the new scoring system, there were significant differences between the MAP group and the SAP group in mode of admission, length of hospital stay, ICU admission rate, number of deaths, underlying diseases, and incidence rate of complications (all P<0.05). The binary logistic regression analysis showed that body temperature, neutrophil-to-lymphocyte ratio (NLR), C-reactive protein (CRP), albumin, triglycerides, D-dimer, fibrinogen, and MCTSI score were independent risk factors for SAP (all P<0.05). The ROC curve analysis showed that CRP (AUC=0.921), NLR (AUC=0.798), D-dimer (AUC=0.768), and MCTSI score (AUC=0.931) had a good predictive value for SAP, and the combination of these four indicators had an AUC of 0.976 and showed a significantly higher diagnostic efficiency than each indicator alone or the combination of two or three indicators (all P<0.05). For the validation of the new scoring system, a total of 473 patients were enrolled, with 408 in the MAP group and 65 in the SAP group, and there were significant differences between the two groups in mode of admission, length of hospital stay, ICU admission rate, number of deaths, and incidence rate of complications (all P<0.05). The modified BISAP score was better than the BISAP score in predicting SAP (AUC: 0.972 vs 0.887, P<0.05), with an optimal cut-off value of >3 points. The modified BISAP score also had a relatively high value in predicting the mortality of AP patients (AUC=0.910), but there was no significant difference between the modified BISAP score and the BISAP scoring system (AUC: 0.910 vs 0.896, P=0.707). Conclusion The modified BISAP score is better than the BISAP score in predicting the severity of AP and has a relatively high value in predicting the mortality of AP patients, giving a more accurate, objective, and early assessment of the condition of AP patients. -
Key words:
- Acute Pancreatitis /
- BISAP Score /
- Early Diagnosis /
- Prognosis
-
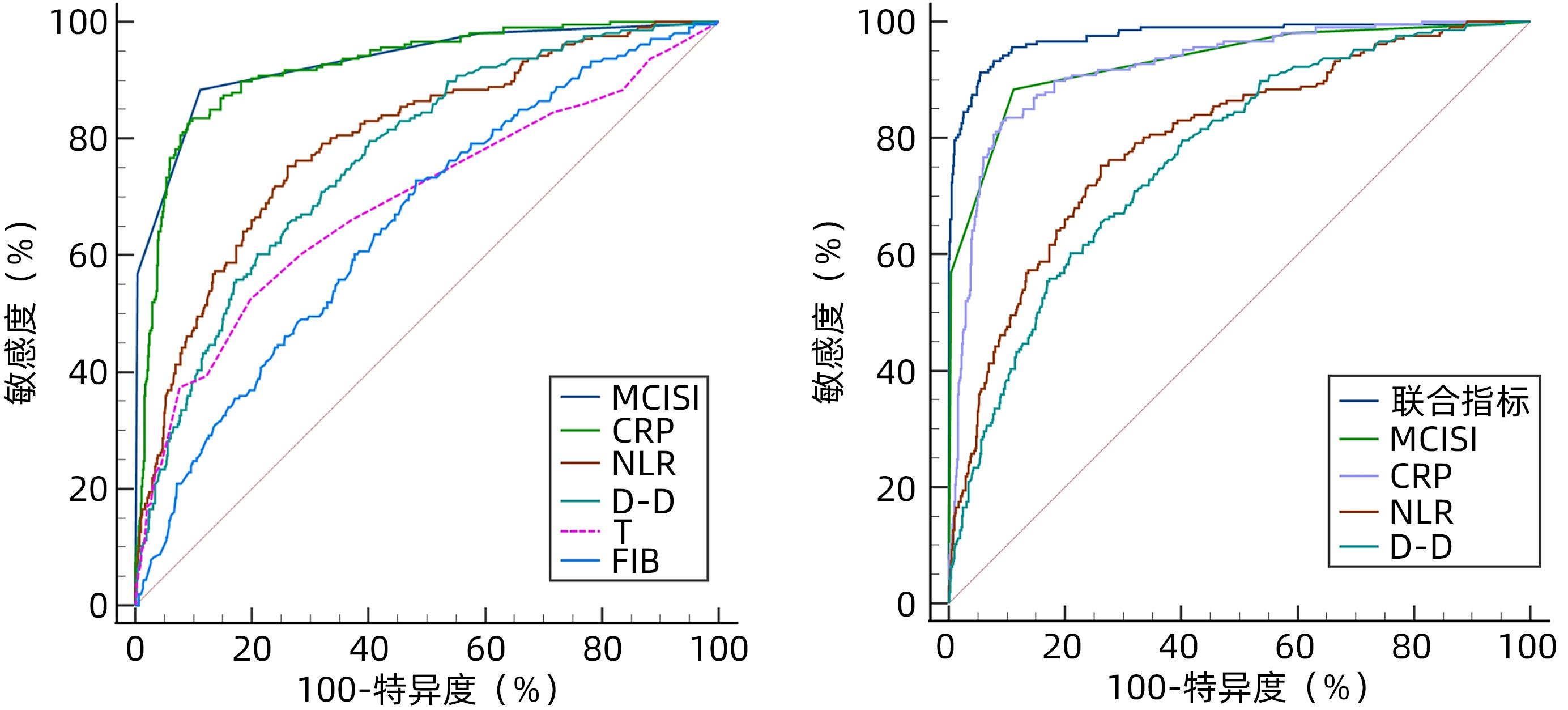
图 1 各指标预测AP患者严重程度的ROC曲线
注: 联合指标是MCTSI评分+CRP+NLR+D-D四项指标联合。
Figure 1. ROC curves of every Indicator for predicting the severity of acute pancreatitis
