
 PDF下载 ( 2878 KB)
PDF下载 ( 2878 KB)

不同BavenoⅦ标准筛查进展期慢性肝病出现高风险食管胃静脉曲张的价值分析
DOI: 10.3969/j.issn.1001-5256.2023.04.012
Value of different Baveno Ⅶ-based criteria in screening for high-risk esophageal and gastric varices in advanced chronic liver disease
-
摘要:
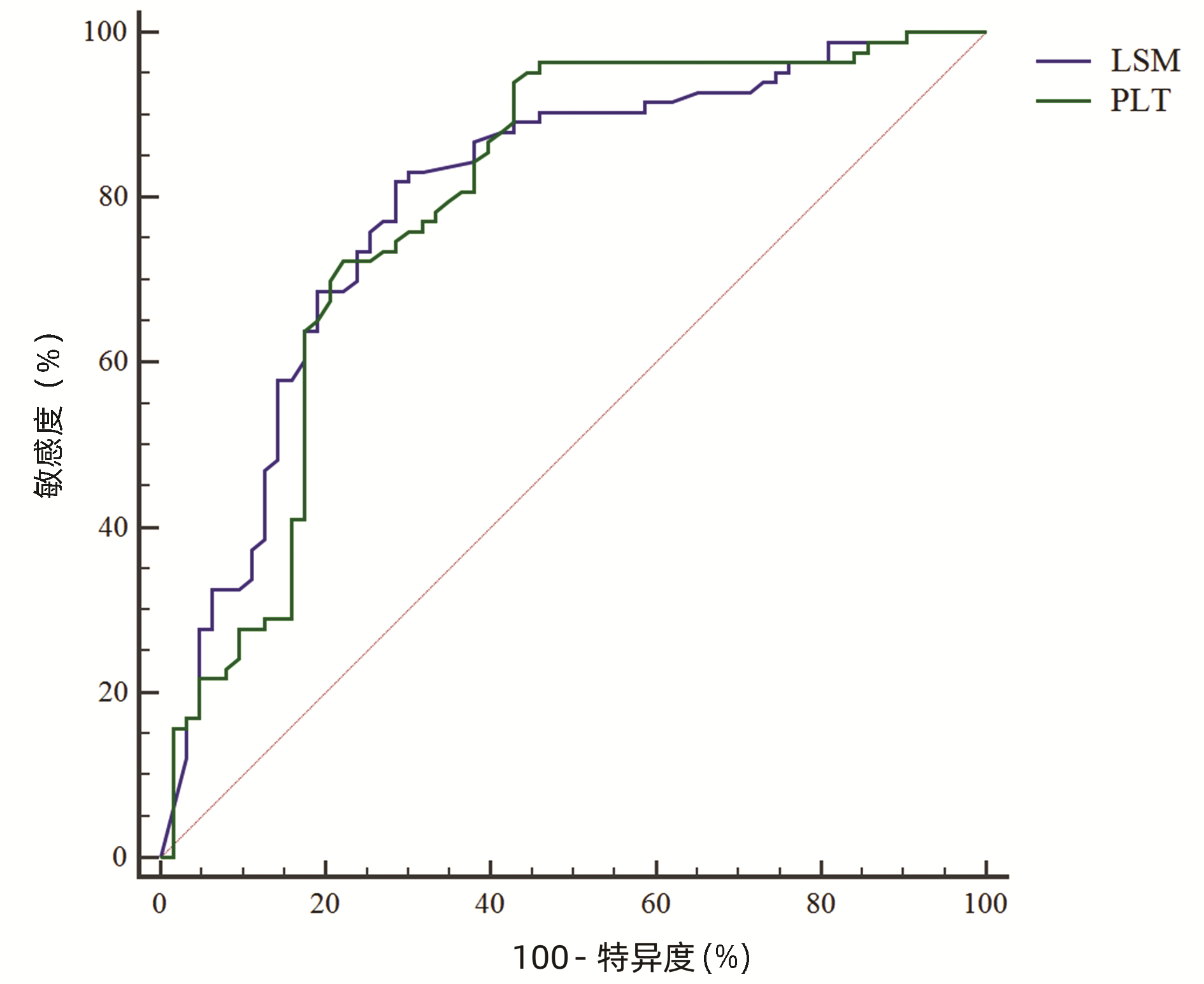
目的 评价Baveno Ⅶ标准用于筛查国内进展期慢性肝病患者出现高风险食管胃静脉曲张(HRV)的价值,并比较与Expanded Baveno Ⅶ标准的优劣。 方法 纳入2016年1月—2018年12月期间首都医科大学附属北京世纪坛医院收治的进展期慢性肝病患者146例,根据胃镜检查是否存在HRV分为HRV组(n=68)和对照组(n=78)。分析患者的临床资料、肝脏硬度值(LSM)和胃镜结果,评价不同的BavenoⅦ标准对于诊断HRV的敏感度和特异度。计量资料组间比较采用Mann-Whitney U检验和McNemar检验;计数资料组间比较采用χ2检验。对预测HRV的各变量进行单因素Logistic回归分析,对单因素分析P<0.1的变量进行多因素分析。比较两种Baveno Ⅶ标准诊断HRV的敏感度和特异度。 结果 入组患者中位年龄54(29~84)岁,男性占比65.8%,主要病因为HBV(n=115, 78.8%)。Logistic单因素回归分析显示,LSM、PLT计数与HRV有关(P值均<0.05);多因素分析显示,根据Baveno Ⅶ标准,LSM>20 kPa或PLT<150×109/L与HRV有关(P值均<0.05);根据Expanded Baveno Ⅶ标准,LSM>25 kPa或PLT<110×109/L与HRV有关(P值均<0.05)。LSM和PLT诊断HRV的受试者工作特征曲线下面积分别为0.797(95%CI: 0.723~0.859)和0.789(95%CI: 0.714~0.852)。符合与不符合Baveno Ⅶ标准患者的食管胃静脉曲张和HRV患病率比较差异有统计学意义(χ2值分别为23.14、23.14,P值均<0.001)。符合与不符合Expanded Baveno Ⅶ标准患者的食管胃静脉曲张和HRV患病率比较差异均有统计学意义(χ2值分别为43.51、25.71,P值均<0.001)。虽然Expanded Baveno Ⅶ标准可以豁免更多的胃镜检查(32.9% vs 13.7%),但BavenoⅦ标准敏感度更高(0.98 vs 0.88), NPV更高(0.95 vs 0.83), 且可更好地避免漏诊HRV(1.0% vs 9.3%)。 结论 Baveno Ⅶ标准更适用于筛查国内进展期肝病患者出现HRV。 -
关键词:
- Baveno Ⅶ标准 /
- 食管和胃静脉曲张 /
- 肝硬化
Abstract:Objective To investigate the value of Baveno Ⅶ criteria versus Expanded Baveno Ⅶ criteria in screening for high-risk varices (HRV) in patients with compensated advanced chronic liver disease (cACLD). Methods A total of 146 patients with cACLD who were admitted to Beijing Shijitan Hospital, Capital Medical University, from January 2016 to December 2018 were enrolled, and according to the absence or presence of HRV based on gastroscopy, they were divided into HRV group with 68 patients and control group with 78 patients. Clinical data, liver stiffness measurement (LSM), and gastroscopy findings were analyzed, and different Baveno Ⅶ criteria were analyzed in terms of their sensitivity and specificity in the diagnosis of HRV. The Mann-Whitney U test and the McNemar test were used for comparison of continuous data between groups, and the chi-square test was used for comparison of categorical data between groups. A univariate logistic regression analysis was performed for the variables used to predict HRV, and a multivariate analysis was performed for the variables with P < 0.1. The two sets of Baveno Ⅶ criteria were compared in terms of their sensitivity and specificity in the diagnosis of HRV. Results A total of 146 patients