
 PDF下载 ( 1996 KB)
PDF下载 ( 1996 KB)

血小板计数及相关评分模型对HBV相关慢加急性肝衰竭预后的预测价值
DOI: 10.3969/j.issn.1001-5256.2023.06.009
Value of platelet count and related scoring models in predicting the prognosis of hepatitis B virus-related acute-on-chronic liver failure
-
摘要:
目的 探究血小板(PLT)计数与HBV相关慢加急性肝衰竭(HBV-ACLF)预后的相关性,建立新的PLT相关评分模型并评估其在HBV-ACLF短期预后中的预测价值。 方法 选取2018年1月—2022年1月于西部战区总医院消化内科住院治疗的HBV-ACLF患者作为回顾性研究队列。收集所有患者入院24 h内的临床资料,根据随访180天后的生存情况将患者分为生存组和死亡组。符合正态分布的计量资料组间比较采用成组t检验;不符合正态分布的计量资料组间比较采用Mann-Whitney U检验;计数资料组间比较采用χ2检验。采用Pearson相关系数分析各指标之间相关性。采用Logistic回归模型进行预后影响因素分析。采用受试者工作曲线评估预后模型预测价值。通过Kaplan-Meier曲线分析患者生存情况。 结果 共纳入236例患者,180天生存率为75.85%(179/236)。死亡组年龄[(53.98±10.45)岁vs (47.44±12.46)岁,P=0.001]、INR[1.78(1.46~2.04) vs 1.47(1.23~1.68),P<0.001]、TBil[275.60(165.00~451.45) μmol/L vs 230.60(154.90~323.70) μmol/L,P=0.035]、MELD评分[21.47(18.14~24.76)分vs 18.67(15.70~21.62)分,P<0.001]、ALBI评分[-1.06(-1.64~-0.86)分vs-1.32(-1.73~-1.01)分,P=0.034] 高于生存组,PLT水平[80.00(50.00~124.50)×109/L vs 115.00(82.00~143.00)×109/L,P=0.001]、PWR[13.40(9.54~20.70) vs 18.49(13.95~24.74),P=0.001]低于生存组,差异均有统计学意义。Pearson相关性分析显示,PLT与肝硬化的发生及INR呈负相关(r值分别为-0.332、-0.194,P值分别为<0.001、0.003)。多因素Logistic回归分析显示,年龄、PLT、INR为HBV-ACLF患者180天预后的独立影响因素(OR值分别为1.045、0.990、2.591,95%CI分别为1.015~1.076、0.983~0.998、1.363~4.925)。获得新的预测模型:AIP=0.006×年龄+0.187×INR-0.001×PLT。AIP评分模型对预测HBV-ACLF患者180天生存率曲线下面积(AUC)为0.718 (敏感度为81.1%,特异度为54.1%),而PLT、PWR、LPACLF评分、MELD评分、ALBI评分的AUC分别为0.673、0.659、0.588、0.647、0.578。AIP评分模型的cut-off值为0.48。Kaplan-Meier生存分析发现,高AIP评分组的生存率明显低于低AIP评分组(P<0.001)。 结论 PLT相关评分模型对HBV-ACLF预后的预测价值优于其他模型,高PLT水平HBV-ACLF患者的整体生存率更高。 Abstract:Objective To investigate the association between platelet count (PLT) and the prognosis of hepatitis B virus-related acute-on-chronic liver failure (HBV-ACLF), to establish a new PLT-related scoring model, and to assess its value in predicting the short-term prognosis of HBV-ACLF. Methods A retrospective cohort study was conducted among the patients with HBV-ACLF who were hospitalized and treated in Department of Gastroenterology, The General Hospital of Western Theater Command, from January 