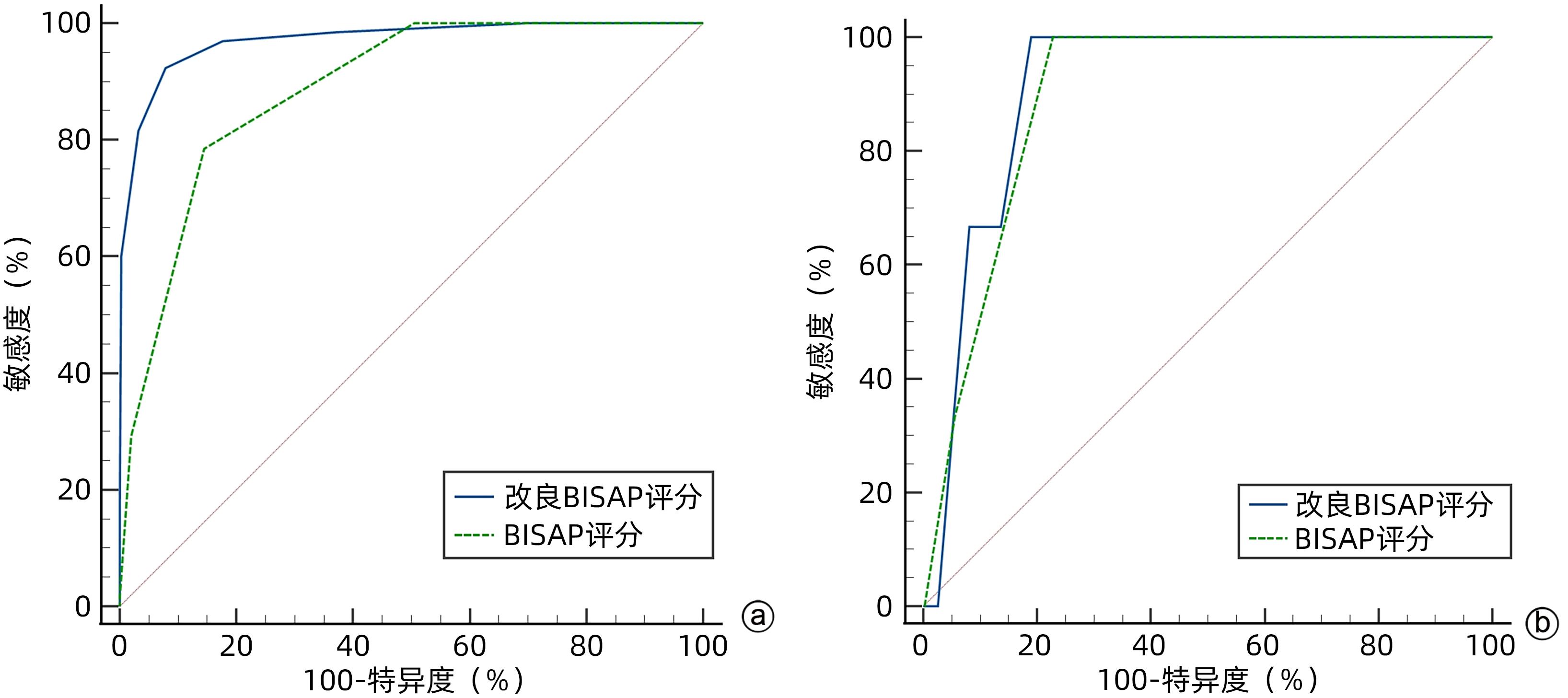
图 2 BISAP评分与改良BISAP评分预测SAP及AP死亡效能比较
注: a,预测SAP的效能;b,预测AP死亡效能。
Figure 2. Comparison of the ability of BISAP score and modified BISAP score to predict the severity and mortality of acute pancreatitis
表 1 患者的一般资料
Table 1. General information of patients
临床资料 MAP组(n=827) SAP组(n=206) 统计值 P值 年龄(岁) 46.22±14.72 47.23±14.56 t=-0.885 0.376 性别[例(%)] χ²=0.005 0.508 男 564(68.2) 141(68.4) 女 263(31.8) 65(31.6) 病因[例(%)] χ²=2.354 0.502 胆源性 297(35.9) 76(36.9) 脂源性 399(48.2) 106(51.5) 酒精性 25(3.0) 5(2.4) 其他 106(12.8) 19(9.2) 基础疾病[例(%)] χ²=15.302 0.004 高血压 121(14.6) 42(20.4) 糖尿病 148(17.9) 63(30.6) 脂肪肝 308(37.2) 64(31.1) 高脂血症 303(36.6) 108(52.4) 胆囊结石 212(25.6) 61(29.6) 入院方式[例(%)] χ²=216.775 <0.001 步行 689(83.3) 67(32.5) 非步行 138(16.7) 139(67.5) 住院天数(天) 8.0(6.0~11.0) 21.5(14.0~31.0) Z=17.520 <0.001 是否入住ICU[例(%)] χ²=432.798 <0.001 是 9(1.1) 108(52.4) 否 818(98.9) 98(47.6) 死亡[例(%)] 0(0.0) 7(3.4) χ²=138.361 <0.001 合并症[例(%)] χ²=87.405 <0.001 ARDS 0(0.0) 43(20.9) MODS 0(0.0) 9(4.4) 浆膜腔积液 69(8.3) 57(27.7) 胰周感染 13(1.6) 17(8.3) 脓毒血症 0(0.0) 11(5.3) 急性肾损伤 0(0.0) 16(7.8) 急性肝损伤 39(4.7) 30(14.6) 胰腺假性囊肿 12(1.5) 14(6.8)  下载: 导出CSV
下载: 导出CSV
表 2 SAP的单因素分析
Table 2. Single factor analysis of severe acute pancreatitis
临床资料 MAP组(n=827) SAP组(n=206) 统计值 P值 生命体征 体温(℃) 36.5(36.4~36.7) 36.8(36.5~37.0) Z=-8.664 <0.001 脉搏(次/min) 90.01±17.12 107.52±21.99 t=-10.654 <0.001 呼吸(次/min) 20(20~20) 22(20~25) Z=-12.080 <0.001 收缩压(mmHg) 126.61±16.77 132.18±26.46 t=-2.878 0.004 舒张压(mmHg) 80.06±11.03 78.70±13.74 t=1.324 0.187 血常规指标 WBC(×109/L) 10.60±4.14 14.22±5.60 t=-8.706 <0.001 N(×109/L) 8.57±3.87 12.50±5.33 t=-9.954 <0.001 L(×109/L) 1.23(0.92~1.60) 0.88(0.60~1.16) Z=-9.195 <0.001 NLR 6.69(4.26~9.97) 13.52(9.64~19.31) Z=-13.239 <0.001 Hb(g/L) 135.31±19.56 134.01±31.78 t=0.560 0.576 Plt(×109/L) 208.65±64.96 215.67±94.65 t=-1.007 0.315 HCT(%) 40.73±5.27 39.65±8.48 t=1.743 0.083 RDW(fL) 43.1(41.1~45.1) 44.6(42.7~47.5) Z=-6.764 <0.001 PDW(fL) 16.3(15.7~16.6) 16.5(16.2~16.9) Z=-5.376 <0.001 CRP(mg/L) 55.2(20.9~113.0) 258.1(211.0~301.3) Z=-18.742 <0.001 肝功能指标 ALT(U/L) 29(18~60) 24(15~54) Z=-2.786 0.005 AST(U/L) 26.0(18.0~44.0) 37.5(23.0~56.3) Z=-4.697 <0.001 