were enrolled in the study, among whom 68 (46.6%) were found to have HRV. The median age was 54 years (range 29-84 years), male patients accounted for 65.8%, and hepatitis B virus was the main etiology observed in 115 patients (78.8%). The univariate logistic regression analysis showed that LSM and platelet count (PLT) were associated with HRV (both P < 0.05). The multivariate analysis showed that based on Baveno Ⅶ criteria, LSM > 20 kPa or PLT < 150×109/L was associated with HRV (both P < 0.05), and based on Expanded Baveno Ⅶ criteria, LSM > 25 kPa or PLT < 110×109/L was associated with HRV (both P < 0.05). LSM and PLT had an area under the ROC curve of 0.797 (95% confidence interval [CI]: 0.723-0.859) and 0.789 (95% CI: 0.714-0.852), respectively, in the diagnosis of HRV. There were significant differences in the prevalence rates of esophageal and gastric varices and HRV between the patients who met Baveno Ⅶ criteria and those who did not meet such criteria (χ2=23.14 and 23.14, both P < 0.001), as well as between the patients who met Expanded Baveno Ⅶ criteria and those who did not meet such criteria (χ2=43.51 and 25.71, both P < 0.001). Although a higher proportion of patients were exempted from gastroscopy based on Expanded Baveno Ⅶ criteria (32.9% vs 13.7%), Baveno Ⅶ criteria had higher sensitivity (0.98 vs 0.88) and negative predictive value (0.95 vs 0.83) and could better avoid the missed diagnosis of HRV (1.0% vs 9.3%). Conclusion Baveno Ⅶ criteria are more suitable for the screening for HRV in cACLD patients in China. -
Key words:
- BavenoⅦ Criteria /
- Esophageal and Gastric Varices /
- Liver Cirrhosis
-

图 1 典型胃镜检查结果
注:a, 无食管静脉曲张;b, 食管静脉显露:内镜下观察到食管静脉,直径小于0.1 cm;c, 轻度食管静脉曲张(直径0.1~0.5 cm),红色征阴性; d, 中度食管静脉曲张(直径0.5~1.0 cm),红色征阴性;e~f, 重度食管静脉曲张(直径1.0 cm, 2.0 cm),红色征阳性; d~f, HRV。
Figure 1. Typical endoscopic pictures
表 1 两组患者的临床资料比较
Table 1. Baseline characteristics of study population
项目 cACLD患者(n=146) 对照组(n=78) HRV组(n=68) 统计值 P值 年龄(岁) 54(24~89) 53(24~80) 54(36~89) Z=0.598 0.469 男[例(%)] 96(65.8) 43(55.1) 53(77.9) χ2=8.396 0.004 病因[例(%)] χ2=10.353 0.006 HBV 115(78.8) 54(69.2) 61(89.7) 酒精性肝病 20(13.7) 14(17.9) 6(8.8) PBC 11(7.5) 10(12.8) 1(1.5) Child-Pugh分级[例(%)] χ2=0.440 0.507 A级 73(50.0) 37(47.4) 36(52.9) B级 73(50.0) 41(52.6) 32(47.1) MELD评分 12.9(9.9~14.5) 13.1(10.2~14.4) 12.6(9.3~14.8) Z=0.134 0.563 PLT(×109/L) 122.5(59.0~172.0) 188.6(60.5~275.3) 106.0(52.5~166.5) Z=3.976 0.008 ALT(U/L) 33.1(17.0~36.5) 40.8(17.0~48.6) 44.9(17.0~52.0) Z=1.819 0.520 AST(U/L) 45.9(26.5~49.0) 38.2(26.0~46.8) 53.3(27.0~58.2) Z=1.954 0.007 TBil(μmol/L) 36.7(17.8~41.6) 36.3(17.8~41.1) 47.0(16.6~52.6) Z=1.032 0.027 Alb(g/L) 36.9(31.7~40.0) 47.4(31.9~49.6) 33.6(31.4~40.4) Z=1.025 0.005 LSM(kPa) 32.1(16.8~42.5) 10.1(7.9~25.3) 44.2(15.9~57.3) Z=8.948 <0.001 注:PBC, 原发性胆汁性胆管炎; MELD, 终末期肝病评分。  下载: 导出CSV