2018 to January 2022. Clinical data within 24 hours after admission were collected from all patients, and according to the survival after 180 days of follow-up, the patients were divided into survival group and death group. The independent-samples t test was used for comparison of normally distributed continuous data between groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between groups; the chi-square test was used for comparison of categorical data between groups. The Pearson correlation coefficient was used to investigate the correlation between different indicators, and the logistic regression model was used to analyze the influencing factors for prognosis. The receiver operating characteristic (ROC) curve was used to assess the predictive value of the prognostic model, and the Kaplan-Meier curve analysis was used to investigate the survival condition of the high AIP group and the low AIP group. Results A total of 236 patients were enrolled, with a 180-day survival rate of 75.85% (179/236). Compared with the survival group, the death group had significantly higher age (53.98±10.45 vs 47.44±12.46, P=0.001), international normalized ratio (INR) [1.78 (1.46-2.04) vs 1.47 (1.23-1.68), P < 0.001], total bilirubin [275.60 (165.00-451.45) vs 230.60 (154.90-323.70), P=0.035], Model for End-Stage Liver Disease (MELD) score [21.47 (18.14-24.76) vs 18.67 (15.70-21.62), P < 0.001], and albumin-bilirubin (ALBI) score [-1.06 (-1.64~-0.86) vs-1.32 (-1.73~-1.01), P=0.034], as well as significantly lower PLT [80.00 (50.00~124.50) vs 115.00 (82.00~143.00), P=0.001] and platelet-to-white blood cell ratio (PWR) [13.40 (9.54~20.70) vs 18.49 (13.95~24.74), P=0.001]. The Pearson correlation analysis showed that PLT was negatively correlated with liver cirrhosis and INR (r=-0.332 and -0.194, P < 0.001 and P=0.003). The multivariate logistic regression analysis showed that age (odds ratio [OR]=1.045, 95% confidence interval [CI]: 1.015-1.076), PLT (OR=0.990, 95%CI: 0.983-0.998), and INR (OR=2.591, 95%CI: 1.363-4.925) were independent risk factors for the 180-day prognosis