
 PDF下载 ( 3410 KB)
PDF下载 ( 3410 KB)

重症急性胰腺炎继发持续性炎症-免疫抑制-分解代谢综合征的影响因素及预测模型构建
DOI: 10.3969/j.issn.1001-5256.2023.06.019
Influencing factors for persistent inflammation, immunosuppression, and catabolism syndrome in patients with severe acute pancreatitis and establishment of a predictive model
-
摘要:
目的 探讨重症急性胰腺炎(SAP)继发持续性炎症-免疫抑制-分解代谢综合征(PICS)的影响因素,并构建预测模型。 方法 回顾性分析2012年5月—2022年5月广西医科大学第一附属医院163例因SAP收入重症医学科、急诊重症监护室患者的临床资料。依据PICS诊断标准分成2组:PICS组(65例,SAP发生PICS患者)和非PICS组(98例,SAP未发生PICS患者)。符合正态分布的计量资料2组间比较采用成组t检验;不符合正态分布的计量资料2组间比较采用Mann-Whitney U秩和检验。计数资料2组间比较采用χ2检验或Fisher确切概率法。计算方差膨胀因子、相关系数矩阵热图评估变量间多重共线性,采用Lasso回归及多因素Logistic回归筛选出独立危险因素,构建列线图预测模型。采用受试者工作特征曲线、校准曲线及Hosmer-Lemeshow拟合优度检验对模型进行内部验证;采用临床决策曲线评估模型的临床实用性。 结果 单因素分析结果显示,平均动脉压、血红蛋白、红细胞压积(HCT)、中性粒细胞与淋巴细胞比值、血小板与淋巴细胞比值(PLR)、尿素、肌酐、格拉斯哥昏迷评分(GCS)、APACHE Ⅱ、SOFA、机械通气、急性呼吸窘迫综合征、急性肾损伤(AKI)、急性肝损伤、低血容量性休克、脓毒症、腹腔高压、腹腔出血、多器官功能障碍综合征在PICS组和非PICS组间比较差异均有统计学意义(P值均<0.05)。Lasso回归筛选的预测变量包括PLR、HCT、APACHE Ⅱ、SOFA、机械通气、AKI、低血容量性休克、腹腔高压。多因素Logistic回归显示,PLR、机械通气、AKI、低血容量性休克是SAP发生PICS的独立危险因素(OR分别为1.006、4.324、3.432、6.910,P值均<0.05)。将上述因素进行模型拟合,经bootstrap内部验证列线图模型曲线下面积为0.874(95%CI:0.822~0.925),校准曲线接近参考曲线,Hosmer-Lemeshow拟合优度检验表明该模型具有良好的拟合度(χ2=8.895,P=0.351)。临床决策曲线分析显示预测模型具有良好的临床实用性。 结论 PLR、机械通气、AKI、低血容量性休克是SAP继发PICS的独立危险因素,构建的列线图模型具有良好的区分度、校准度和临床实用性。 -
关键词:
- 胰腺炎 /
- 持续性炎症-免疫抑制-分解代谢综合征 /
- 危险因素
Abstract:Objective To investigate the influencing factors for persistent inflammation, immunosuppression, and catabolism syndrome (PICS) in patients with severe acute pancreatitis(SAP), and to establish a predictive model. Methods A retrospective analysis was performed for the clinical data of 163 patients who were admitted to the intensive care unit and the emergency intensive care unit due to SAP in The First Affiliated Hospital of Guangxi Medical University from May 2012 to