
 PDF下载 ( 937 KB)
PDF下载 ( 937 KB)

HBV感染家庭聚集性传播的影响因素及远期结局情况分析
DOI: 10.3969/j.issn.1001-5256.2023.09.009
Familial aggregation transmission of hepatitis B virus infection and influencing factors for outcome
-
摘要:
目的 分析云南省HBV感染的家庭聚集性、传播危险因素及结局情况,为控制HBV家庭聚集性传播提供策略。 方法 选取2015年1月—2017年12月在昆明市第三人民医院确诊的HBsAg阳性患者,调查其家庭的人口学特征、实验室指标等。对HBsAg阳性者的家庭进行二项分布拟合优度χ2检验并计算家庭聚集率。以单因素和多因素Logistic回归模型分析HBV传播及新发肝硬化或肝癌的影响因素。使用Kaplan-Meier法分析HBsAg阳性者肝硬化或肝癌的累积发生率,并采用Log-rank检验进行比较。 结果 共调查459户HBsAg阳性家庭,包括618例HBsAg阳性者和918例HBsAg阴性者,其中有107户≥2名家庭成员HBsAg阳性,家庭聚集率为23.31%(χ2=95.393,P<0.001)。传播方式以母婴传播为主。多因素Logistic回归分析结果显示,性别(OR=0.397,95%CI:0.270~0.584,P<0.001)、民族(OR=1.655,95%CI:1.035~2.648,P=0.036)、月收入(OR=1.612,95%CI:1.094~2.375,P=0.016)、共用洁具(OR=2.789,95%CI:1.530~5.086,P<0.001)、基线肝硬化(OR=2.702,95%CI:1.404~5.203,P=0.003)、总胆固醇(OR=0.772,95%CI:0.657~0.908,P=0.002)和HBV DNA(OR=2.063,95%CI:1.753~2.428,P<0.001)是HBV家庭聚集性传播的独立影响因素。618例HBsAg阳性者平均随访4.80年,累积新发肝硬化或肝癌85例(13.75%);Kaplan-Meier法分析结果显示,HBV传播聚集性家庭的肝硬化或肝癌的累积发生率高于非聚集性家庭(χ2=10.629,P<0.001)。以是否抗病毒治疗、是否为HBV聚集性传播家庭对618例HBsAg阳性患者进行分层分析,结果显示HBV传播聚集性家庭且未抗病毒治疗者的肝硬化或肝癌的累积发生率最高(32.50%),非HBV传播聚集性家庭且抗病毒治疗者的肝硬化或肝癌的累积发生率最低(3.33%)。 结论 HBsAg阳性者具有家庭聚集性,应加强其家庭成员的筛查、健康宣传教育和追踪观察。抗病毒治疗能有效降低聚集家庭内肝硬化和肝癌的发生率。 Abstract:Objective To investigate the condition of hepatitis B virus (HBV) infection in Yunnan, China, in terms of familial aggregation, risk factors for transmission, and outcome, and to provide strategies for controlling the familial aggregation transmission of HBV. Methods The HBsAg-positive patients who were diagnosed in The Third People’s Hospital of Kunming from January 2015 to December 2017 were enrolled, and related data were analyzed, including demographic features and laboratory markers. The chi-square goodness-of-fit test for binomial distribution was performed for the families of the HBsAg-positive patients, and the familial aggregation rate was calculated. The univariate and multivariate Logistic regression models were used to analyze