TBil(μmol/L) 16.8(11.8~25.1) 17.5(10.6~28.5) Z=-0.245 0.807 DBil(μmol/L) 5.1(3.4~8.4) 6.7(3.3~13.5) Z=-2.544 0.011 TBA(μmol/L) 2.5(1.1~5.5) 3.0(1.4~6.1) Z=-1.977 0.048 Alb(g/L) 38.57±5.44 32.83±4.91 t=13.825 <0.001 GLB(g/L) 27.08±5.39 26.96±7.1 t=0.210 0.834 A/G 1.48±0.35 1.29±0.34 t=7.050 <0.001 肾功能指标 肌酐(mmol/L) 64(53~76) 76(56~118) Z=-6.147 <0.001 尿素(mmol/L) 4.23(3.28~5.33) 6.90(4.77~10.48) Z=-12.147 <0.001 尿酸(mmol/L) 309.89±110.83 331.83±142.91 t=-2.055 0.041 血脂指标 TC(mmol/L) 4.92(3.89~6.49) 4.60(3.18~7.19) Z=-1.745 0.081 TG(mmol/L) 2.45(1.16~5.98) 3.77(1.52~10.63) Z=-4.487 <0.001 HDL-C(mmol/L) 1.04(0.83~1.23) 0.76(0.53~1.03) Z=-9.109 <0.001 LDL-C(mmol/L) 2.44±1.09 2.23±1.10 t=2.415 0.016 电解质 血钙(mmol/L) 2.20±0.18 1.98±0.30 t=10.054 <0.001 血钾(mmol/L) 3.93±0.43 4.01±0.64 t=-1.792 0.074 血钠(mmol/L) 138.74±3.67 137.95±5.22 t=2.040 0.042 血氯(mmol/L) 103.0(100.5~105.4) 102.4(98.7~106.5) Z=-0.179 0.858 凝血功能指标 D-D(mg/L) 1.05(0.45~2.15) 3.26(1.50~6.20) Z=-11.920 <0.001 PT(s) 12.3(11.5~13.2) 13.1(12.2~14.1) Z=-7.586 <0.001
下载: 导出CSV
表 3 SAP的多因素Logistic回归分析
Table 3. Multivariate Logistic regression analysis of severe acute pancreatitis
变量 β值 SE Wald值 OR(95%CI) P值 体温(℃) 0.705 0.328 4.621 2.024(1.064~3.850) 0.032 NLR 0.099 0.036 7.431 1.104(1.028~1.185) 0.006 CRP(mg/L) 0.014 0.002 38.099 1.015(1.01~1.019) <0.001 Alb(g/L) -0.184 0.052 12.362 0.832(0.751~0.922) <0.001 TG(mmol/L) 0.072 0.033 4.832 1.075(1.008~1.147) 0.028 D-D(mg/L) 0.157 0.064 6.097 1.171(1.033~1.326) 0.014 FIB(g/L) -0.442 0.112 15.652 0.643(0.516~0.800) <0.001 MCTSI评分 1.174 0.137 73.247 3.233(2.471~4.230) <0.001
下载: 导出CSV
表 4 预测SAP的ROC曲线分析及诊断阈值
Table 4. ROC curves analysis and cut-off level for predicting the severity of acute pancreatitis
变量 AUC cut-off值 敏感度(%) 特异度(%) 95%CI 约登指数 体温 0.692 36.7 ℃ 52.4 80.3 0.647~0.736 0.327 NLR 0.798 9.66 75.2 73.9 0.763~0.832 0.491 CRP 0.921 175.5 mg/L 83.5 90.2 0.900~0.943 0.737 Alb 0.211 20.1 g/L 100 0.4 0.178~0.245 0.004 TG 0.601 7.51 mmol/L 34.5 79.7 0.557~0.645 0.142 D-D 0.768 1.375 mg/L 79.6 59.9 0.733~0.803 0.395 FIB 0.655 4.255 g/L 72.8 51.9 0.614~0.696 0.247 MCTSI评分 0.931 5 88.3 88.9 0.909~0.953 0.772 MCTSI评分+CRP 0.968 94.7 89.4 0.955~0.978 0.840 MCTSI评分+CRP+NLR 0.974 91.8 93.8 0.963~0.983 0.856 MCTSI评分+CRP+D-D 0.969 93.7 91.1 0.956~0.978 0.847 MCTSI评分+CRP+NLR+D-D 0.976 91.2 94.6 0.964~0.984 0.858