May 2022, and according to the diagnostic criteria for PICS, these patients were divided into PICS group (65 SAP patients with PICS) and non-PICS group (98 SAP patients without PICS). The independent-samples t test was used for comparison of normally distributed continuous data between two groups, and the Mann-Whitney U rank sum test was used for comparison of non-normally distributed continuous data between two groups; the chi-square test or the Fisher's exact test was used for comparison of categorical data between two groups. Variance inflation factor and correlation matrix heatmap were used to evaluate multicollinearity between variables, and Lasso regression and multivariate logistic regression were used to identify independent risk factors and establish a nomogram predictive model. The receiver operating characteristic (ROC) curve, the calibration curve, and the Hosmer-Lemeshow goodness-of-fit test were used for the internal validation of the model, and the decision curve was used to evaluate the clinical practicability of the model. Results The univariate analysis showed that there were significant differences between the PICS group and the non-PICS group in mean arterial pressure, hemoglobin, hematocrit (HCT), neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio (PLR), blood urea nitrogen, creatinine, Glasgow coma score, Acute Physiology and Chronic Health Evaluation Ⅱ (APACHE Ⅱ) score, Sequential Organ Failure Assessment (SOFA) score, mechanical ventilation, acute respiratory distress syndrome, acute kidney injury (AKI), acute liver injury, hypovolemic shock, sepsis, intra-abdominal hypertension, intra-abdominal hemorrhage, and multiple organ dysfunction syndrome (all P < 0.05). The Lasso regression analysis showed that related predictive variables included PLR, HCT, APACHE