the risk factors for HBV transmission and new-onset liver cirrhosis or liver cancer. The Kaplan-Meier method was used to investigate the cumulative incidence rate of new-onset liver cirrhosis or liver cancer in HBsAg-positive patients, and the log-rank test was used for comparison. Results A total of 459 HBsAg-positive families were analyzed, involving 618 HBsAg-positive individuals and 918 HBsAg-negative individuals, and among these families, 107 had ≥2 HBsAg-positive family members, with a familial aggregation rate of 23.31% (χ2=95.393, P<0.001). The mode of transmission was mainly mother-to-child transmission. The multivariate Logistic regression analysis showed that sex (odds ratio [OR]=0.397, 95% confidence interval [CI]: 0.270-0.584, P<0.001), nationality (OR=1.655, 95%CI: 1.035-2.648, P=0.036), monthly income (OR=1.612, 95%CI: 1.094-2.375, P=0.016), shared sanitary appliance (OR=2.789, 95%CI: 1.530-5.086, P<0.001), liver cirrhosis at baseline (OR=2.702, 95%CI: 1.404-5.203, P=0.003), total cholesterol (OR=0.772, 95%CI: 0.657-0.908, P=0.002), and HBV DNA (OR=2.063, 95%CI: 1.753-2.428, P<0.001) were independent influencing factors for the familial aggregation transmission of HBV. The 618 HBsAg-positive patients were followed up for a mean time of 4.80 years, with 85 cases (13.75%) of new-onset liver cirrhosis or liver cancer, and the Kaplan-Meier analysis showed that the families with familial aggregation transmission of HBV had a significantly higher cumulative incidence rate of liver cirrhosis or liver cancer than those without familial aggregation transmission (χ2=10.629, P<0.001). A stratified analysis was performed for the 618 HBsAg-positive patients based on the presence or absence of antiviral therapy and familial aggregation transmission of HBV, and the results showed that the patients who came from the family with familial aggregation transmission of HBV and did not receive antiviral therapy had the highest cumulative