下载: 导出CSV
表 5 改良BISAP评分系统赋值表
Table 5. Modified BISAP scoring system assignment form
变量 0分 1分 血尿素(mmol/L)1) ≤9 >9 SIRS2) 无 有 年龄(岁) ≤60 >60 胸腔积液 无 有 MCTSI评分 ≤5 >5 CRP(mg/L) ≤175.5 >175.5 NLR ≤9.66 >9.66 D-D(mg/L) ≤1.375 >1.375 注:1)尿素2.86~8.92 mmol/L相当于尿素氮8~25 mg/dL。2)SIRS,全身炎症反应综合征,确诊至少具备以下2项:①体温<36 ℃/>38 ℃;②呼吸频率>20次/min或二氧化碳分压(PCO2)<32 mmHg;③脉搏>90次/min;④WBC>12×109/L或<4×109/L。
下载: 导出CSV
临床资料 MAP组(n=827) SAP组(n=206) 统计值 P值 INR 1.08(1.00~1.16) 1.15(1.07~1.25) Z=-7.564 <0.001 FIB(g/L) 4.2(3.2~5.8) 5.2(4.1~7.5) Z=-6.900 <0.001 PTA(%) 86.17±15.05 74.11±17.62 t=9.933 <0.001 APTT(s) 28.53±4.23 31.57±10.85 t=-3.950 <0.001 其他指标 总淀粉酶(U/L) 112.0(56.0~329.0) 228.5(71.5~588.8) Z=-4.215 <0.001 胰淀粉酶(U/L) 94(42~303) 201(56~523) Z=-3.893 <0.001 CO2CP(mmol/L) 23.31±4.00 20.68±4.96 t=7.080 <0.001 血糖(mmol/L) 6.83(5.24~9.87) 9.87(7.03~14.10) Z=-8.104 <0.001 PCT(ng/mL) 0.05(0.02~0.17) 1.31(0.36~4.19) Z=-16.238 <0.001 MCTSI评分 3.27±1.56 6.89±1.59 t=-29.770 <0.001
下载: 导出CSV
表 6 验证组患者的一般资料
Table 6. General information of patients in the validation group
临床资料 MAP组(n=408) SAP组(n=65) 统计值 P值 年龄(岁) 49.75±15.39 48.43±15.99 t=0.638 0.524 性别[例(%)] χ²=0.718 0.397 男 241(59.1) 42(64.6) 女 167(40.9) 23(35.4) 病因[例(%)] χ²=4.332 0.214 胆源性 160(39.2) 21(32.3) 脂源性 195(47.8) 38(58.5) 酒精性 12(2.9) 3(4.6) 其他 41(10.0) 3(4.6) 基础疾病[例(%)] χ²=8.281 0.082 高血压 56(10.5) 13(13.3) 糖尿病 68(12.7) 16(16.3) 脂肪肝 121(22.7) 16(16.3) 高脂血症 130(24.3) 33(33.7) 胆囊结石 159(29.8) 20(20.4) 入院方式[例(%)] χ²=191.003 <0.001 步行 359(88.0) 7(10.8) 非步行 49(12.0) 58(89.2) 住院天数(天) 10.0(7.0~14.0) 23.0(18.0~33.5) Z=-9.639 <0.001 是否入住ICU[例(%)] χ²=302.343 <0.001 是 2(0.5) 46(70.8) 否 404(99.5) 19(29.2) 死亡[例(%)] 0(0.0) 3(4.6) 0.019 合并症[例(%)] χ²=63.644 <0.001 ARDS 2(2.7) 41(31.5) MODS 0(0.0) 4(3.1) 浆膜腔积液 54(74.0) 38(29.2) 胰周感染 1(1.4) 5(3.8) 脓毒血症 0(0.0) 4(3.1) 急性肾损伤 0(0.0) 16(12.3) 急性肝损伤 3(4.1) 12(9.2) 胰腺假性囊肿 13(17.8) 10(7.2)
下载: 导出CSV
表 7 BISAP评分与改良BISAP评分预测SAP的ROC曲线分析
Table 7. ROC curves of BISAP score and modified BISAP score for predicting the severity of acute pancreatitis
