
 PDF下载 ( 2115 KB)
PDF下载 ( 2115 KB)

微波消融联合全身化疗治疗复发性肝内胆管癌的有效性与安全性分析
DOI: 10.3969/j.issn.1001-5256.2023.07.015
Efficacy and safety of microwave ablation combined with systemic chemotherapy in treatment of recurrent intrahepatic cholangiocarcinoma
-
摘要:
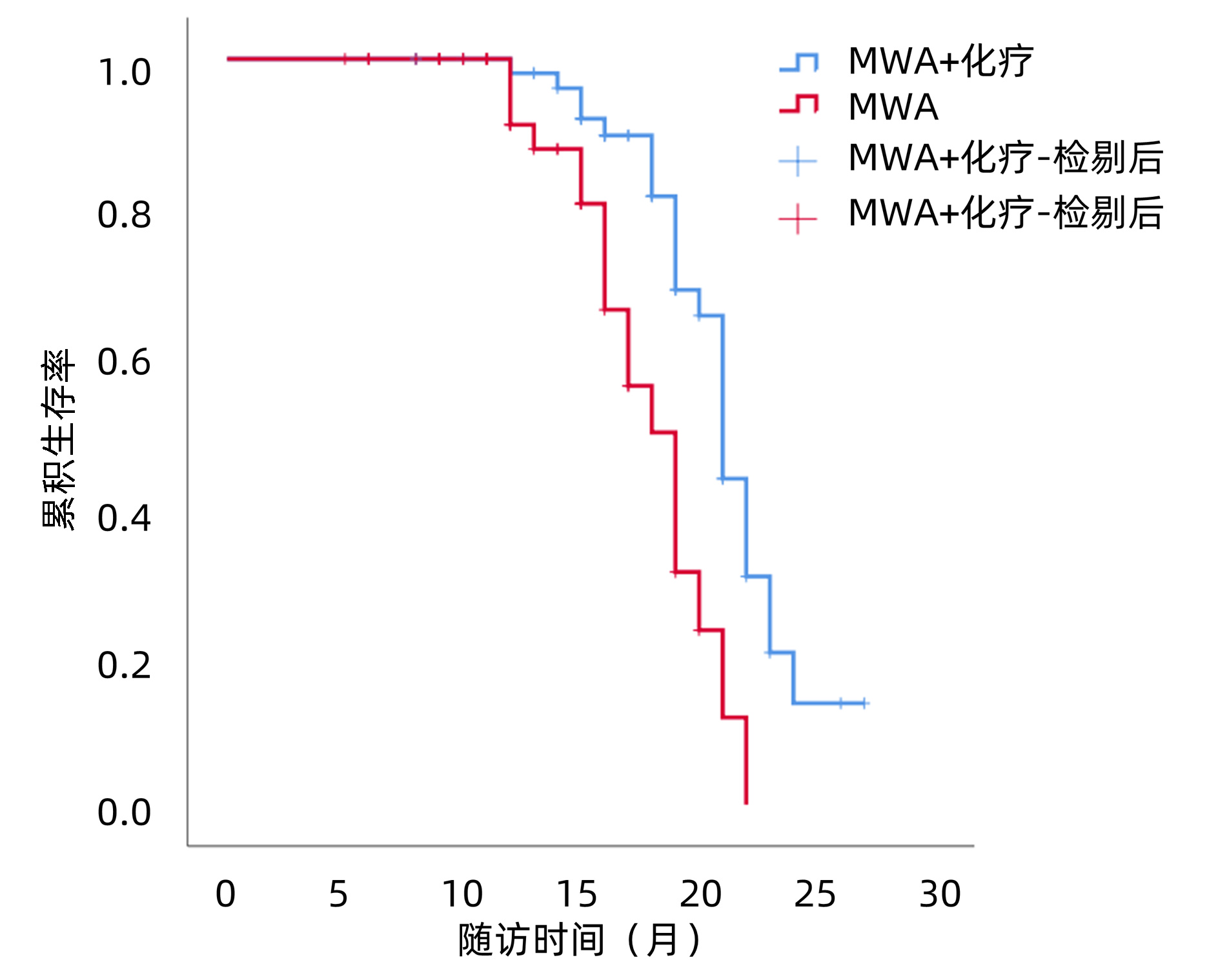
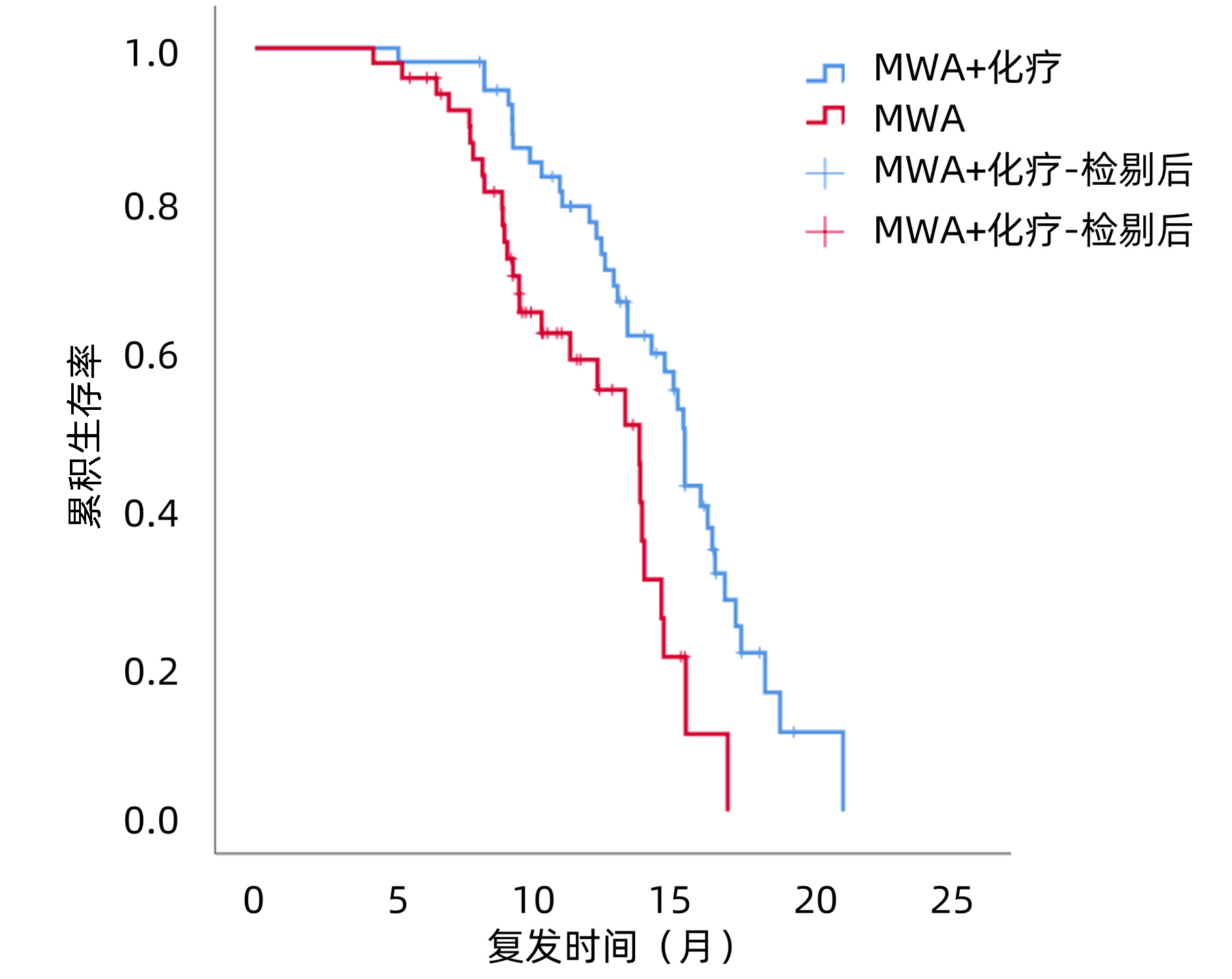
目的 探讨微波消融(MWA)联合化疗与单独MWA治疗复发性肝内胆管癌(RICC)的有效性和安全性。 方法 采用回顾性队列研究方法。选取2014年1月—2021年3月内江市第二人民医院及西南医科大学附属医院接受MWA+ 化疗和单独MWA的RICC患者,收集入组患者的临床病理资料。计量资料两组间比较采用成组t检验,计数资料两组间比较采用χ2检验和Fisher精确检验。釆用Kaplan-Meier法计算无进展生存期(PFS)和总生存期(OS)。使用Log-rank检验方法比较生存差异。应用单因素和多因素Cox比例风险回归模型分析生存预后的危险因素。 结果 共筛选到106例RICC患者,其中MWA+化疗组55例,MWA组51例。至随访截止,MWA+化疗组的中位PFS为15.0个月(95%CI:14.5~15.5),MWA组中位PFS为13.4个月(95%CI:11.6~15.2),两组差异有统计学意义(χ2=9.624,P=0.002)。MWA+化疗组的中位OS为21.0个月(95%CI:20.0~21.8),MWA组中位OS为18.0个月(95%CI:16.3~19.7),两组差异有统计学意义(χ2=12.784,P<0.001)。Cox回归分析显示,肿瘤直径(HR=0.425, 95%CI:0.208~0.868,P=0.019;HR=0.299, 95%CI:0.121~0.739,P=0.009)、复发时间(HR=7.064, 95%CI:3.612~13.618,P<0.001;HR=2.341, 95%CI:1.072~5.113,P=0.033)及联合化疗(HR=0.138, 95%CI:0.069~0.276,P<0.001;HR=0.175, 95%CI:0.081~0.380,P<0.001)是RICC患者PFS和OS的独立影响因素。两组常见不良反应中,除血液学毒性发生率(χ2=12.524,P<0.001)外,其余不良反应发生率差异均无统计学意义(P值均>0.05)。 结论 与单独MWA相比,MWA+化疗可以改善RICC的预后,延长其PFS和OS,且副反应安全可控。肿瘤直径>5 cm、复发时间<1年、未联合全身化疗的患者预后不良。 Abstract:Objective To investigate the efficacy and safety of microwave ablation (MWA) combined with chemotherapy versus MWA alone in the treatment of recurrent intrahepatic cholangiocarcinoma (RICC). Methods A retrospective cohort study was conducted among the patients with RICC who received MWA+chemotherapy or MWA in The Second People's Hospital of Neijiang and The Affiliated Hospital of Southwest Medical University from January 2014 to March 2021, and their clinicopathological data were collected. The independent samples t-test was used for comparison of continuous data, and the chi-square test and the Fisher's exact test were used for comparison of categorical data. The Kaplan-Meier method was used to calculate progression-free survival (PFS) and overall survival (OS), and the Log-rank test was used for comparison of survival differences. Univariate and