Ⅱ, SOFA, mechanical ventilation, AKI, hypovolemic shock, and intra-abdominal hypertension, and the multivariate logistic regression analysis showed that PLR (odds ratio [OR]=1.006, P < 0.05), mechanical ventilation (OR=4.324, P < 0.05), AKI (OR=3.432, P < 0.05), and hypovolemic shock (OR= 6.910, P < 0.05) were independent risk factors for PICS in patients with SAP. Model fitting was performed for the above factors, and bootstrap internal validation showed that the nomogram model had an area under the ROC curve of 0.874 (95% confidence interval: 0.822-0.925); the calibration curve of the model was close to the reference curve, and the Hosmer-Lemeshow goodness-of-fit test showed that the model was well fitted (χ2=8.895, P=0.351). The decision curve analysis showed that the predictive model had good clinical practicability. Conclusion PLR, mechanical ventilation, AKI, and hypovolemic shock are independent risk factors for PICS in patients with SAP, and the nomogram model established has good discriminatory ability, calibration, and clinical practicability. -
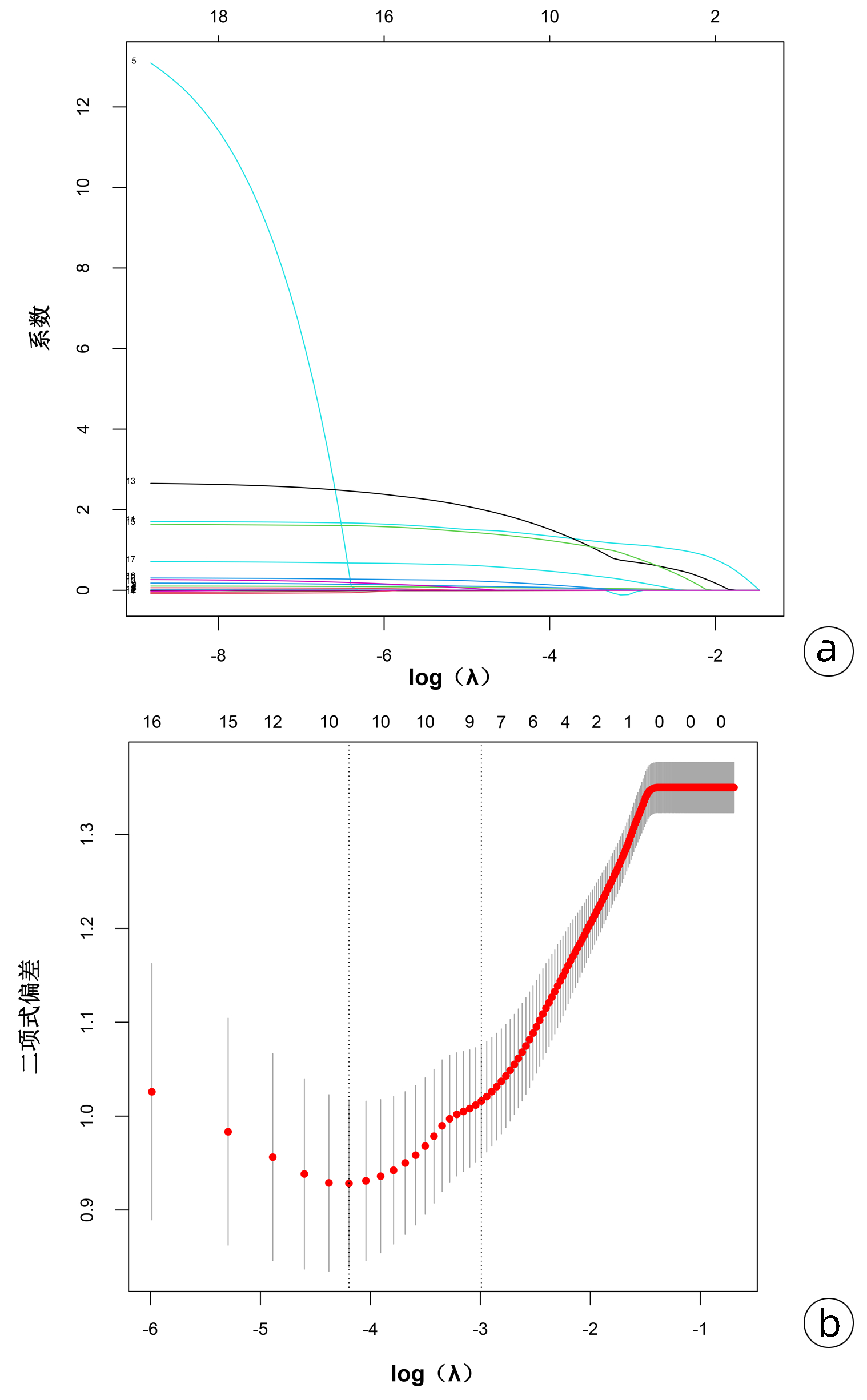
图 2 Lasso回归进行临床特征筛选
注:a,19个临床特征的系数曲线;b,Lasso回归10倍交叉验证选择临床特征。
Figure 2. Selection of potential predictors of PICS in patients with SAP by the Lasso regression
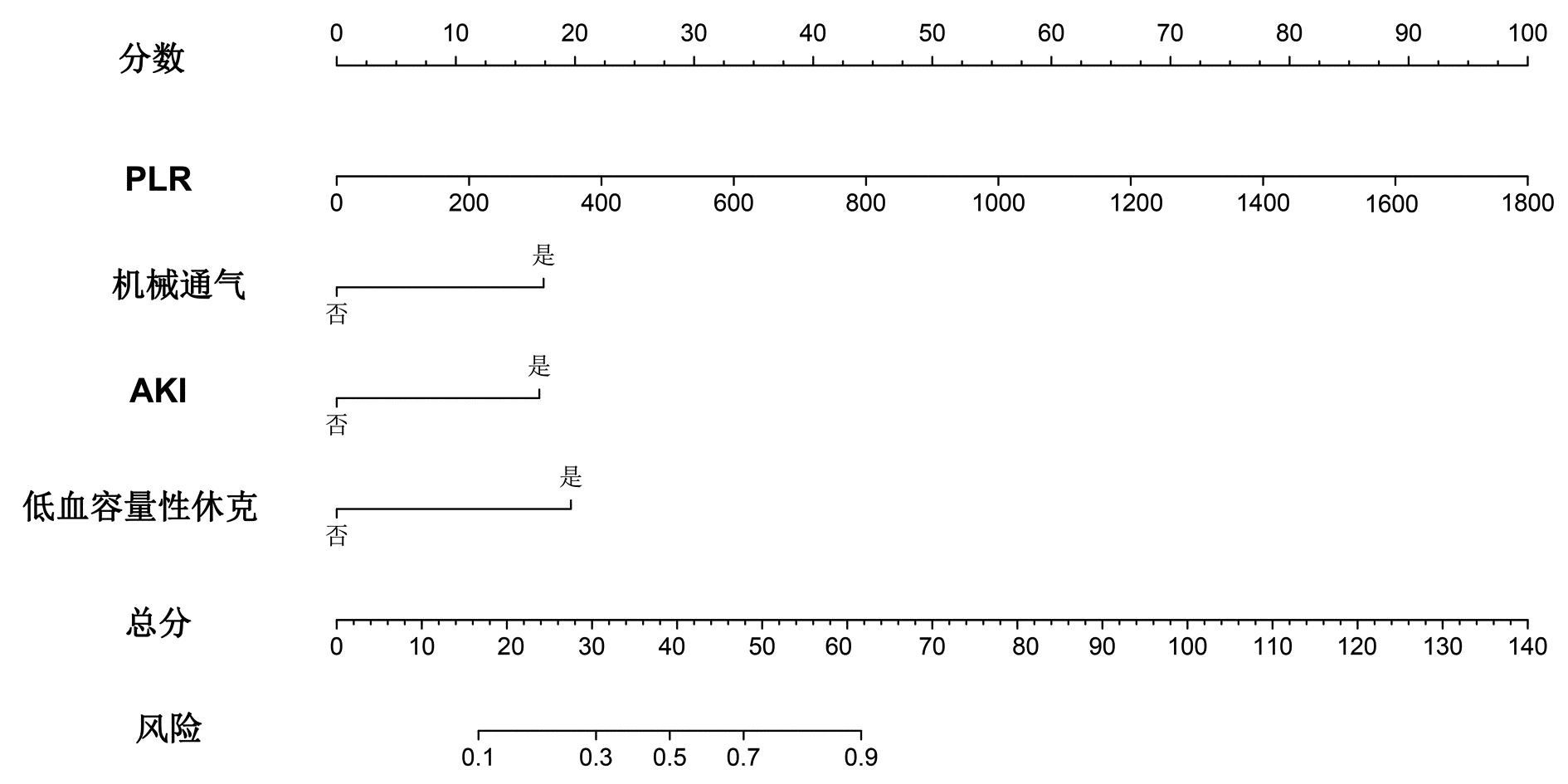
图 3 SAP患者发生PICS风险预测模型列线图
Figure 3. Nomogram of the risk predictive model for PICS in SAP patients
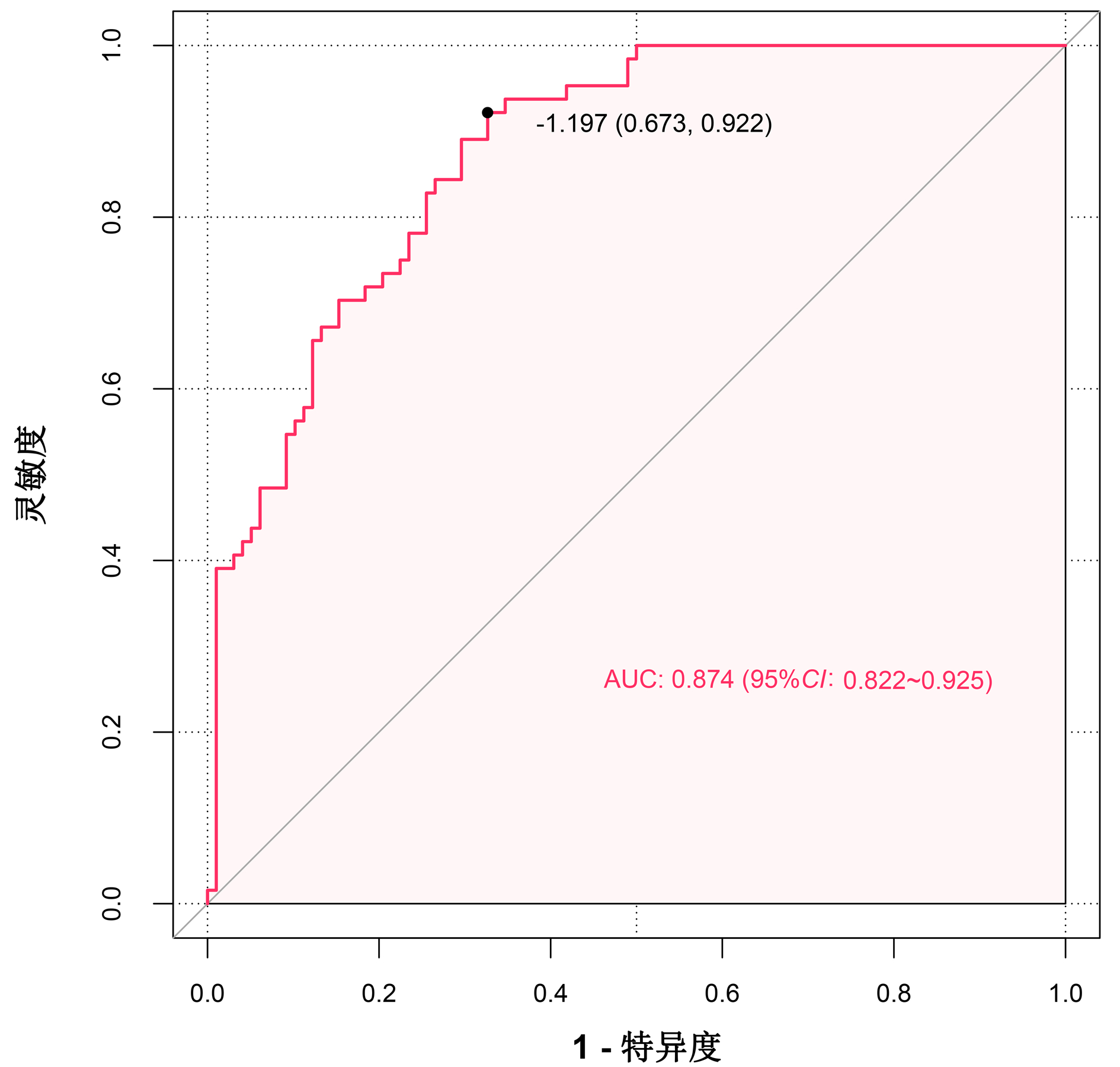
图 4 SAP患者发生PICS风险预测模型的ROC曲线
Figure 4. ROC curve of the risk predictive model for PICS in SAP patients

图 5 SAP患者发生PICS风险预测模型的校准曲线
Figure 5. Calibration curve of the risk predictive model for PICS in SAP patients
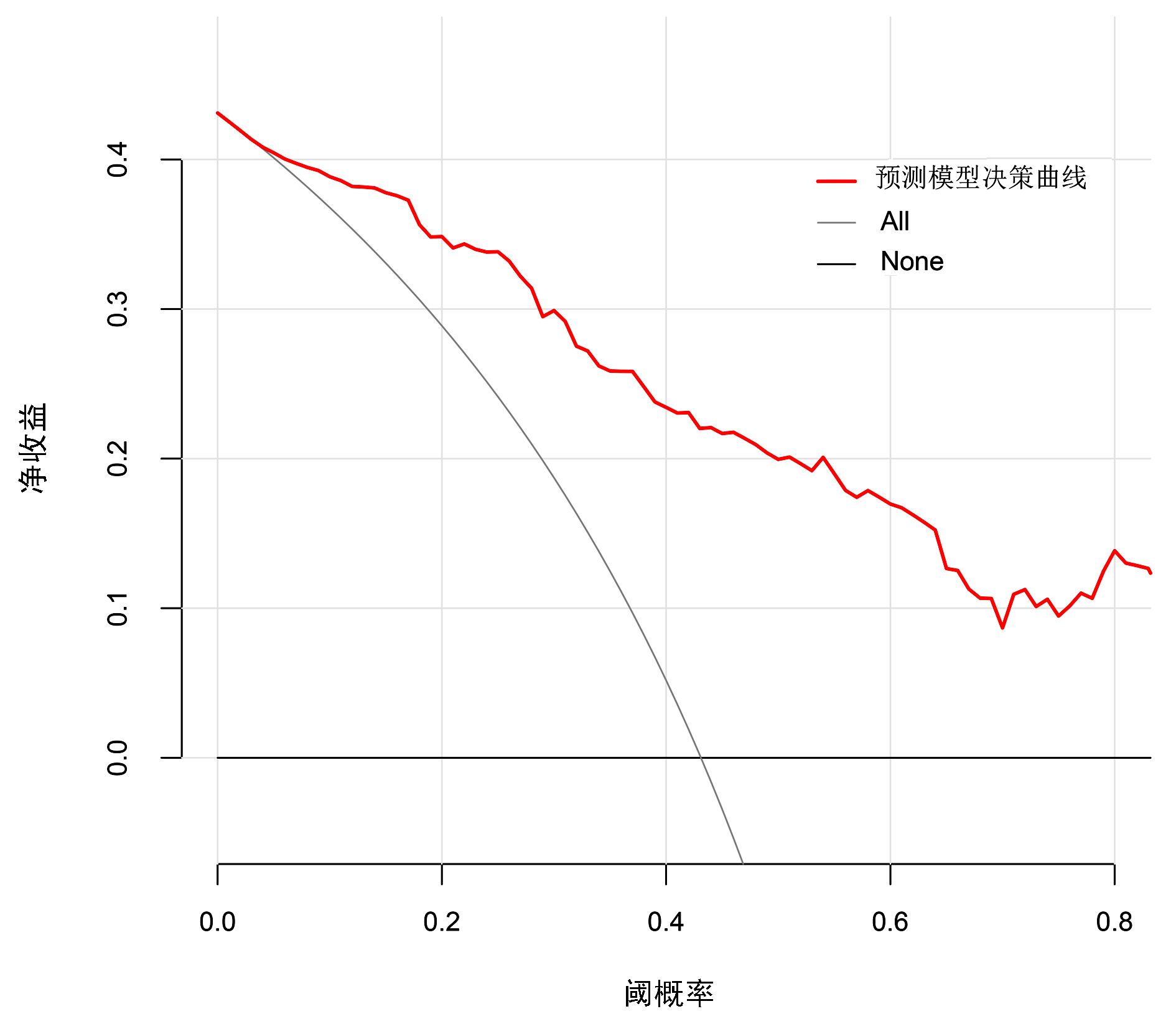
图 6 SAP患者发生PICS风险预测模型的决策曲线
Figure 6. Decision curve of the risk predictive model for PICS in SAP patients