项目 AUC SE 95%CI 敏感度(%) 特异度(%) 截断值 改良BISAP评分 0.972 0.010 0.952~0.985 92.31 92.16 >3 BISAP评分 0.887 0.017 0.855~0.914 78.46 85.54 >1
下载: 导出CSV
表 8 BISAP评分与改良BISAP评分预测AP死亡的ROC曲线分析
Table 8. ROC curves of BISAP score and modified BISAP score for predicting the mortality of acute pancreatitis
项目 AUC SE 95%CI 敏感度(%) 特异度(%) 改良BISAP评分 0.910 0.038 0.881~0.934 100.00 81.06 BISAP评分 0.896 0.039 0.865~0.922 100.00 77.23
下载: 导出CSV
-
[1] LANKISCH PG, APTE M, BANKS PA. Acute pancreatitis[J]. Lancet, 2015, 386( 9988): 85- 96. DOI: 10.1016/S0140-6736(14)60649-8. [2] Chinese Pancreatic Surgery Association, Chinese Society of Surgery, Chinese Medical Association. Guidelines for diagnosis and treatment of acute pancreatitis in China(2021)[J]. Chin J Dig Surg, 2021, 20( 7): 730- 739. DOI: 10.3760/cma.j.cn115610-20210622-00297.中华医学会外科学分会胰腺外科学组. 中国急性胰腺炎诊治指南(2021)[J]. 中华消化外科杂志, 2021, 20( 7): 730- 739. DOI: 10.3760/cma.j.cn115610-20210622-00297. [3] LUO XP, WANG J, WU Q, et al. Reasearch advances in acute pancreatitis scoring system[J]. J Clin Hepatol, 2022, 38( 9): 2188- 2192. DOI: 10.3969/j.issn.1001-5256.2022.09. 046.罗秀平, 王洁, 吴青, 等. 急性胰腺炎评分系统的研究进展[J]. 临床肝胆病杂志, 2022, 38( 9): 2188- 2192. DOI: 10.3969/j.issn.1001-5256.2022.09.046. [4] LI YF, XU F, XIAO JC, et al. The value of lactate dehydrogenase combined with BISAP scoring in predicting acutepancreatitis complicated with persistent organ damage[J]. Mod Med J, 2015, 43( 4): 459- 462. DOI: 10.3969/j.issn. 1671-7562. 2015.04.016.李玉芳, 徐峰, 肖接承, 等. 乳酸脱氢酶联合BISAP评分预测急性胰腺炎并发持续器官损害的价值[J]. 现代医学, 2015, 43( 4): 459- 462. DOI: 10.3969/j.issn.1671-7562.2015.04. 016. [5] BANKS PA, BOLLEN TL, DERVENIS C, et al. Classification of acute pancreatitis-2012: revision of the Atlanta classification and definitions by international consensus[J]. Gut, 2013, 62( 1): 102- 111. DOI: 10.1136/gutjnl-2012-302779. [6] WU BU, JOHANNES RS, SUN X, et al. The early prediction of mortality in acute pancreatitis: a large population-based study[J]. Gut, 2008, 57( 12): 1698- 1703. DOI: 10.1136/gut.2008.152702. [7] TRIKUDANATHAN G, WOLBRINK D, van SANTVOORT HC, et al. Current