multivariate Cox proportional-hazards regression model analyses were used to investigate the risk factors for survival and prognosis. Results A total of 106 patients with RIC were enrolled, among whom there were 55 patients in the MWA+chemotherapy group and 51 in the MWA group. By the end of follow-up, the MWA+chemotherapy group had a median PFS of 15.0 months (95% confidence interval [CI]: 14.5-15.5), and the MWA group had a median PFS of 13.4 months (95%CI: 11.6-15.2), with a significant difference between the two groups (χ2=9.624, P=0.002). The MWA+chemotherapy group had a median OS of 21.0 months (95%CI: 20.0-21.8), and the MWA group had a median OS of 18.0 months (95%CI: 16.3-19.7), with a significant difference between the two groups (χ2=12.784, P < 0.001). The Cox regression analysis showed that tumor diameter (PFS: hazard ratio [HR]=0.425, 95%CI: 0.208-0.868, P=0.019; OS: HR=0.299, 95%CI: 0.121-0.739, P=0.009), time to recurrence (PFS: HR=7.064, 95%CI: 3.612-13.618, P < 0.001; OS: HR=2.341, 95%CI: 1.072-5.113, P=0.033), and combined chemotherapy (PFS: HR=0.138, 95%CI: 0.069-0.276, P < 0.001; OS: HR=0.175, 95%CI: 0.081-0.380, P < 0.001) were independent influencing factors for PFS and OS in patients with RICC. As for the common adverse reactions, there were no significant differences in the incidence rates of all adverse reactions except hematological toxicity (χ2=12.524, P < 0.001). Conclusion Compared with MWA alone, MWA combined with chemotherapy can improve the prognosis of RICC and prolong PFS and OS, with safe and controllable side effects. Patients with tumor diameter > 5 cm, time to recurrence < 1 year, and absence of systemic chemotherapy tend to have a poor prognosis. -
Key words:
- Cholangiocarcinoma /
- Ablation Techniques /
- Drug Therapy
-
表 1 两组基线资料比较
Table 1. Comparison of baseline data between the two groups