下载: 导出CSV
表 2 Logistic单因素和多因素分析结果
Table 2. The univariate and multivariate logistic regression analysis
指标 Baveno Ⅶ标准 Expanded Baveno Ⅶ标准 单因素分析 多因素分析 单因素分析 多因素分析 OR(95%CI) P值 OR(95%CI) P值 OR(95%CI) P值 OR(95%CI) P值 年龄(岁) 1.011(0.982~1.040) 0.884 1.007(0.978~1.037) 0.850 男性 1.178(0.609~2.280) 0.626 1.187(0.608~2.319) 0.615 病因 0.625(0.127~3.088) 0.564 0.625(0.127~3.088) 0.564 Child-Pugh评分 0.891(0.465~1.710) 0.729 0.745(0.385~1.445) 0.384 MELD评分 0.977(0.913~1.046) 0.356 0.976(0.909~1.048) 0.343 ALT(U/L) 0.999(0.978~1.020) 0.348 0.998(0.977~1.019) 0.344 AST(U/L) 0.999(0.981~1.017) 0.618 0.999(0.982~1.017) 0.619 TBil(μmol/L) 0.999(0.988~1.009) 0.788 0.996(0.984~1.007) 0.453 Alb(g/L) 0.987(0.932~1.046) 0.667 1.002(0.946~1.062) 0.934 LSM 1.025(1.008~1.044) 0.005 LSM>20 kPa 38.500(8.804~168.369) <0.001 52.797(11.586~240.601) <0.001 LSM>25 kPa 21.852(9.090~52.532) <0.001 23.282(9.144~59.281) <0.001 PLT 1.010(1.005~1.016) <0.001 PLT<150×109/L 7.875(2.844~21.806) <0.001 12.450(4.083~37.969) <0.001 PLT<110×109/L 3.423(1.719~6.815) <0.001 3.891(1.555~9.736) 0.004
下载: 导出CSV
表 3 两种Baveno Ⅶ标准对于cACLD患者出现食管胃静脉曲张或HRV的患病情况分析
Table 3. Prevalence of any varices and high-risk varices in groups generated by the recommended cut-off values from the Baveno Ⅶ criteria and expanded Baveno Ⅶ criteria in individuals with cACLD
标准 食管胃静脉曲张 HRV Baveno Ⅶ LSM<20 kPa(n=44) 15 2 LSM≥20 kPa(n=102) 88 66 PLT≥150×109/L(n=35) 13 5 PLT<150×109/L(n=111) 90 63 符合Baveno Ⅶ标准(n=20) 51) 12) 不符合Baveno Ⅶ标准(n=126) 98 67 Expanded Baveno Ⅶ LSM<25 kPa(n=69) 27 9 LSM≥25 kPa(n=77) 76 59 PLT>110×109/L(n=85) 45 29 PLT<110×109/L(n=61) 58 39 符合Expanded Baveno Ⅶ标准(n=48) 173) 84) 不符合Expanded Baveno Ⅶ标准(n=98) 86 60 注:与不符合Baveno Ⅶ标准比较,1)χ2=23.14,P<0.001;2)χ2=23.14,P<0.001。与不符合Expanded Baveno Ⅶ标准比较,3)χ2=43.51,P<0.001;4)χ2=25.71,P<0.001。
下载: 导出CSV
表 4 两种Baveno Ⅶ标准对于HRV的诊断效能
Table 4. Performance of criteria in the prediction of high-risk varices in individuals with cACLD
标准 豁免胃镜
[例(%)]漏诊HRV
[例(%)]敏感度 特异度 PPV NPV LR+ LR- Baveno Ⅶ 20(13.7) 1(1.0) 0.98 0.24 0.53 0.95 1.29 0.08 Expanded Baveno Ⅶ 48(32.9) 8(9.3) 0.88 0.51 0.61 0.83 1.79 0.24 注:PPV,阳性预测值;NPV,阴性预测值;LR+,阳性似然比;LR-,阴性似然比。
下载: 导出CSV
表 5 两种Baveno Ⅶ标准对于各病因cACLD患者的诊断价值
Table 5. Performance of criteria in the prediction of high-risk varices according to etiology in individuals with cACLD