表 1 2组患者一般资料比较
Table 1. Comparison of general data between the two groups
项目 PICS组(n=65) 非PICS组(n=98) 统计值 P值 年龄(岁) 48.00(39.50~59.00) 47.50(37.00~59.25) Z=-0.005 0.996 性别[例(%)] χ2=0.916 0.339 男 52(80.0) 72(73.5) 女 13(20.0) 26(26.5) BMI(kg/m2) 23.94(22.00~27.55) 24.98(22.49~27.76) Z=-0.668 0.504 既往史[例(%)] 高血压 14(34.7) 34(20.9) χ2=3.255 0.071 糖尿病 8(12.3) 15(15.3) χ2=0.290 0.590 腹部疾病 27(41.5) 52(53.1) χ2=1.897 0.168 SAP病因[例(%)] 胆源性 5(7.7) 11(1.1) χ2=0.551 0.458 高脂血症性 17(26.2) 34(34.7) χ2=1.326 0.250 酒精性 12(18.5) 18(18.4) χ2<0.001 0.988 创伤性 2(3.1) 3(3.1) χ2<0.001 0.995 病因不明 29(44.6) 32(32.7) χ2=2.388 0.122 体温(℃) 37.60(37.00~38.00) 37.50(36.78~38.10) Z=-0.553 0.580 心率(次/min) 119.43±23.02 112.69±21.48 t=1.881 0.062 呼吸(次/min) 24.00(20.00~33.00) 26.00(21.50~32.00) Z=-1.064 0.287 平均动脉压(mmHg) 98.33(80.67~111.67) 104.50(91.59~113.08) Z=-2.207 0.027 预后 开放饮食时间(d) 8.00(3.50~13.50) 7.00(3.00~11.00) Z=-1.288 0.198 病死率[例(%)] 26(40.0) 16(16.3) χ2=11.450 0.001 住院时间(d) 30.00(22.00~51.00) 22.00(17.00~27.25) Z=-4.666 <0.001 总费用(万元) 22.23(12.10~39.31) 8.18(6.06~11.86) Z=-6.893 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 2组患者PICS指标比较
Table 2. Comparison of PICS factors between the two groups
指标 PICS组(n=65) 非PICS组(n=98) Z值 P值 ICU住院时间(d) 22.00(16.00~42.50) 7.00(4.00~11.00) -8.862 <0.001 CRP(mg/L) 180.39(120.84~192.00) 190.67(109.04~192.00) -0.265 0.791 Lym(×109/L) 0.60(0.49~0.75) 1.07(0.72~1.39) -6.547 <0.001 前白蛋白(g/L) 83.30(52.25~104.15) 110.90(76.73~155.35) -3.488 <0.001 白蛋白(g/L) 28.30(26.10~31.25) 30.80(27.58~34.78) -3.517 <0.001
下载: 导出CSV
表 3 2组患者实验室指标和并发症比较
Table 3. Comparison of laboratory data and complication between the two groups