项目 MWA+化疗(n=55) MWA(n=51) 统计值 P值 年龄(岁) 55.008±8.829 55.099±9.070 t=0.211 0.958 男性[例(%)] 39(70.9) 37(72.5) χ2=0.035 0.851 HBV感染 33(60.0) 27(52.9) χ2=0.537 0.464 肝硬化[例(%)] 36(65.5) 31(60.8) χ2=0.248 0.618 TBil(μmol/L) 41.025±13.796 37.208±12.988 t=1.465 0.146 AST(U/L) 65.891±23.122 73.093±24.721 t=-1.551 0.125 ALT(U/L) 69.755±24.965 79.076±35.183 t=-1.562 0.122 Alb(g/L) 38.684±4.069 38.882±3.806 t=-0.265 0.797 PT(s) 14.082±1.326 14.172±1.667 t=-0.310 0.757 INR 1.344±0.197 1.373±0.178 t=-0.806 0.421 CA19-9[例(%)] χ2=0.621 0.431 ≤37 U/mL 36(65.5) 37(72.5) >37 U/mL 19(34.5) 14(27.5) 术后复发TNM分期[例(%)] χ2=0.865 0.649 Ⅰ期 31(56.4) 26(51.0) Ⅱ期 17(30.9) 20(39.2) Ⅲ期 7(12.7) 5(9.8) 肿瘤直径[例(%)] χ2=0.907 0.119 ≤5 cm 35(63.6) 26(51.0) >5 cm 20(36.4) 25(49.0) 肿瘤个数[例(%)] χ2=0.794 0.268 1个 41(74.5) 34(66.7) 2~3个 14(25.5) 17(33.3) 首次切除时分化程度[例(%)] χ2=0.095 0.758 中高度 34(61.8) 33(64.7) 低度 21(38.2) 18(35.3) Child-Pugh分级[例(%)] χ2=0.484 0.486 A级 37(67.3) 31(60.8) B级 18(32.7) 20(39.2) 距初次切除后的复发时间[例(%)] χ2=2.358 0.125 ≤1年 33(60.0) 23(45.1) >1年 22(40.0) 28(54.9) 联合TACE[例(%)] χ2=0.028 0.867 是 38(69.1) 36(70.6) 否 17(30.9) 15(29.4)  下载: 导出CSV
下载: 导出CSV
表 2 RICC患者PFS的单因素分析
Table 2. Univariate analysis of PFS in patients with RICC
项目 HR P值 性别(男/女) 0.708(0.408~1.228) 0.219 年龄(>60/≤60岁) 1.243(0.729~2.120) 0.423 HBV(+)(是/否) 0.859(0.517~1.426) 0.557 TBil(>34.2 μmol/L/≤34.2 μmol/L) 2.498(1.497~4.169) 0.001 AST(>40 U/L/≤40 U/L) 0.754(0.343~1.657) 0.482 ALT(>40 U/L/≤40 U/L) 1.692(0.760~3.768) 0.198 Alb(>35 g/L/≤35 g/L) 1.930(1.061~3.512) 0.031 CA19-9(>37 ng/mL/≤37 ng/mL) 0.326(0.193~0.550) <0.001 TNM分期(≥Ⅱ期/Ⅰ期) 1.012(0.727~1.409) 0.943 肿瘤直径(>5 cm/≤5 cm) 0.353(0.212~0.588) <0.001 肿瘤个数(1个/2~3个) 0.778(0.453~1.335) 0.361 分化程度(中高/低) 0.472(0.287~0.775) 0.003 Child-Pugh分级(A/B) 1.165(0.690~1.969) 0.568 复发时间(>1年/≤1年) 4.286(2.505~7.331) <0.001 联合化疗(是/否) 0.437(0.255~0.747) 0.002 联合TACE(是/否) 0.756(0.446~1.281) 0.298
下载: 导出CSV
表 3 RICC患者OS的单因素分析
Table 3. Univariate analysis of OS in patients with RICC
项目 HR P值 性别(男/女) 0.625(0.329~1.187) 0.151 年龄(>60岁/≤60岁) 0.753(0.578~2.134) 0.753 HBV(+)(是/否) 0.754(0.413~1.376) 0.357 TBil(>34.2 μmol/L/≤34.2 μmol/L) 1.570(0.855~2.883) 0.146 AST(>40 U/L/≤40 U/L) 0.912(0.357~2.332) 0.848 ALT(>40 U/L/≤40 U/L) 2.010(0.778~5.196) 0.150 Alb(>35.0 g/L/≤35.0 g/L) 1.429(0.658~3.106) 0.367 CA19-9>40 ng/mL(是/否) 0.412(0.224~0.756) 0.004 TNM分期(≥Ⅱ期/Ⅰ期) 1.188(0.652~2.166) 0.574 肿瘤直径(>5 cm/≤5 cm) 0.244(0.127~0.470) <0.001 肿瘤个数(1个/2~3个) 0.835(0.427~1.631) 0.598 分化程度(中高/低) 0.502(0.274~0.922) 0.026 Child-Pugh分级(A/B) 0.970(0.512~1.839) 0.927 复发时间(>1年/≤1年) 2.606(1.382~4.912) 0.003 联合化疗(是/否) 0.339(0.177~0.651) 0.001 联合TACE(是/否) 0.629(0.335~1.179) 0.148