of HBV-ACLF patients. The new predictive model was established as follows: AIP=0.006×age+0.187×INR-0.001×PLT. The AIP scoring model had an area under the ROC curve (AUC) of 0.718 in predicting the 180-day prognosis of HBV-ACLF patients, with a sensitivity of 81.1% and a specificity of 54.1%, while PLT, PWR, LPACLF score, MELD score, and ALBI score had an AUC of 0.673, 0.659, 0.588, 0.647, and 0.578, respectively. The AIP scoring model had an optimal cut-off value of 0.48. The Kaplan-Meier survival analysis showed that the high AIP group had a significantly lower survival rate than the low AIP group (P < 0.001). Conclusion The PLT-related scoring model has a better value than other models in predicting the prognosis of HBV-ACLF, and HBV-ACLF patients with a relatively high PLT level tend to have a high overall survival rate. -
Key words:
- Acute-on-Chronic Liver Failure /
- Hepatitis B virus /
- Blood Platelets /
- Prognosis
-
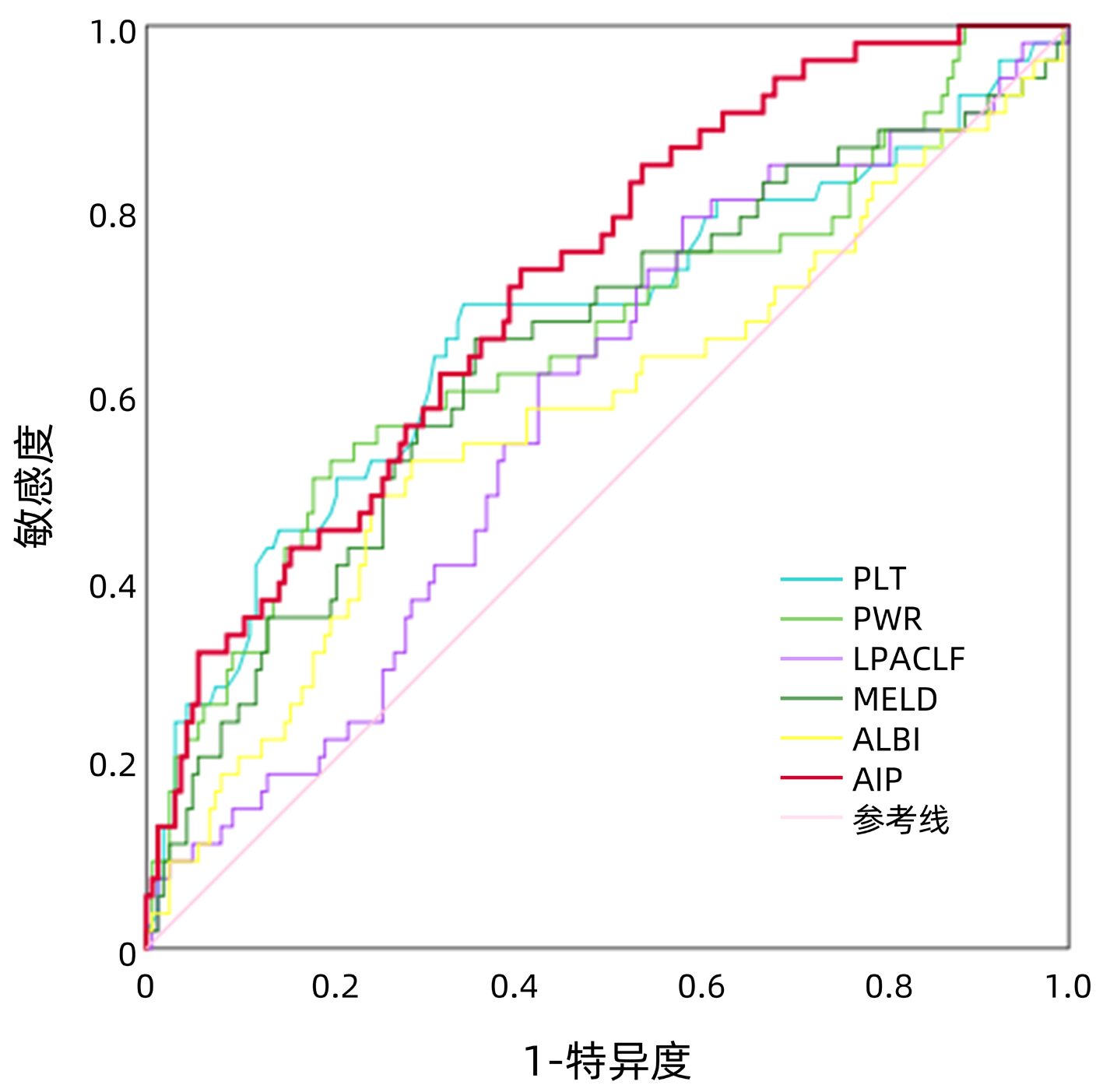
图 1 AIP评分与MELD、ALBI评分对HBV-ACLF预后的ROC曲线
Figure 1. Prognostic ROC curve of PLT and related models, MELD and ALBI models for HBV-ACLF
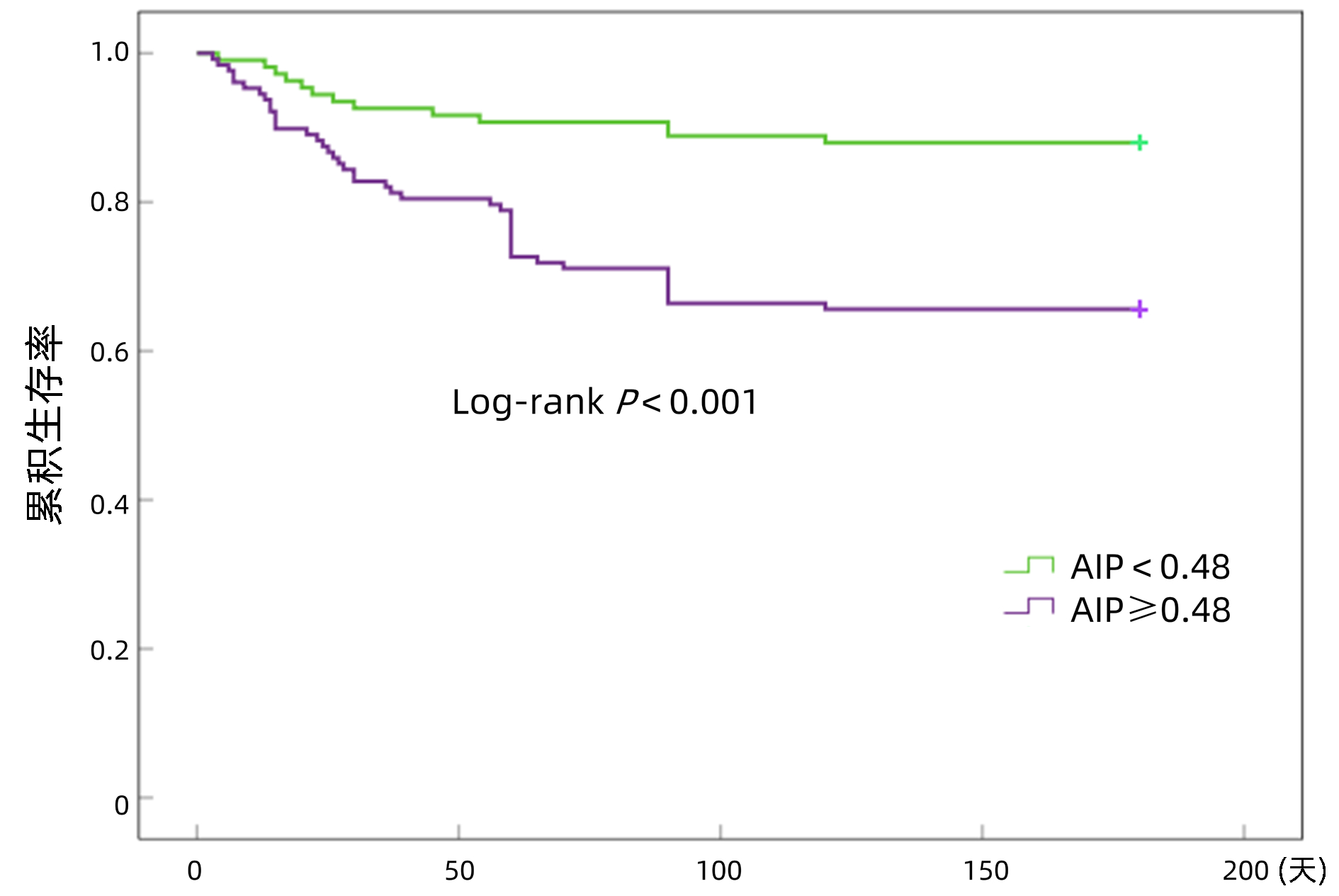
图 2 不同AIP评分组的无移植存活率比较
Figure 2. Comparison of transplant-free survival rate among different AIP groups
表 1 两组HBV-ACLF患者临床特征比较
Table 1. Comparison of characteristics of HBV-ACLF patients in survival group and death group
指标 生存组(n=179) 死亡组(n=57) 统计值 P值 年龄(岁) 47.44±12.46 53.98±10.45 t=-3.322 0.001 男性[例(%)] 145(81.00) 41(71.93) χ2=0.144 0.147 PLT(×109/L) 115.00(82.00~143.00) 80.00(50.00~124.50) Z=-3.799 0.001 WBC(×109/L) 5.78(4.45~7.68) 5.73(4.42~7.93) Z=-0.254 0.711 Neu(×109/L) 4.08(2.82~5.48) 4.37(3.20~6.09) Z=-0.756 0.709 PT(s) 16.75(14.00~18.93) 20.00(16.45~22.70) Z=-4.188 0.224 INR 1.47(1.23~1.68) 1.78(1.46~2.04) Z=-4.254 <0.001 Alb(g/L) 33.90(30.90~38.30) 32.74(28.90~37.10) Z=-1.582 0.278 TBil(μmol/L) 230.60(154.90~323.70) 275.60(165.00~451.45) Z=-1.732 0.035 ALT(U/L) 282.80(104.85~901.55) 434.10(138.80~1 117.20) Z=-1.279 0.281 AST(U/L) 338.70(105.75~924.80) 364.30(141.80~819.20) Z=-0.632 0.530 AFP(μg/L) 54.27(13.71~163.84) 