病因 避免胃镜
[例(%)]漏诊HRV
[例(%)]敏感度 特异度 PPV NPV LR+ LR- BavenoⅦ标准 HBV(n=115) 12(10.4) 0 1.00 0.21 0.56 1.00 1.41 0 酒精性肝病(n=20) 5(25.0) 0 1.00 0.38 0.47 1.00 1.61 0 PBC(n=11) 3(27.3) 1(33.3) 0.67 0.13 0.22 0.50 0.77 5.15 Expanded BavenoⅦ标准 HBV(n=115) 38(33.0) 5(13.2) 0.91 0.58 0.69 0.87 1.03 0.75 酒精性肝病(n=20) 6(30.0) 1(16.7) 0.86 0.38 0.43 0.38 1.39 0.37 PBC(n=11) 4(36.4) 2(50.0) 0.33 0.25 0.14 0.50 0.44 2.68
下载: 导出CSV
-
[1] D'AMICO G, GARCIA-TSAO G, PAGLIARO L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies[J]. J Hepatol, 2006, 44(1): 217-231. DOI: 10.1016/j.jhep.2005.10.013. [2] FORTUNE BE, GARCIA-TSAO G, CIARLEGLIO M, et al. Child-turcotte-pugh class is best at stratifying risk in variceal hemorrhage: analysis of a us multicenter prospective study[J]. J Clin Gastroenterol, 2017, 51(5): 446-453. DOI: 10.1097/MCG.0000000000000733. [3] SUN X, ZHANG A, ZHOU T, et al. Partial splenic embolization combined with endoscopic therapies and NSBB decreases the variceal rebleeding rate in cirrhosis patients with hypersplenism: a multicenter randomized controlled trial[J]. Hepatol Int, 2021, 15(3): 741-752. DOI: 10.1007/s12072-021-10155-0. [4] KIM DJ, CHOI MS. Life-sustaining treatment and palliative care in patients with liver cirrhosis-legal, ethical, and practical issues[J]. Clin Mol Hepatol, 2017, 23(2): 115-122. DOI: 10.3350/cmh.2017.0018. [5] LAU J, YU Y, TANG R, et al. Timing of endoscopy for acute upper gastrointestinal bleeding[J]. N Engl J Med, 2020, 382(14): 1299-1308. DOI: 10.1056/NEJMoa1912484. [6] GARCIA-TSAO G, ABRALDES JG, BERZIGOTTI A, et al. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases[J]. Hepatology, 2017, 65(1): 310-335. DOI: 10.1002/hep.28906. [7] SUK KT. Hepatic venous pressure gradient: clinical use in chronic liver disease[J]. Clin Mol Hepatol, 2014, 20(1): 6-14. DOI: 10.3350/cmh.2014.20.1.6. [8] STAFYLIDOU M, PASCHOS P, KATSOULA A, et al. Performance of Baveno Ⅵ and Expanded Baveno Ⅵ criteria for excluding high-risk varices in patients with chronic liver diseases: a systematic review and meta-analysis[J]. Clin Gastroenterol Hepatol, 2019, 17(9): 1744-1755. e11. DOI: 10.1016/j.cgh.2019.04.062. [9] AUGUSTIN S, PONS M, MAURICE JB, et al. Expanding the Baveno Ⅵ criteria for the screening of varices in patients with compensated advanced chronic liver disease[J]. Hepatology, 2017, 66(6): 1980-1988. DOI: 10.1002/hep.29363. [10] IRANMANESH P, VAZQUEZ O, TERRAZ S, et al. Accurate computed tomography-based portal pressure assessment in patients with hepatocellular carcinoma[J]. J Hepatol, 2014, 60(5): 