下载: 导出CSV
表 4 两组不良反应比较
Table 4. Comparison of complications between the two groups
项目 MWA+化疗(n=55) MWA(n=51) χ2值 P值 所有级别 3~4级 所有级别 3~4级 血液学毒性[例(%)] 18(32.7) 2(3.6) 2(3.9) 0(0.0) 12.524 <0.001 乏力[例(%)] 22(40.0) 3(5.5) 16(31.4) 1(2.0) 0.856 0.355 胃肠道反应[例(%)] 21(38.2) 2(3.6) 11(21.6) 1(2.0) 3.465 0.063 疼痛[例(%)] 18(32.7) 0(0.0) 15(29.4) 2(3.9) 0.136 0.713 肝功能异常[例(%)] 16(29.1) 1(1.8) 10(19.6) 0(0.0) 1.286 0.257 发热[例(%)] 8(14.5) 0(0.0) 4(7.8) 0(0.0) 0.277 出血[例(%)] 1(1.8) 0(0.0) 2(3.9) 0(0.0) 0.607 腹水/胸水[例(%)] 2(3.6) 0(0.0) 4(7.8) 0(0.0) 0.425 血栓[例(%)] 1(1.8) 0(0.0) 0(0.0) 0(0.0) >0.05
下载: 导出CSV
-
[1] KHAN SA, DAVIDSON BR, GOLDIN RD, et al. Guidelines for the diagnosis and treatment of cholangiocarcinoma: an update[J]. Gut, 2012, 61(12): 1657-1669. DOI: 10.1136/gutjnl-2011-301748. [2] DING XY, SUN W, SHEN YJ, et al. Efficacy and safety of lenvatinib combined with sintilimab as the second-line therapy for intrahepatic cholangiocarcinoma[J]. J Clin Hepatol, 2022, 38(8): 1813-1818. DOI: 10.3969/j.issn.1001-5256.2022.08.018.丁晓燕, 孙巍, 申燕军, 等. 仑伐替尼联合信迪利单抗二线治疗肝内胆管癌的效果和安全性[J]. 临床肝胆病杂志, 2022, 38(8): 1813-1818. DOI: 10.3969/j.issn.1001-5256.2022.08.018. [3] CLOYD JM, EJAZ A, PAWLIK TM. The Landmark series: Intrahepatic cholangiocarcinoma[J]. Ann Surg Oncol, 2020, 27(8): 2859-2865. DOI: 10.1245/s10434-020-08621-4. [4] DOUSSOT A, GONEN M, WIGGERS JK, et al. Recurrence patterns and disease-free survival after resection of intrahepatic cholangiocarcinoma: Preoperative and postoperative prognostic models[J]. J Am Coll Surg, 2016, 223(3): 493-505. e2. DOI: 10.1016/j.jamcollsurg.2016.05.019. [5] WRIGHT GP, PERKINS S, JONES H, et al. Surgical resection does not improve survival in multifocal intrahepatic cholangiocarcinoma: A comparison of surgical resection with intra-arterial therapies[J]. Ann Surg Oncol, 2018, 25(1): 83-90. DOI: 10.1245/s10434-017-6110-1. [6] BARTSCH F, PASCHOLD M, BAUMGART J, et