25.54(5.93~122.84) Z=-2.029 0.266 Cre(μmol/L) 73.00(62.00~86.00) 70.00(61.50~88.00) Z=-0.268 0.697 PWR 18.49(13.95~24.74) 13.40(9.54~20.70) Z=-3.376 0.001 LPACLF评分 -6.99(-7.85~-4.58) -6.59(-7.22~-4.55) Z=-1.862 0.063 MELD评分 18.67(15.70~21.62) 21.47(18.14~24.76) Z=-3.499 <0.001 ALBI评分 -1.32(-1.73~-1.01) -1.06(-1.64~-0.86) Z=-2.120 0.034  下载: 导出CSV
下载: 导出CSV
表 2 HBV-ACLF患者180天预后多因素Logistic分析
Table 2. Multivariate Logistic analysis of 180-day prognosis of HBV-ACLF patients
指标 β SE OR(95%CI) P值 年龄 0.006 0.015 1.045(1.015~1.076) 0.003 PLT -0.001 0.004 0.990(0.983~0.998) 0.010 INR 0.187 0.328 2.591(1.363~4.925) 0.004 TBil 0.001 0.001 1.001(0.999~1.004) 0.211
下载: 导出CSV
表 3 AIP评分与MELD、ALBI评分对HBV-ACLF预后的预测价值比较
Table 3. Comparison of prognostic value of PLT and related models, MELD and ALBI models for HBV-ACLF
评分模型 AUC cut-off值 约登指数 敏感度 特异度 PLT 0.673 99.50 0.352 0.698 0.656 PWR 0.659 13.41 0.328 0.509 0.819 LPACLF 0.588 -7.24 0.211 0.792 0.419 MELD 0.647 20.21 0.304 0.660 0.644 ALBI 0.578 -1.03 0.247 0.491 0.756 AIP 0.718 0.48 0.352 0.811 0.541
下载: 导出CSV
-
[1] ARROYO V, MOREAU R, JALAN R. Acute-on-chronic liver failure[J]. N Engl J Med, 2020, 382(22): 2137-2145. DOI: 10.1056/NEJMra1914900. [2] LISMAN T, PORTE RJ. Mechanisms of platelet-mediated liver regeneration[J]. Blood, 2016, 128(5): 625-629. DOI: 10.1182/blood-2016-04-692665. [3] ARYAL B, YAMAKUCHI M, SHIMIZU T, et al. Therapeutic implication of platelets in liver regeneration -hopes and hues[J]. Expert Rev Gastroenterol Hepatol, 2018, 12(12): 1219-1228. DOI: 10.1080/17474124.2018.1533813. [4] TAKAHASHI K, LIANG C, ODA T, et al. Platelet and liver regeneration after liver surgery[J]. Surg Today, 2020, 50(9): 974-983. DOI: 10.1007/s00595-019-01890-x. [5] Liver Failure and Artificial Liver Group, Chinese Society of Infectious Diseases, Chinese Medical Association; Severe Liver Disease and Artificial Liver Group, Chinese Society of Hepatology, Chinese Medical Association. Guideline for diagnosis and treatment of liver failure(2018)[J]. J Clin Hepatol, 2019, 35(1): 38-44. DOI: 10.3969/j.issn.1001-5256.2019.01.007.