incidence rate of liver cirrhosis or liver cancer (32.50%), while those who came from the family without familial aggregation transmission of HBV and received antiviral therapy had the lowest incidence rate of liver cirrhosis or liver cancer (3.33%). Conclusion Familial aggregation is observed in HBsAg-positive individuals, and screening, health education, and follow-up observation should be strengthened for their family members. Antiviral therapy can effectively reduce the incidence rates of liver cirrhosis and liver cancer in families with aggregation transmission. -
Key words:
- Hepatitis B Virus /
- Disease Transmission, Infectious /
- Root Cause Analysis
-

图 1 单项指标预测HBV家庭聚集传播的ROC曲线
Figure 1. ROC curve for predicting HBV family agglomeration transmission by single indicator
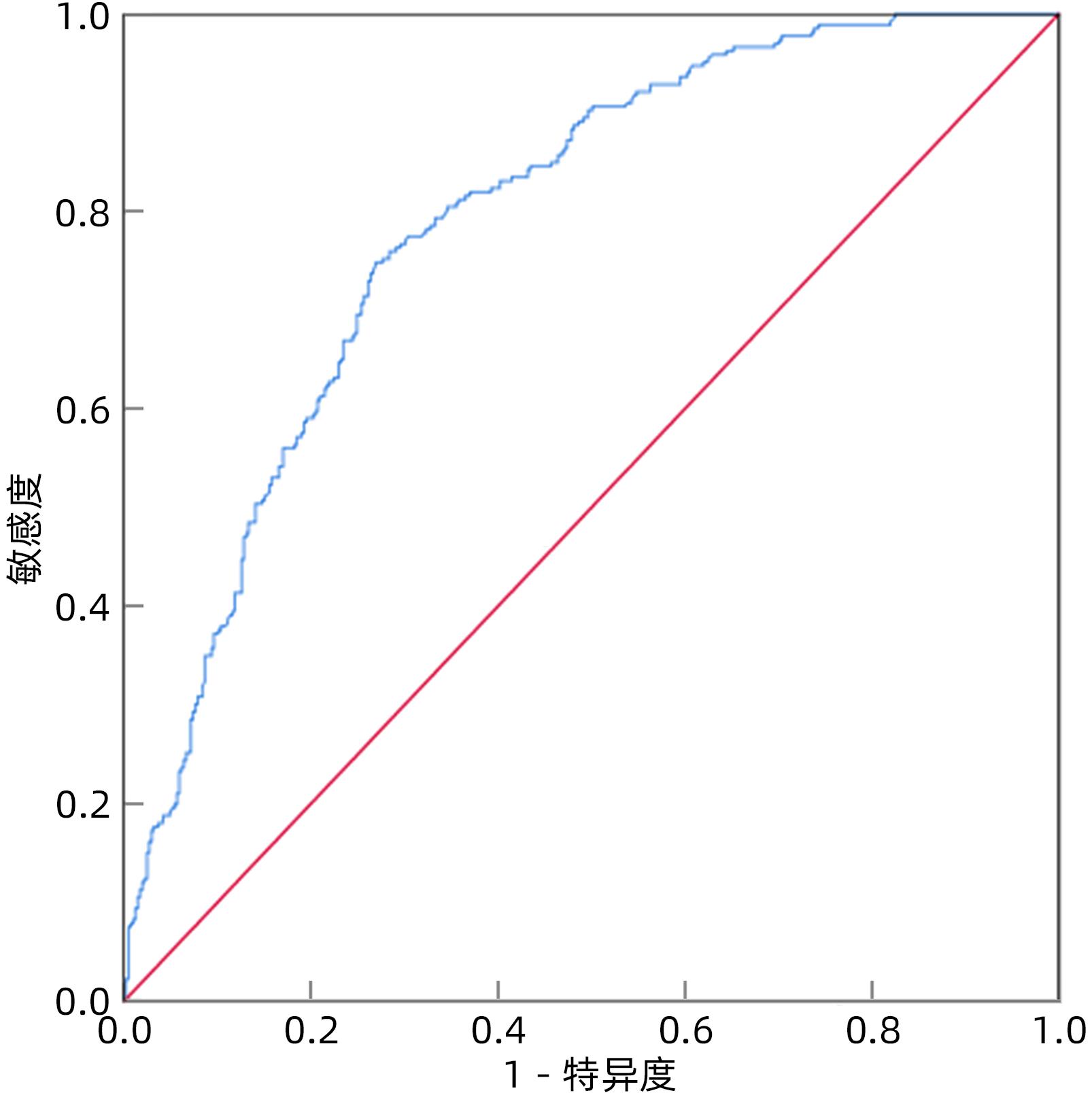
图 2 7项指标联合预测HBV家庭聚集传播的ROC曲线
Figure 2. ROC curve for predicting HBV family aggregation transmission using a combination of seven indicators
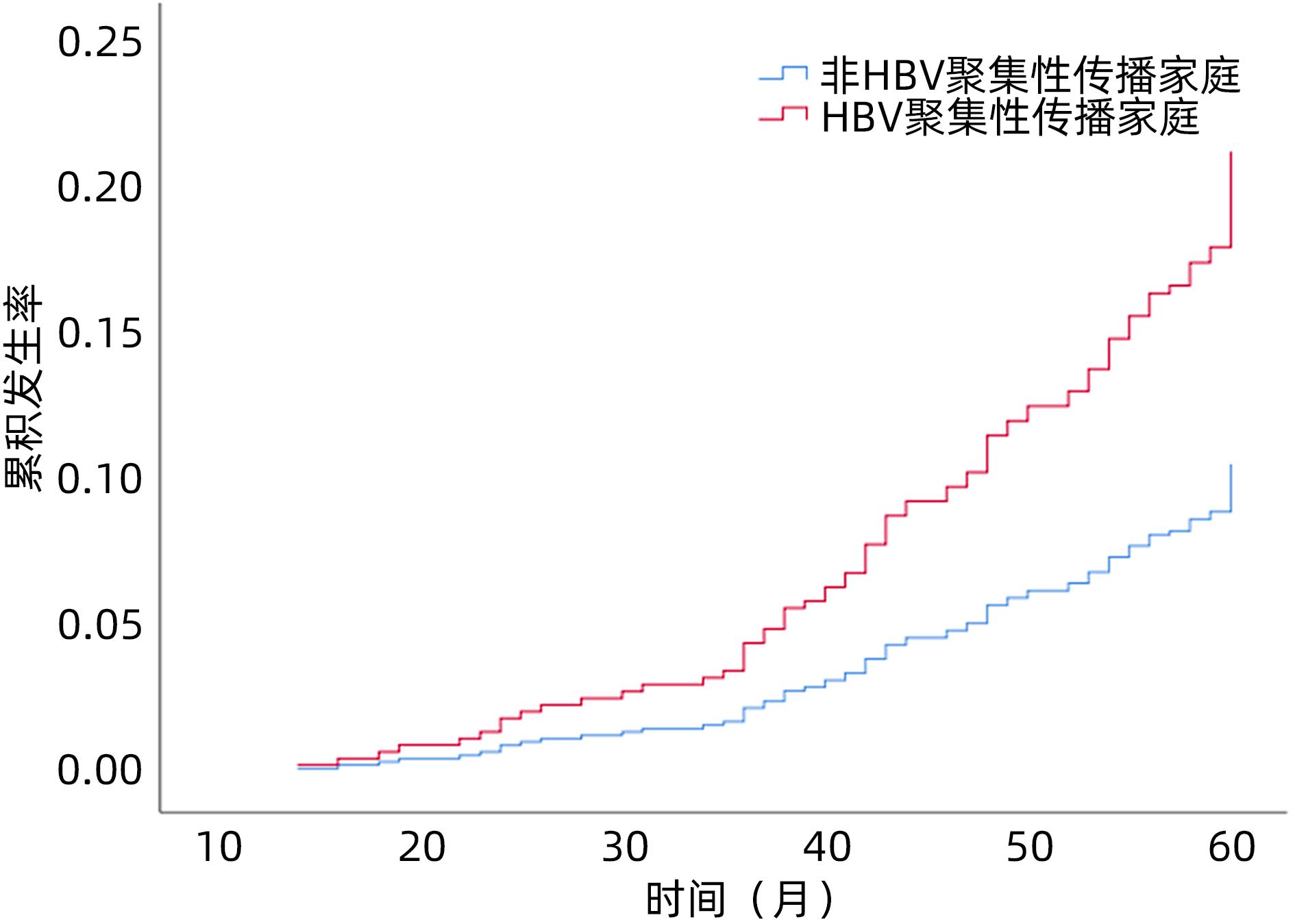
图 3 HBV家庭聚集与非家庭聚集患者的肝硬化或肝癌累积发生率
Figure 3. Accumulative incidence of liver cirrhosis or liver cancer in HBV family aggregation and non family aggregation
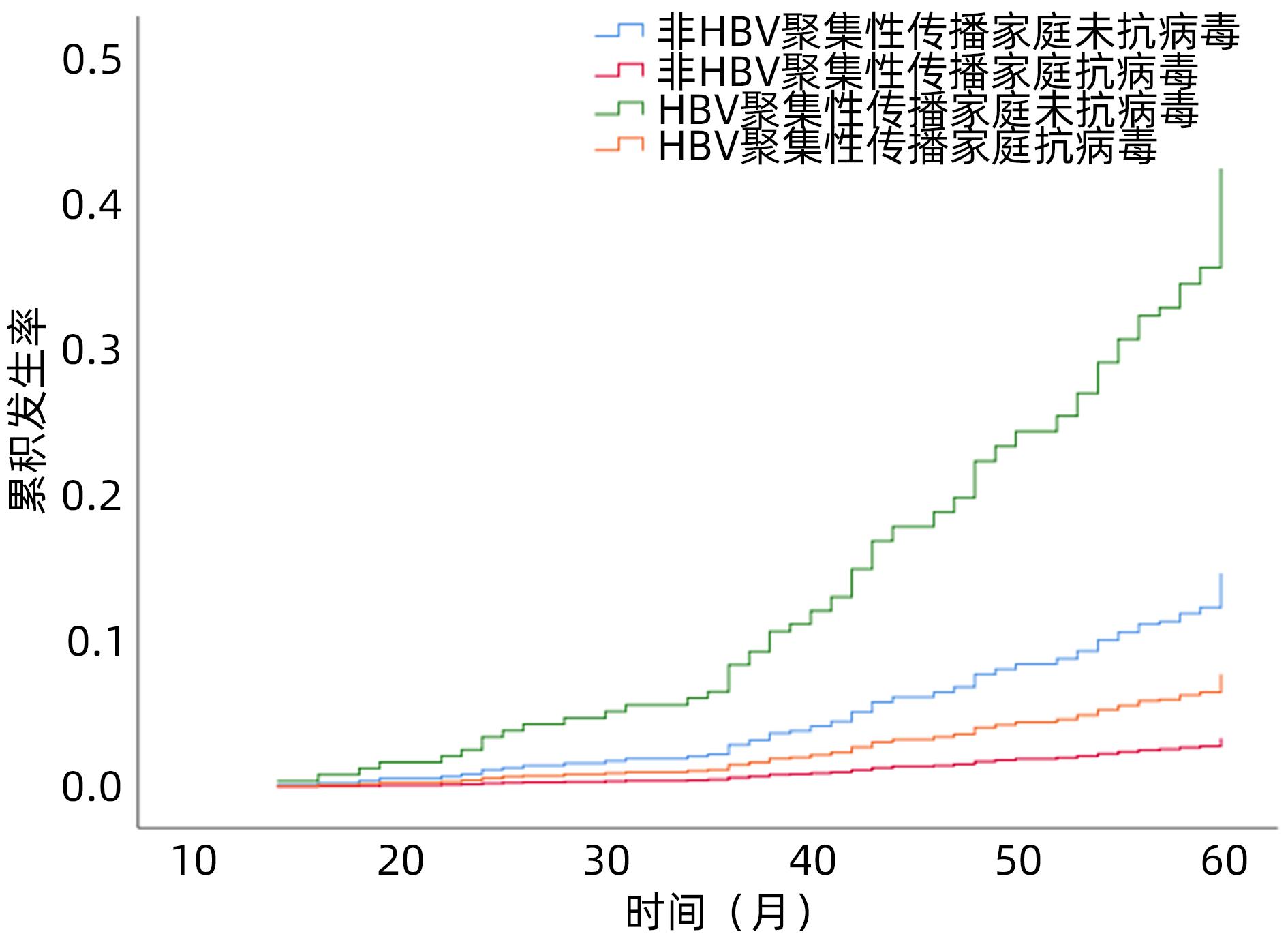
图 4 HBV家庭聚集与非家庭聚集中抗病毒和未抗病毒患者的肝硬化或肝癌累积发生率
Figure 4. Cumulative incidence of liver cirrhosis or liver cancer with antiviral and non antiviral in HBV family aggregation and non family aggregation
表 1 HBsAg阳性者例数和家庭成员数的分布情况
Table 1. Distribution of HBsAg positive cases and family members
HBsAg阳性例数 家庭成员数 2名 3名 4名 5名 6名 7名 8名 9名 合计 1 147 106 45 32 11 8 2 1 352 2 25 13 11 8 6 2 1 2 68 3 10 7 5 2 3 1 0 28 4 3 2 1 1 2 0 9 5 1 0 0 1 0 2  下载: 导出CSV
下载: 导出CSV
表 2 所有调查对象的人口学特征
Table 2. Demographic characteristics of all respondents
项目 HBsAg阴性 (n=918) HBsAg阳性 (n=618) 男/女(例) 462/456 324/294 年龄(例) <18岁 71 58 18~<35岁 282 202 35~<60岁 465 287 ≥60岁 100 71 民族(例) 汉族 663 498 彝族 75 39 白族 58 31 哈尼族 36 18 傣族 32 13 其他 54 19 职业(例) 儿童和学生 107 74 农民和工人 606 390 其他 205 154 文化程度(例) 高中及以下 615 483 高中以上 303 135