指标 PICS组(n=65) 非PICS组(n=98) 统计值 P值 WBC(×109/L) 14.46(8.94~18.69) 14.72(10.45~20.09) Z=-0.857 0.391 Hb(g/L) 87.70(75.05~112.70) 106.60(83.68~126.13) Z=-2.532 0.011 血小板计数(×109/L) 176.00(117.15~237.20) 196.35(141.93~272.40) Z=-1.366 0.172 Neu(×109/L) 13.22(8.00~17.00) 12.18(8.38~17.45) Z=-0.095 0.924 NLR 21.69(11.47~30.30) 12.35(7.41~23.13) Z=-3.383 0.001 PLR 261.85(198.42~455.46) 207.28(118.19~315.79) Z=-3.210 0.001 HCT 0.26(0.22~0.36) 0.33(0.26~0.39) Z=-2.649 0.008 PH 7.44(7.36~7.48) 7.43(7.38~7.48) Z=-0.061 0.951 PO2(mmHg) 102.00(78.05~136.05) 88.50(71.00~126.03) Z=-1.161 0.246 PCO2(mmHg) 34.10(30.40~39.40) 35.55(30.00~39.00) Z=-0.278 0.781 氧合指数 253.00(198.00~332.90) 234.50(184.25~326.50) Z=-0.552 0.581 血Na(mmol/L) 138.10(133.95~143.20) 137.00(133.80~140.95) Z=-0.727 0.467 血K(mmol/L) 4.10(3.80~4.52) 4.00(3.59~4.31) Z=-1.466 0.143 TBil(μmol/L) 26.30(13.30~47.30) 20.55(12.48~35.03) Z=-1.469 0.142 DBil(μmol/L) 13.30(6.25~28.20) 9.30(5.00~18.75) Z=-1.737 0.082 BUN(mmol/L) 10.36(6.32~17.51) 6.43(4.15~10.50) Z=-3.250 0.001 SCr(μmol/L) 152.00(71.50~293.50) 73.50(55.75~141.00) Z=-2.915 0.004 血淀粉酶(U/L) 76.00(44.00~306.50) 103.00(53.75~389.75) Z=-0.935 0.350 GCS评分 15.00(13.00~15.00) 15.00(15.00~15.00) Z=-2.973 0.003 APACHE Ⅱ 13.00(10.00~16.00) 11.00(7.75~14.00) Z=-3.173 0.002 SOFA 6.00(4.00~10.00) 4.00(2.00~6.00) Z=-4.309 <0.001 并发症[例(%)] 机械通气 54(83.1) 34(34.7) χ2=17.785 <0.001 ARDS 54(83.1) 49(50.0) χ2=17.785 <0.001 AKI 40(61.5) 23(23.5) χ2=44.521 <0.001 急性肝损伤 16(24.6) 12(12.2) χ2=105.631 <0.001 低血容量性休克 15(23.1) 3(3.1) χ2=108.741 <0.001 脓毒症 37(56.9) 27(27.6) χ2=50.971 <0.001 肺部感染 63(96.9) 90(91.8) χ2=3.053 0.158 腹腔高压 34(52.3) 22(22.4) χ2=57.715 <0.001 腹腔出血 12(18.5) 6(6.1) χ2=118.409 <0.001 肠瘘 2(3.1) 2(2.0) χ2=0.175 0.524 MODS 49(75.4) 36(36.7) χ2=26.749 <0.001
下载: 导出CSV
表 4 SAP患者发生PICS多因素Logistic回归分析
Table 4. Multivariate logistic regression analysis of PICS in patients with SAP