中华医学会感染病学分会肝衰竭与人工肝学组, 中华医学会肝病学分会重型肝病与人工肝学组. 肝衰竭诊治指南(2018年版)[J]. 临床肝胆病杂志, 2019, 35(1): 38-44. DOI: 10.3969/j.issn.1001-5256.2019.01.007. [6] JIE Y, GONG J, XIAO C, et al. Low platelet to white blood cell ratio indicates poor prognosis for acute-on-chronic liver failure[J]. Biomed Res Int, 2018, 2018: 7394904. DOI: 10.1155/2018/7394904. [7] XU X, HOU Z, XU Y, et al. The dynamic of platelet count as a novel and valuable predictor for 90-day survival of hepatitis B virus-related acute-on-chronic liver failure patients[J]. Clin Res Hepatol Gastroenterol, 2021, 45(2): 101482. DOI: 10.1016/j.clinre.2020.06.008. [8] GUO J, GONG ZJ, SHI CX. Research progress on hepatitis B virus related acute-on-chronic liver failure with infections[J/CD]. Chin J Liver Dis(Electronic Edition), 2022, 14(3): 5-8. DOI: 10.3969/j.issn.1674-7380.2022.03.002 .郭金, 龚作炯, 石春霞. 乙型肝炎病毒相关慢加急性肝衰竭合并感染研究进展[J/CD]. 中国肝脏病杂志(电子版), 2022, 14(3): 5-8. DOI:10.3969/j.issn.1674-7380.2022.03.002 .[9] DUSEJA A, SINGH SP. Toward a better definition of acute-on-chronic liver failure[J]. J Clin Exp Hepatol, 2017, 7(3): 262-265. DOI: 10.1016/j.jceh.2017.05.002. [10] GAO XY, CHEN L, GAN JH. Value of Model for End-Stage Liver Disease score combined with platelet-to-white blood cell ratio in predicting the prognosis of patients with hepatitis B virus-associated acute-on-chronic liver failure[J]. J Clin Hepatol, 2021, 37(5): 1070-1074. DOI: 10.3969/j.issn.1001-5256.2021.05.019.高心怡, 陈丽, 甘建和. MELD评分联合血小板/白细胞比值对HBV相关慢加急性肝衰竭患者预后的预测价值[J]. 临床肝胆病杂志, 2021, 37(5): 1070-1074. DOI: 10.3969/j.issn.1001-5256.2021.05.019. [11] SARIN SK, CHOUDHURY A, SHARMA MK, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific association for the study of the liver (APASL): an update[J]. Hepatol Int, 2019, 13(4): 353-390. DOI: 10.1007/s12072-019-09946-3. [12] SHI Y, YANG Y, HU Y, et al. Acute-on-chronic liver failure precipitated by hepatic injury is distinct from that precipitated by extrahepatic insults[J]. Hepatology, 2015, 62(1): 232-242. DOI: 10.1002/hep.27795. -

 本文二维码
本文二维码
计量
- 文章访问数: 227
- HTML全文浏览量: 37
- PDF下载量: 38
- 被引次数: 0