下载: 导出CSV
表 3 HBsAg阳性病例的家庭聚集单因素分析
Table 3. Single factor analysis of family aggregation of HBsAg positive cases
项目 家庭聚集性传播 (n=266) 无家庭聚集性传播 (n=352) P值 OR 95%CI 男/女(例) 103/163 221/131 <0.001 0.375 0.270~0.520 年龄(例) <18岁 30 28 1 18~<35岁 91 111 0.041 2.098 1.029~4.277 35~<60岁 121 166 0.100 1.605 0.913~2.823 ≥60岁 24 47 0.200 1.427 0.828~2.461 婚姻状况(未婚/已婚,例) 93/173 119/233 0.764 0.950 0.680~1.328 汉族/少数民族(例) 196/70 300/52 <0.001 2.060 1.379~3.078 职业(例) 儿童和学生 48 26 1 农民和工人 194 232 <0.001 10.001 5.241~19.080 其他 24 147 <0.001 5.361 3.322~8.652 文化程度(高中及以下/高中以上,例) 206/60 277/75 0.710 1.076 0.732~1.580 家庭月收入(<3 000元/≥3 000元,例) 154/112 224/128 0.042 1.406 1.013~1.953 饮酒(否/是,例) 170/96 238/114 0.336 1.179 0.843~1.649 糖尿病(无/有,例) 238/28 317/35 0.813 1.066 0.631~1.801 高血压(无/有,例) 232/34 299/53 0.421 0.827 0.520~1.314 共用洁具(否/是,例) 219/47 326/26 <0.001 2.691 1.618~4.475 肝硬化(无/有,例) 231/35 327/25 0.013 1.982 1.155~3.401 BMI(kg/m2) 22.59 ± 1.81 22.56 ± 1.87 0.851 1.008 0.925~1.100 WBC(×109/L) 4.98 ± 1.65 5.12 ± 1.47 0.266 0.943 0.851~1.046 Hb(g/L) 119.97 ± 32.45 118.31 ± 35.75 0.554 1.001 0.997~1.006 PLT(×109/L) 130(84~189) 137(92~198) 0.318 0.999 0.997~1.001 TBil(μmol/L) 40.2(28.3~58.9) 42.0(24.6~63.2) 0.839 0.999 0.993~1.005 ALT(U/L) 93(43~166) 108(52~182) 0.147 0.999 0.997~1.000 AST(U/L) 79(41~119) 82(40~127) 0.184 0.998 0.995~1.001 Alb(g/L) 35.58 ± 6.55 36.48 ± 6.48 0.087 0.979 0.955~1.003 球蛋白(g/L) 29.64 ± 4.69 30.06 ± 4.21 0.239 0.979 0.944~1.015 GGT(U/L) 37(24~51) 38(24~54) 0.441 0.997 0.988~1.005 ALP(U/L) 76(58~97) 77(59~92) 0.292 1.003 0.997~1.009 GLU(mmol/L) 4.99 ± 0.59 4.95 ± 0.59 0.336 1.141 0.872~1.494 TC(mmol/L) 3.67 ± 1.28 3.98 ± 1.11 <0.001 0.801 0.699~0.918 TG(mmol/L) 0.93(0.58~1.41) 1.01(0.60~1.53) 0.199 0.845 0.653~1.093 BUN(mmol/L) 4.81 ± 1.81 4.68 ± 1.72 0.382 1.041 0.951~1.140 Cr(μmol/L) 65.04 ± 21.59 66.60 ± 20.15 0.353 0.996 0.989~1.004 UA(μmol/L) 355(293~421) 352(285~411) 0.372 1.001 0.999~1.002 PT(s) 13.35 ± 3.07 13.38 ± 2.76 0.892 0.996 0.943~1.053 INR 1.17 ± 0.32 1.14 ± 0.31 0.194 1.401 0.840~2.329 HBV DNA(lg IU/mL) 5.07 ± 1.34 5.03 ± 1.36 <0.001 2.125 1.821~2.481 注:GLU,血糖;TC,总胆固醇;TG,甘油三酯;BUN,尿素氮;Cr,血肌酐;UA,尿酸;PT,凝血酶原时间;INR,国际标准化比值。