变量 β值 P值 OR 95%CI PLR 0.006 <0.001 1.006 1.003~1.009 HCT -2.810 0.256 0.060 0.000~7.768 APACHE Ⅱ 0.076 0.124 1.079 0.982~1.195 SOFA 0.053 0.458 1.055 0.913~1.216 机械通气 1.464 0.002 4.324 1.723~11.423 AKI 1.233 0.018 3.432 1.253~9.854 低血容量性休克 1.933 0.013 6.910 1.685~39.068 腹腔高压 0.743 0.107 2.102 0.852~5.245
下载: 导出CSV
-
[1] VANZANT EL, LOPEZ CM, OZRAZGAT-BASLANTI T, et al. Persistent inflammation, immunosuppression, and catabolism syndrome after severe blunt trauma[J]. J Trauma Acute Care Surg, 2014, 76(1): 21-29. DOI: 10.1097/TA.0b013e3182ab1ab5. [2] GENTILE LF, CUENCA AG, EFRON PA, et al. Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care[J]. J Trauma Acute Care Surg, 2012, 72(6): 1491-1501. DOI: 10.1097/TA.0b013e318256e000. [3] MIRA JC, GENTILE LF, MATHIAS BJ, et al. Sepsis pathophysiology, chronic critical illness, and persistent inflammation-immunosuppression and catabolism syndrome[J]. Crit Care Med, 2017, 45(2): 253-262. DOI: 10.1097/CCM.0000000000002074. [4] NAKAMURA K, OGURA K, NAKANO H, et al. C-reactive protein clustering to clarify persistent inflammation, immunosuppression and catabolism syndrome[J]. Intensive Care Med, 2020, 46(3): 437-443. DOI: 10.1007/s00134-019-05851-3. [5] EFRON PA, MOHR AM, BIHORAC A, et al. Persistent inflammation, immunosuppression, and catabolism and the development of chronic critical illness after surgery[J]. Surgery, 2018, 164(2): 178-184. DOI: 10.1016/j.surg.2018.04.011. [6] XU D, XUN J. Persistentinflammation-immunosuppression-catabolism syndrome in severe acute pancreatitis[J]. J Chin Pract Diagn Ther, 2018, 32(7): 725-728. DOI: 10.13507/j.issn.1674-3474.2018.07.030.徐冬, 荀江. 重症急性胰腺炎并持续性炎症-免疫抑制-分解代谢综合征研究进展[J]. 中华实用诊断与治疗杂志, 2018, 32(7): 725-728. DOI: 10.13507/j.issn.1674-3474.2018.07.030. [7] YANG R, DU LL, ZHANG ZD, et al. Clinical observation of severe patients with persistent inflammation immunosuppression catabolism syndrome[J]. China J Emerg Resuscitation Disaster Med, 2021, 16(8): 919-921. DOI: 10.3969/j.issn.1673-6966.2021.08.021.