969-974. DOI: 10.1016/j.jhep.2013.12.015. [11] PONS M, AUGUSTIN S, SCHEINER B, et al. Noninvasive diagnosis of portal hypertension in patients with compensated advanced chronic liver disease[J]. Am J Gastroenterol, 2021, 116(4): 723-732. DOI: 10.14309/ajg.0000000000000994. [12] Chinese Society of Hepatology, Chinese Medical Association; Chinese Society of Gastroenterology, Chinese Medical Association; Chinese Society of Endoscopy, Chinese Medical Association. Guidelines for the diagnosis and treatment of esophageal and gastric variceal bleeding in cirrhotic portal hypertension[J]. J Clin Hepatol, 2016, 32(2): 203-219. DOI: 10.3969/j.issn.1001-5256.2016.02.002.中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会内镜学分会. 肝硬化门静脉高压食管胃静脉曲张出血的防治指南[J]. 临床肝胆病杂志, 2016, 32(2): 203-219. DOI: 10.3969/j.issn.1001-5256.2016.02.002. [13] ABRALDES JG, BUREAU C, STEFANESCU H, et al. Noninvasive tools and risk of clinically significant portal hypertension and varices in compensated cirrhosis: The"Anticipate"study[J]. Hepatology, 2016, 64(6): 2173-2184. DOI: 10.1002/hep.28824. [14] QI XL. New techniques for diagnosis and monitoring of portal hypertension in liver cancer (Part)[J/CD]. Chin J Exp Clin Infect Dis (Electronic Edition), 2021, 15(1): 72. DOI: 10.3877/cma.j.issn.1674-1358.2021.01.101 .祁小龙. 肝癌门静脉高压症诊断与监测新技术(上)[J/CD]. 中华实验和临床感染病杂志(电子版), 2021, 15(1): 72. DOI:10.3877/cma.j.issn.1674-1358.2021.01.101 .[15] QI XL. New techniques for diagnosis and monitoring of portal hypertension in liver cancer (Part Ⅱ)[J/CD]. Chin J Exp Clin Infect Dis (Electronic Edition), 2021, 15(2): 144. DOI: 10.3877/cma.j.issn.1674-1358.2021.02.101 祁小龙. 肝癌门静脉高压症诊断与监测的新技术(下)[J/CD]. 中华实验和临床感染病杂志(电子版), 2021, 15(2): 144. DOI:10.3877/cma.j.issn.1674-1358.2021.02.101 [16] REVERTER E, TANDON P, AUGUSTIN S, et al. A MELD-based model to determine risk of mortality among patients with acute variceal bleeding[J]. Gastroenterology, 2014, 146(2): 412-419. e3. DOI: 10.1053/j.gastro.2013.10.018. [17] European Association for Study of Liver, Asociacion Latinoamericana para el Estudio del Higado. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis[J]. J Hepatol, 2015, 63(1): 237-264. DOI: 10.1016/j.jhep.2015.04.006. [18] PALANIYAPPAN N, COX E, BRADLEY C, et al. Non-invasive assessment of portal hypertension using quantitative magnetic resonance imaging[J]. J Hepatol, 2016, 65(6): 1131-1139. DOI: 10.1016/j.jhep.2016.07.021. [19] de FRANCHIS R, BOSCH J, GARCIA-TSAO G, et al. Baveno Ⅶ-Renewing consensus in portal hypertension[J]. J Hepatol, 2022, 76(4): 959-974. DOI: 10.1016/j.jhep.2021.12.022. [20] BUCK