下载: 导出CSV
表 4 HBsAg阳性病例的家庭聚集多因素分析
Table 4. Multi-factor analysis of family aggregation of HBsAg positive cases
项目 B值 SE Wald P值 OR 95%CI 性别 -0.923 0.197 21.998 <0.001 0.397 0.270~0.584 共用洁具 1.026 0.307 11.199 <0.001 2.789 1.530~5.086 月收入 0.478 0.198 5.832 0.016 1.612 1.094~2.375 民族 0.504 0.240 4.418 0.036 1.655 1.035~2.648 基线肝硬化 0.994 0.334 8.846 0.003 2.702 1.404~5.203 TC -0.580 0.082 9.854 0.002 0.772 0.657~0.908 HBV DNA 0.724 0.083 75.997 <0.001 2.063 1.753~2.428
下载: 导出CSV
表 5 新发肝硬化或肝癌的单因素和多因素Logistic回归分析
Table 5. Single factor and multiple factor Logistic regression analysis of new liver cirrhosis or liver cancer
项目 单因素分析 多因素分析 OR 95%CI P值 OR 95%CI P值 职业 0.579 0.391~0.856 0.006 家庭聚集 2.097 1.317~3.339 0.002 1.996 1.096~3.635 0.024 抗病毒治疗 0.241 0.134~0.431 <0.001 0.182 0.092~0.359 <0.001 WBC(×109/L) 0.660 0.565~0.771 <0.001 PLT(×109/L) 0.989 0.985~0.992 <0.001 TBil(μmol/L) 0.991 0.982~1.000 0.042 ALT(U/L) 0.991 0.988~0.995 <0.001 0.995 0.990~0.999 0.019 Alb(g/L) 0.918 0.884~0.953 <0.001 ALP(U/L) 1.016 1.008~1.025 <0.001 TC(mmol/L) 0.410 0.325~0.517 <0.001 0.561 0.427~0.738 <0.001 TG(mmol/L) 0.308 0.193~0.490 <0.001 BUN(mmol/L) 1.147 1.008~1.304 0.038 UA(μmol/L) 1.003 1.001~1.006 0.005 INR 4.170 1.988~8.745 <0.001
下载: 导出CSV
-
[1] TAN M, BHADORIA AS, CUI F, et al. Estimating the proportion of people with chronic hepatitis B virus infection eligible for hepatitis B antiviral treatment worldwide: a systematic review and meta-analysis[J]. Lancet Gastroenterol Hepatol, 2021, 6( 2): 106- 119. DOI: 10.1016/S2468-1253(20)30307-1. [2] Chinese Society of Infectious Diseases, Chinese Medical Association; Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B(version 2019)[J]. J Clin Hepatol, 2019, 35( 12): 2648- 2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.