al. Surgical resection for recurrent intrahepatic cholangiocarcinoma[J]. World J Surg, 2019, 43(4): 1105-1116. DOI: 10.1007/s00268-018-04876-x. [7] ZHANG XF, BEAL EW, BAGANTE F, et al. Early versus late recurrence of intrahepatic cholangiocarcinoma after resection with curative intent[J]. Br J Surg, 2018, 105(7): 848-856. DOI: 10.1002/bjs.10676. [8] LI M, LU YY, DONG JH, et al. Clinical effect of transcatheter arterial chemoembolization combined with microwave ablation in treatment of advanced primary liver cancer[J]. J Clin Hepatol, 2020, 36(12): 2720-2724. DOI: 10.3969/j.issn.1001-5256.2020.12.016.李猛, 陆荫英, 董景辉, 等. 经肝动脉化疗栓塞术联合微波消融治疗中晚期原发性肝癌的效果分析[J]. 临床肝胆病杂志, 2020, 36(12): 2720-2724. DOI: 10.3969/j.issn.1001-5256.2020.12.016. [9] HAN Y, SHAO N, XI X, et al. Use of microwave ablation in the treatment of patients with multiple primary malignant tumors[J]. Thorac Cancer, 2017, 8(4): 365-371. DOI: 10.1111/1759-7714.12445. [10] XU C, LI L, XU W, et al. Ultrasound-guided percutaneous microwave ablation versus surgical resection for recurrent intrahepatic cholangiocarcinoma: intermediate-term results[J]. Int J Hyperthermia, 2019, 36(1): 351-358. DOI: 10.1080/02656736.2019.1571247. [11] SPOLVERATO G, KIM Y, ALEXANDRESCU S, et al. Management and outcomes of patients with recurrent intrahepatic cholangiocarcinoma following previous curative-intent surgical resection[J]. Ann Surg Oncol, 2016, 23(1): 235-243. DOI: 10.1245/s10434-015-4642-9. [12] YUAN ZB, FANG HB, FENG QK, et al. Prognostic factors of recurrent intrahepatic cholangiocarcinoma after hepatectomy: A retrospective study[J]. World J Gastroenterol, 2022, 28(15): 1574-1587. DOI: 10.3748/wjg.v28.i15.1574. [13] VALLE J, WASAN H, PALMER DH, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer[J]. N Engl J Med, 2010, 362(14): 1273-1281. DOI: 10.1056/NEJMoa0908721. [14] MIURA JT, JOHNSTON FM, TSAI S, et al. Chemotherapy for surgically resected intrahepatic cholangiocarcinoma[J]. Ann Surg Oncol, 2015, 22(11): 3716-3723. DOI: 10.1245/s10434-015-4501-8. [15] BENSON AB, D'ANGELICA MI, ABBOTT DE, et al. Hepatobiliary cancers, version 2.2021, NCCN clinical practice