concepts in severe acute and necrotizing pancreatitis: an evidence-based approach[J]. Gastroenterology, 2019, 156( 7): 1994- 2007. e 3. DOI: 10.1053/j.gastro.2019.01.269. [8] VALVERDE-LÓPEZ F, MATAS-COBOS AM, ALEGRÍA-MOTTE C, et al. BISAP, RANSON, lactate and others biomarkers in prediction of severe acute pancreatitis in a European cohort[J]. J Gastroenterol Hepatol, 2017, 32( 9): 1649- 1656. DOI: 10.1111/jgh.13763. [9] HAGJER S, KUMAR N. Evaluation of the BISAP scoring system in prognostication of acute pancreatitis-A prospective observational study[J]. Int J Surg, 2018, 54(PtA): 76- 81. DOI: 10. 1016/j.ijsu.2018.04.026. [10] HARSHIT KUMAR A, SINGH GRIWAN M. A comparison of APACHE II,BISAP,Ranson’s score and modified CTSI in predicting the severity of acute pancreatitis based on the 2012 revised Atlanta Classification[J]. Gastroenterol Rep, 2018, 6( 2): 127- 131. DOI: 10.1093/gastro/ gox029. [11] MIKO A, VIGH É, MÁTRAI P, et al. Computed tomography severity index vs.other indices in the prediction of severity and mortality in acute pancreatitis:a predictive accuracy meta analysis[J]. Front Physiol, 2019, 10: 1002. DOI: 10.3389/fphys.2019.01002. [12] NING XX, PENG J. The value of modified CT severity index combined with BISAP score for acute pancreatitis[J]. J Clin Radiol, 2022, 41( 4): 659- 663. DOI: 10.13437/j.cnki. jcr.2022.04.035.宁晓详, 彭婕. 改良CT严重程度指数联合BISAP评分对早期急性胰腺炎预测价值[J]. 临床放射学杂志, 2022, 41( 4): 659- 663. DOI: 10.13437/j.cnki.jcr.2022.04.035. [13] LEE KJ, KIM HM, CHOI JS, et al. Comparison of predictive systems in severe acute pancreatitis according to the revised atlanta classification[J]. Pancreas, 2016, 45( 1): 46- 50. DOI: 10.1097/MPA.0000000000000433. [14] STIRLING AD, MORAN NR, KELLY ME, et al. The predictive value of C-reactive protein(CRP) in acute pancreatitisis interval change in CRP an additional indicator of severity?