中华医学会感染病学分会, 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35( 12): 2648- 2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007. [3] YANG Y, JIN L, WANG J, et al. Study of molecular epidemiology in families with clusters of hepatitis B virus infection and unfavorable outcome[J]. Chin J Infect Dis, 2016, 34( 9): 540- 544. DOI: 10.3760/cma.j.issn.1000-6680.2016.09.006.杨瑗, 金李, 王静, 等. 不良结局家族聚集性乙型肝炎病毒感染家系的分子流行病学[J]. 中华传染病杂志, 2016, 34( 9): 540- 544. DOI: 10.3760/cma.j.issn.1000-6680.2016.09.006. [4] ZHANG RL, WANG MY, CHEN QY, et al. Study on the risk factors related vertical transmission of HBV positive couples to their infant[J]. Chin J Epidemiol, 2012, 33( 12): 1283- 1287. DOI: 10.3760/cma.j.issn.0254-6450.2012.12.020.张荣莲, 王梅颖, 陈起燕, 等. 父母双方乙型肝炎病毒感染垂直传播的危险因素研究[J]. 中华流行病学杂志, 2012, 33( 12): 1283- 1287. DOI: 10.3760/cma.j.issn.0254-6450.2012.12.020. [5] HUANG Y, WANG W, ZHANG CH, et al. Hepatitis B infection and hepatitis B knowledge and behavior among families with hepatitis B surface antigen positive individuals in Guangzhou[J]. Chin J Vacc Immu, 2021, 27( 2): 187- 190. DOI: 10.19914/j.CJVI.2021027.黄勇, 王雯, 张春焕, 等. 广州市乙型肝炎表面抗原阳性家庭乙型肝炎感染和乙型肝炎相关知识与行为调查[J]. 中国疫苗和免疫, 2021, 27( 2): 187- 190. DOI: 10.19914/j.CJVI.2021027. [6] Chinese Society of Hepatology and Chinese Society of Infectious Diseases, Chinese Medical Association. The guideline of prevention and treatment for chronic hepatitis B: a 2015 update[J]. J Clin Hepatol, 2015, 31( 12): 1941- 1960. DOI: 10.3969/j.issn.1001-5256.2015.12.002.中华医学会肝病学分会, 中华医学会感染病学分会. 慢性乙型肝炎防治指南(2015年更新版)[J]. 临床肝胆病杂志, 2015, 31( 12): 1941- 1960. DOI: 10.3969/j.issn.1001-5256.2015.12.002. [7] MIN DY, HUANG WY, YANG JY, et al. Familial aggregation of hepatitis B virus infection and its influence factors in minority areas of Guizhou province[J]. China Public Health, 2016, 32( 2): 183- 187. DOI: 10.11847/zgggws2016-32-02-15.闵定玉, 黄文湧, 杨敬源, 等. 贵州少数民族人群HBV感染家庭聚集性及影响因素分析[J]. 