guidelines in oncology[J]. J Natl Compr Canc Netw, 2021, 19(5): 541-565. DOI: 10.6004/jnccn.2021.0022. [16] SPOLVERATO G, EJAZ A, KIM Y, et al. Rates and patterns of recurrence after curative intent resection for gastric cancer: a United States multi-institutional analysis[J]. J Am Coll Surg, 2014, 219(4): 664-675. DOI: 10.1016/j.jamcollsurg.2014.03.062. [17] EISENHAUER EA, THERASSE P, BOGAERTS J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1)[J]. Eur J Cancer, 2009, 45(2): 228-247. DOI: 10.1016/j.ejca.2008.10.026. [18] MAVROS MN, ECONOMOPOULOS KP, ALEXIOU VG, et al. Treatment and prognosis for patients with intrahepatic cholangiocarcinoma: Systematic review and meta-analysis[J]. JAMA Surg, 2014, 149(6): 565-574. DOI: 10.1001/jamasurg.2013.5137. [19] LURJE G, BEDNARSCH J, RODERBURG C, et al. Intrahepatic cholangiocarcinoma - current perspectives and treatment algorithm[J]. Chirurg, 2018, 89(11): 858-864. DOI: 10.1007/s00104-018-0718-y. [20] TAKAHASHI Y, EBATA T, YOKOYAMA Y, et al. Surgery for recurrent biliary tract cancer: A single-center experience with 74 consecutive resections[J]. Ann Surg, 2015, 262(1): 121-129. DOI: 10.1097/SLA.0000000000000827. [21] YANG HI, SHERMAN M, SU J, et al. Nomograms for risk of hepatocellular carcinoma in patients with chronic hepatitis B virus infection[J]. J Clin Oncol, 2010, 28(14): 2437-2444. DOI: 10.1200/JCO.2009.27.4456. [22] KIM GH, KIM PH, KIM JH, et al. Thermal ablation in the treatment of intrahepatic cholangiocarcinoma: a systematic review and meta-analysis[J]. Eur Radiol, 2022, 32(2): 1205-1215. DOI: 10.1007/s00330-021-08216-x. [23] SHROFF RT, KENNEDY EB, BACHINI M, et al. Adjuvant Therapy for resected biliary tract cancer: ASCO clinical practice guideline[J]. J Clin Oncol, 2019, 37(12): 1015-1027. DOI: 10.1200/JCO.18.02178. [24] DÍAZ-GONZÁLEZÁ, VILANA R, BIANCHI L, et al. Thermal ablation for intrahepatic cholangiocarcinoma in cirrhosis: Safety and efficacy in non-surgical patients[J]. J Vasc Interv Radiol, 2020, 31(5): 710-719. DOI: 10.1016/j.jvir.2019.06.014. [25] HAN K, KO HK, KIM KW, et al. Radiofrequency ablation in the treatment of unresectable