杨蓉, 杜玲玲, 章志丹, 等. 重症患者持续性炎症-免疫抑制-分解代谢综合征的临床观察研究[J]. 中国急救复苏与灾害医学杂志, 2021, 16(8): 919-921. DOI: 10.3969/j.issn.1673-6966.2021.08.021. [8] KOUPENOVA M, CLANCY L, CORKREY HA, et al. Circulating platelets as mediators of immunity, inflammation, and thrombosis[J]. Circ Res, 2018, 122(2): 337-351. DOI: 10.1161/circresaha.117.310795. [9] ZHOU H, MEI X, HE X, et al. Severity stratification and prognostic prediction of patients with acute pancreatitis at early phase: A retrospective study[J]. Medicine (Baltimore), 2019, 98(16): e15275. DOI: 10.1097/md.0000000000015275. [10] HAWKINS RB, RAYMOND SL, STORTZ JA, et al. Chronic critical illness and the persistent inflammation, immunosuppression, and catabolism syndrome[J]. Front Immunol, 2018, 9: 1511. DOI: 10.3389/fimmu.2018.01511. [11] CHEN MY, CHEN MX, WANG MX, et al. Risk factors for acute kidney injury in severe acute pancreatitis: a Meta-analysis[J]. Chin Gen Pract, 2022, 25(30): 3834-3842. DOI: 10.12114/j.issn.1007-9572.2022.0452.陈美颖, 陈木欣, 王明欣, 等. 重症急性胰腺炎患者并发急性肾损伤危险因素的Meta分析[J]. 中国全科医学, 2022, 25(30): 3834-3842. DOI: 10.12114/j.issn.1007-9572.2022.0452. [12] WANG X, ZHUANG X, WEI R, et al. Protective effects of Acanthopanax vs. Ulinastatin against severe acute pancreatitis-induced brain injury in rats[J]. Int Immunopharmacol, 2015, 24(2): 285-298. DOI: 10.1016/j.intimp.2014.12.020. [13] WANG Y, QI WJ, ZENG YW, et al. Mechanism of action of magnolol in the treatment of acute lung injury in a rat model of severe acute pancreatitis[J]. J Clin Hepatol, 2020, 36(12): 2782-2787. DOI: 10.3969/j.issn.1001-5256.2020.12.028.王燕, 齐文杰, 曾亚薇, 等. 厚朴酚治疗重症急性胰腺炎大鼠模型并发急性肺损伤的作用机制[J]. 