中国公共卫生, 2016, 32( 2): 183- 187. DOI: 10.11847/zgggws2016-32-02-15. [8] Chinese Society of Hepatology, Chinese Medical Association. Chinese guidelines on the management of liver cirrhosis[J]. J Clin Hepatol, 2019, 35( 11): 2408- 2425. DOI: 10.3969/j.issn.1001-5256.2019.11.006.中华医学会肝病学分会. 肝硬化诊治指南[J]. 临床肝胆病杂志, 2019, 35( 11): 2408- 2425. DOI: 10.3969/j.issn.1001-5256.2019.11.006. [9] General Office of National Health Commission. Standard for diagnosis and treatment of primary liver cancer(2022 edition)[J]. J Clin Hepatol, 2022, 38( 2): 288- 303. DOI: 10.3969/j.issn.1001-5256.2022.02.009.国家卫生健康委办公厅. 原发性肝癌诊疗指南(2022年版)[J]. 临床肝胆病杂志, 2022, 38( 2): 288- 303. DOI: 10.3969/j.issn.1001-5256.2022.02.009. [10] PANG XH, WANG H, MA JX, et al. Study on family aggregation and risk factors of hepatitis B virus transmission in Chaoyang district, Beijing[J]. Chin J Prevent Med, 2012, 46( 9): 818- 821. DOI: 10.3760/cma.j.issn.0253-9624.2012.09.009.庞星火, 王怀, 马建新, 等. 北京市朝阳区乙型肝炎病毒感染家庭聚集性及传播危险因素研究[J]. 中华预防医学杂志, 2012, 46( 9): 818- 821. DOI: 10.3760/cma.j.issn.0253-9624.2012.09.009. [11] BU SH, HUANG WY, WANG JH, et al. Study on association of family structures with family aggregation of hepatitis B virus infection in 1115 households in Guizhou province[J]. J Guizhou Med Univ, 2019, 44( 6): 658- 663. DOI: 10.19367/j.cnki.1000-2707.2019.06.008.卜苏洪, 黄文湧, 汪俊华, 等. 贵州省1115户居民家庭结构和乙肝感染家庭聚集性关系研究[J]. 贵州医科大学学报, 2019, 44( 6): 658- 663. DOI: 10.19367/j.cnki.1000-2707.2019.06.008. [12] XIE ZY, FEI Y, YANG T, et al. Epidemiological investigation of hepatitis B virus infection and analysis of virus mutations in hepatitis B surface antigen positive students and their first-degree relatives[J]. Acad J Second Military Med Univ, 2019, 40( 1): 54- 60. DOI: 10.16781/j.0258-879x.2019.01.0054.谢震宇, 费怡, 杨天, 等. 乙型肝炎表面抗原阳性学生及其一级亲属乙型肝炎病毒感染流行病学调查与病毒变异分析[J]. 