M, GARCIA-TSAO G, GROSZMANN RJ, et al. Novel inflammatory biomarkers of portal pressure in compensated cirrhosis patients[J]. Hepatology, 2014, 59(3): 1052-1059. DOI: 10.1002/hep.26755. [21] WANG S, HUANG Y, HU W, et al. Detachable string magnetically controlled capsule endoscopy for detecting high-risk varices in compensated advanced chronic liver disease (CHESS1801): A prospective multicenter study[J]. Lancet Reg Health West Pac, 2021, 6: 100072. DOI: 10.1016/j.lanwpc.2020.100072. [22] CHANG PE, TAN CK, CHEAH CC, et al. Validation of the Expanded Baveno-Ⅵ criteria for screening gastroscopy in asian patients with compensated advanced chronic liver disease[J]. Dig Dis Sci, 2021, 66(4): 1343-1348. DOI: 10.1007/s10620-020-06334-y. [23] HU Y, WEN Z. Validation and comparison of non-invasive prediction models based on liver stiffness measurement to identify patients who could avoid gastroscopy[J]. Sci Rep, 2021, 11(1): 150. DOI: 10.1038/s41598-020-80136-0. [24] DAJTI E, RAVAIOLI F, COLECCHIA A, et al. Are the Expanded Baveno Ⅵ Criteria really safe to screen compensated cirrhotic patients for high-risk varices?[J]. Dig Liver Dis, 2019, 51(3): 456-457. DOI: 10.1016/j.dld.2018.12.013. [25] KANG Y, PARK S, KIM S, et al. Validating the BAVENO Ⅵ criteria to identify low risk biliary atresia patients without endoscopy for esophageal varix[J]. Clin Res Hepatol Gastroenterol, 2021, 45(1): 101437. DOI: 10.1016/j.clinre.2020.04.007. [26] ZHENG KI, LIU C, LI J, et al. Validation of Baveno Ⅵ and expanded Baveno Ⅵ criteria to identify high-risk varices in patients with MAFLD-related compensated cirrhosis[J]. J Hepatol, 2020, 73(6): 1571-1573. DOI: 10.1016/j.jhep.2020.06.042. [27] THABUT D, BUREAU C, LAYESE R, et al. Validation of Baveno Ⅵ criteria for screening and surveillance of esophageal varices in patients with compensated cirrhosis and a sustained response to antiviral therapy[J]. Gastroenterology, 2019, 156(4): 997-1009. e5. DOI: 10.1053/j.gastro.2018.11.053. [28] GIANNINI EG, de MARIA C, CRESPI M, et al. Course of oesophageal varices and performance of noninvasive predictors following hepatitis C virus clearance in compensated advanced chronic liver disease[J]. Eur J Clin Invest, 2020, 50(5): e13231. DOI: 10.1111/eci.13231. [29] LEE HA, KIM SU, SEO YS, et al. Prediction of the varices needing treatment with non-invasive tests in patients with compensated advanced chronic liver disease[J]. Liver Int, 2019, 39(6): 1071-1079. DOI: 10.1111/liv.14036. -


 本文二维码
本文二维码
计量
- 文章访问数: 247
- HTML全文浏览量: 67
- PDF下载量: 41
- 被引次数: 0