intrahepatic cholangiocarcinoma: systematic review and meta-analysis[J]. J Vasc Interv Radiol, 2015, 26(7): 943-948. DOI: 10.1016/j.jvir.2015.02.024. [26] CARRAFIELLO G, LAGANÀ D, COTTA E, et al. Radiofrequency ablation of intrahepatic cholangiocarcinoma: preliminary experience[J]. Cardiovasc Intervent Radiol, 2010, 33(4): 835-839. DOI: 10.1007/s00270-010-9849-3. [27] SHI Q, CHEN D, ZHOU C, et al. Drug-eluting beads versus lipiodol transarterial chemoembolization for the treatment of hypovascular hepatocellular carcinoma: A single-center retrospective study[J]. Cancer Manag Res, 2020, 12: 5461-5468. DOI: 10.2147/CMAR.S255960. [28] FENG R, TAO ZG, XU HY, et al. The short-term curative effect of the callisphere drug embolization microsphere in the treatment of malignant tumor of the liver[J]. J Clin Radiol, 2019, 38(6): 1107-1111. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201906040.htm冯锐, 陶志刚, 徐后云, 等. CalliSpheres载药栓塞微球治疗肝脏乏血供恶性肿瘤短期疗效分析[J]. 临床放射学杂志, 2019, 38(6): 1107-1111. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201906040.htm [29] CHEN X, DU J, HUANG J, et al. Neoadjuvant and adjuvant therapy in intrahepatic cholangiocarcinoma[J]. J Clin Transl Hepatol, 2022, 10(3): 553-563. DOI: 10.14218/JCTH.2021.00250. [30] STEIN A, ARNOLD D, BRIDGEWATER J, et al. Adjuvant chemotherapy with gemcitabine and cisplatin compared to observation after curative intent resection of cholangiocarcinoma and muscle invasive gallbladder carcinoma (ACTICCA-1 trial) - a randomized, multidisciplinary, multinational phase Ⅲ trial[J]. BMC Cancer, 2015, 15: 564. DOI: 10.1186/s12885-015-1498-0. [31] EDELINE J, BENABDELGHANI M, BERTAUT A, et al. Gemcitabine and oxaliplatin chemotherapy or surveillance in resected biliary tract cancer (PRODIGE 12-ACCORD 18-UNICANCER GI): A Randomized Phase Ⅲ Study[J]. J Clin Oncol, 2019, 37(8): 658-667. DOI: 10.1200/JCO.18.00050. [32] MAZZAFERRO V, GORGEN A, ROAYAIE S, et al. Liver resection and transplantation for intrahepatic cholangiocarcinoma[J]. J Hepatol, 2020, 72(2): 364-377. DOI: 10.1016/j.jhep.2019.11.020. -

 本文二维码
本文二维码
计量
- 文章访问数: 256
- HTML全文浏览量: 71
- PDF下载量: 22
- 被引次数: 0