第二军医大学学报, 2019, 40( 1): 54- 60. DOI: 10.16781/j.0258-879x.2019.01.0054. [13] BU SH, HUANG WY, WANG JH, et al. Risk factors of family aggregation with hepatitis B virus infection in minority areas of Guizhou province using multilevel statistical model[J]. J Guizhou Med Univ, 2019, 44( 4): 447- 452. DOI: 10.19367/j.cnki.1000-2707.2019.04.014.卜苏洪, 黄文湧, 汪俊华, 等. 贵州省两个少数民族地区乙肝感染家庭聚集性影响因素分析[J]. 贵州医科大学学报, 2019, 44( 4): 447- 452. DOI: 10.19367/j.cnki.1000-2707.2019.04.014. [14] KONG Y, DING ZR, LUO M, et al. Investigation on risk factors of the hepatitis B virus infection by logitstic regression in Yunnan province[J]. Chin J Vacc Immu, 2012, 18( 2): 123- 126, 152.孔毅, 丁峥嵘, 罗梅, 等. 云南省乙型肝炎病毒感染危险因素Logistic回归模型分析[J]. 中国疫苗和免疫, 2012, 18( 2): 123- 126, 152. [15] WU X, XU TT, SHEN LD, et al. Cancer-related risk factors in remote and minority areas of Yunnan province[J]. J Kunming Med Univ, 2019, 40( 10): 77- 80.吴夕, 徐婷婷, 沈丽达, 等. 云南省贫困、偏远、少数民族聚集地区癌症相关危险因素现状调查[J]. 昆明医科大学学报, 2019, 40( 10): 77- 80. [16] LU W, ZHOU Y, XIE JX, et al. Epidemic survey of family clustering risk factors for hepatitis B in Shanghai area[J]. Acad J Second Military Med Univ, 2009, 30( 10): 1162- 1165. DOI: 10.3724/SP.J.1008.2009.01162.陆伟, 周赟, 谢佳新, 等. 上海地区乙型肝炎家庭聚集性危险因素的流行病学调查[J]. 第二军医大学学报, 2009, 30( 10): 1162- 1165. DOI: 10.3724/SP.J.1008.2009.01162. [17] LI YW, DOU XG. Focus on the special population with hepatitis B virus infection: Early diagnosis, early treatment, and early benefits[J]. J Clin Hepatol, 2022, 38( 11): 2441- 2443. DOI: 10.3969/j.issn.1001-5256.2022.11.001.李艳伟, 窦晓光. 关注HBV感染特殊人群: 早诊、早治、早获益[J]. 临床肝胆病杂志, 2022, 38( 11): 2441- 2443. DOI: 10.3969/j.issn.1001-5256.2022.11.001. [18] ZHOU HK, JIANG JN, SU MH, et al. Efficacy of entecavir versus tenofovir disoproxil fumarate in treatment of chronic hepatitis B patients with high viral load[J]. J Clin Hepatol, 2022, 38( 3): 532- 536. DOI: 10.3969/j.issn.1001-5256.2022.03.008.周珲堃, 江建宁, 苏明华, 等. 恩替卡韦与替诺福韦酯治疗高病毒载量慢性乙型肝炎患者的效果分析[J]. 临床肝胆病杂志, 2022, 38( 3): 532- 536. DOI: 10.3969/j.issn.1001-5256.2022.03.008. -

 本文二维码
本文二维码
计量
- 文章访问数: 265
- HTML全文浏览量: 136
- PDF下载量: 64
- 被引次数: 0