[J]. HPB(Oxford), 2017, 19( 10): 874- 880. DOI: 10.1016/j.hpb.2017.06.001. [15] KE L, TONG ZH, LI WQ, et al. Predictors of critical acute pancreatitis: a prospective cohort study[J]. Medicine(Baltimore), 2014, 93( 21): e108. DOI: 10.1097/MD.0000000000000108. [16] STERNBY H, HARTMAN H, JOHANSEN D, et al. IL-6 and CRP are superior in early differentiation between mild and nonmild acute pancreatitis[J]. Pancreatology, 2017, 17( 4): 550- 554. DOI: 10.1016/j.pan.2017.05.392. [17] STAUBLI SM, OERTLI D, NEBIKER CA. Laboratory markers predicting severity of acute pancreatitis[J]. Crit Rev Clin Lab Sci, 2015, 52( 6): 273- 283. DOI: 10.3109/10408363.2015.1051659. [18] LEPPÄNIEMI A, TOLONEN M, TARASCONI A, et al. 2019 WSES guidelines for the management of severe acute pancreatitis[J]. World J Emerg Surg, 2019, 14: 27. DOI: 10.1186/s13017-019-0247-0. [19] van den BERG FF, de BRUIJN AC, van SANTVOORT HC, et al. Early laboratory biomarkers for severity in acute pancreatitis;A systematic review and meta-analysis[J]. Pancreatology, 2020, 20( 7): 1302- 1311. DOI: 10.1016/j.pan.2020.09.007. [20] MATOWICKA-KARNA J. Markers of inflammation, activation of blood platelets and coagulation disorders in inflammatory bowel diseases[J]. Postepy Hig Med Dosw(Online), 2016, 70: 305- 312. DOI: 10.5604/17322693.1199305. [21] LELUBRE C, ANSELIN S, ZOUAOUI BOUDJELTIA K, et al. Interpretation of C-reactive protein concentrations in critically ill patients[J]. Biomed Res Int, 2013, 2013: 124021. DOI: 10.1155/2013/124021. [22] KONG W, HE Y, BAO H, et al. Diagnostic value of neutrophil-lymphocyte ratio for predicting the severity of acute pancreatitis: a meta-analysis[J]. Dis Markers, 2020, 2020: 9731854. DOI: 10.1155/2020/9731854. [23] UEDA T, TAKEYAMA Y, YASUDA T, et al. Immunosuppression in patients with severe acute pancreatitis[J]. J Gastroenterol, 2006, 41( 8): 779- 784. DOI: 10.1007/s00535-006-1852-8. [24] HUANG L, CHEN C, YANG L, et al. Neutrophil-to-lymphocyte ratio can specifically predict the severity of hypertriglyceridemia-induced acute pancreatitis compared with white blood cell[J]. J Clin Lab Anal, 2019, 33( 4): e22839. DOI: 10.1002/jcla.22839. [25] ZHOU TY, PAN T, LIU JL, et al. Value of the neutrophil-lymphocyte ratio for predicting the severity of acute pancreatitis based on the Revised Atlanta Classification[J]. J Shanghai Jiaotong Univ(Med Sci), 2016, 36( 7): 1023- 1028. DOI: 10.3969/j.issn.1674-8115.2016.07.013.