临床肝胆病杂志, 2020, 36(12): 2782-2787. DOI: 10.3969/j.issn.1001-5256.2020.12.028. [14] WANG X, WANG XK, CEN RF, et al. Influence of Xuebijing injection on clinical effects and cellular immune function of patients with severe acute pancreatitis[J]. Chin J New Drugs Clin Rem, 2015, 34(6): 476-479. DOI: 10.14109/j.cnki.xyylc.2015.06.016.王雪, 王先坤, 岑荣飞, 等. 血必净注射液对重症急性胰腺炎疗效及患者细胞免疫功能的影响[J]. 中国新药与临床杂志, 2015, 34(6): 476-479. DOI: 10.14109/j.cnki.xyylc.2015.06.016. [15] WANG P, LI L, LAN D, et al. Effects of hemofiltration therapy on biochemical indexes, liver and kidney function and inflammatory factors in patients with severe acute pancreatitis complicated with abdominal compartment syndrome[J]. J Clin Exp Med, 2022, 21(4): 384-388. DOI: 10.3969/j.issn.1671-4695.2022.04.014.王萍, 李乐, 兰东, 等. 血液滤过治疗对重症急性胰腺炎合并腹腔间隔室综合征患者生化指标、肝肾功能及炎症因子水平的影响[J]. 临床和实验医学杂志, 2022, 21(4): 384-388. DOI: 10.3969/j.issn.1671-4695.2022.04.014. [16] SU HY, MO ZX, CHEN R, et al. Effect of thymosin α1 on immunity, metabolism and prognosis in elderly patients with sepsis followed by persistent inflammation, immunosuppression, and catabolism syndrome[J]. J Pract Med, 2018, 34(1): 119-123. DOI: 10.3969/j.issn.1006-5725.2018.01.030.苏和毅, 莫泽珣, 陈蕊, 等. 胸腺肽α1干预治疗对脓毒症后的PICS老年患者免疫、代谢功能及预后的影响[J]. 实用医学杂志, 2018, 34(1): 119-123. DOI: 10.3969/j.issn.1006-5725.2018.01.030. [17] LUBBERS T, KOX M, DE HAAN JJ, et al. Continuous administration of enteral lipid- and protein-rich nutrition limits inflammation in a human endotoxemia model[J]. Crit Care Med, 2013, 41(5): 1258-1265. DOI: 10.1097/CCM.0b013e31827c0a17. [18] ZHU X, PRIBIS JP, RODRIGUEZ PC, et al. The central role of arginine catabolism in T-cell dysfunction and increased susceptibility to infection after physical injury[J]. Ann Surg, 2014, 259(1): 171-178. DOI: 10.1097/SLA.0b013e31828611f8. -

 本文二维码
本文二维码

计量
- 文章访问数: 206
- HTML全文浏览量: 69
- PDF下载量: 28
- 被引次数: 0