周天昀, 潘婷, 刘嘉琳, 等. 中性粒细胞与淋巴细胞比值在亚特兰大新分类标准下预测急性胰腺炎严重程度的价值[J]. 上海交通大学学报(医学版), 2016, 36( 7): 1023- 1028. DOI: 10.3969/j.issn.1674-8115.2016.07.013. [26] GEZER NS, BENGI G, BARAN A, et al. Comparison of radiological scoring systems, clinical scores, neutrophil-lymphocyte ratio and serum C-reactive protein level for severity and mortality in acute pancreatitis[J]. Rev Assoc Med Bras(1992), 2020, 66( 6): 762- 770. DOI: 10.1590/1806-9282.66.6.762. [27] WANG Y, LI MZ, LIU YF, et al. Early predictors for acute kidney injury in acute pancreatitis[J]. J Clin Hepatol, 2022, 38( 5): 1192- 1197. DOI: 10.3969/j.issn.1001-5256.2022. 05.046.王岩, 李明政, 刘玉凤, 等. 急性胰腺炎发生急性肾损伤的早期预测指标[J]. 临床肝胆病杂志, 2022, 38( 5): 1192- 1197. DOI: 10.3969/j.issn.1001-5256.2022. 05.046. [28] LI Y, ZHAO YJ, YU HY, et al. Predictive value of soluble urokinase-type plasminogen activator receptor in patients with severe acute pancreatitis[J]. J Army Med Univ, 2022, 44( 3): 241- 245. DOI: 10.16016/j.2097-0927.202107019.李杨, 赵胤杰, 余海燕, 等. 血浆可溶性尿激酶型纤溶酶原激活物受体对重症急性胰腺炎的预测价值[J]. 陆军军医大学学报, 2022, 44( 3): 241- 245. DOI: 10.16016/j. 2097-0927. 202107019. [29] LI Q, LIU CN, LING LQ, et al. Association between coagulation function and prognosis in patients with acute pancreatitis[J]. J South Med Univ, 2022, 42( 7): 1006- 1012. DOI: 10.12122/j.issn.1673-4254.2022.07.06.李勤, 刘超男, 凌莉琴, 等. 凝血相关的实验室指标对急性胰腺炎患者的病情和预后有较高预测价值[J]. 南方医科大学学报, 2022, 42( 7): 1006- 1012. DOI: 10.12122/j.issn. 1673-4254.2022.07.06. [30] ZHANG GQ, WANG G, LI L, et al. Plasma D-Dimer level is an early predictorof severity of acute pancreatitis based on 2012 atlanta classification[J]. Med Sci Monit, 2019, 25: 9019- 9027. DOI: 10.12659/MSM.918311. [31] WAN J, YANG X, HE W, et al. Serum D-dimer levels at admission for prediction of outcomes in acute pancreatitis[J]. BMC Gastroenterol, 2019, 19( 1): 67. DOI: 10.1186/s12876-019-0989-x. [32] JI L, LV JC, SONG ZF, et al. Risk factors of infected pancreatic necrosis secondary to severe acute pancreatitis[J]. Hepatobiliary Pancreat Dis Int, 2016, 15( 4): 428- 433. DOI: 10.1016/s1499-3872(15)60043-1. -

 本文二维码
本文二维码
计量
- 文章访问数: 240
- HTML全文浏览量: 57
- PDF下载量: 40
- 被引次数: 0

