
 PDF下载 ( 2089 KB)
PDF下载 ( 2089 KB)

核苷(酸)类似物序贯派格宾治疗慢性乙型肝炎实现功能性治愈的预测因素
DOI: 10.3969/j.issn.1001-5256.2023.02.008
Predictive factors for functional cure after sequential therapy with nucleos(t)ide analogues and pegylated interferon alfa-2b in treatment of chronic hepatitis B
-
摘要:
目的 探究长期核苷(酸)类似物(NUC)抗病毒治疗后序贯派格宾(聚乙二醇干扰素α-2b)治疗的慢性乙型肝炎(CHB)患者实现功能性治愈的独立预测因素。 方法 以青岛市多家医院2018年—2021年收治的CHB患者共162例为研究对象,所有患者均应用派格宾治疗至少48周,且在派格宾治疗前经过了1年及以上的NUC治疗。根据派格宾治疗48周时是否实现HBsAg阴转将入组患者分为功能性治愈组(79例)和未治愈组(82例),比较两组患者相关临床指标的差异。定量资料两组间比较采用两独立样本t检验和Mann-Whitney U秩和检验;定性资料两组间比较采用χ2检验。相关性分析采用Spearman检验。单因素和多因素Logistic回归分析实现功能性治愈的独立预测因素。绘制相关变量的受试者工作特征曲线(ROC曲线),以曲线下面积(AUC)评估变量的预测准确度。 结果 功能性治愈组患者的基线HBsAg显著低于未治愈组[21.63(3.33~157.60)IU/mL vs 794.70(336.10~1 185.34)IU/mL,Z=-8.869,P<0.001],派格宾治疗12周的HBsAg显著低于未治愈组[1.34(0.04~16.59)IU/mL vs 567.11(226.09~1 047.86)IU/mL,Z=-9.847,P<0.001],派格宾治疗24周的HBsAg显著低于未治愈组[0.01(0.00~0.34)IU/mL vs 304.79(89.24~772.23)IU/mL,Z=-10.474,P<0.001],派格宾治疗12周的HBsAg下降程度显著高于未治愈组[89.6%(57.5%~99.4%) vs 21.8%(2.0%~40.9%),Z=-7.926,P<0.001],派格宾治疗24周的HBsAg下降程度显著高于未治愈组[99.9%(99.0%~100.0%) vs 44.1%(20.6%~73.8%),Z=-9.593,P<0.05],基线HBeAg阳性率显著低于未治愈组(8.9% vs 25.3%,χ2=7.652,P=0.006),基线HBV DNA>1000 IU/mL的比例显著低于未治愈组(0 vs 8.4%,χ2=5.073,P=0.024),基线总胆红素显著低于未治愈组[12.60(10.12~15.93)μmol/L vs 15.50(11.80~24.10)μmol/L,Z=-3.611,P<0.001],治疗12周的AST显著高于未治愈组[47.00(34.00~68.00)U/L vs 41.00(30.00~56.50)U/L,Z=-2.031,P=0.042],治疗12周AST>2倍正常值上限比例显著高于未治愈组(16.5% vs 4.8%,χ2=5.835,P=0.016)。多因素Logistic回归分析显示,基线HBsAg(OR=0.996,95%CI:0.995~0.997)、派格宾治疗12周HBsAg(OR=0.990,95%CI: 0.986~0.994)、派格宾治疗24周HBsAg(OR=0.983,95%CI: 0.975~0.991)、基线总胆红素(OR=0.885,95%CI: 0.826~0.949)为功能性治愈的独立预测因素(P值均<0.05)。基线HBsAg对应的AUC为0.904,最佳界值为118.24 IU/mL;派格宾治疗12周HBsAg对应的AUC为0.948,最佳界值为73.74 IU/mL;派格宾治疗24周HBsAg对应的AUC为0.975,最佳界值为11.01 IU/mL;基线总胆红素对应的AUC为0.664,最佳界值为19.9 μmol/L。 结论 NUC序贯派格宾治疗CHB时基线HBsAg、派格宾治疗12周HBsAg、派格宾治疗24周HBsAg以及基线总胆红素水平是派格宾治疗48周时患者实现功能性治愈的独立预测因素。 -
关键词:
- 乙型肝炎,慢性 /
- 抗病毒药 /
- 聚乙二醇干扰素α-2b /
- 乙型肝炎表面抗原
Abstract:Objective To investigate the independent predictive factors for functional cure after long-term nucleos(t)ide analogue (NUC) antiviral therapy followed by pegylated interferon α-2b therapy in chronic hepatitis B (CHB) patients. Methods A total of 162 CHB patients who were admitted to several hospitals in Qingdao, China, from 2018 to 2021 were enrolled as subjects, and all patients received pegylated interferon α-2b for at least 48 weeks after NUC therapy for one year or longer. According to whether HBsAg clearance was achieved at week 48 of pegylated interferon α-2b treatment, the patients were divided into functional cure group with 79 patients and non-cure group with 83 patients, and related clinical indices were compared between the two groups. The two-independent-samples t test and the Mann-Whitney U rank sum test were used for comparison of continuous data between two groups, and the chi-square test was used for comparison of categorical data between two groups. The Spearman correlation analysis was performed, and the univariate and multivariate logistic regression analyses were used to investigate the independent predictive factors for functional cure. The receiver operating characteristic (ROC) curve was plotted for related variables, and the area under the ROC curve (AUC) was used to evaluate the prediction accuracy of the variables. Results Compared with the non-cure group, the functional cure group had a significantly lower HBsAg level at baseline [21.63 (3.33-157.60) IU/mL vs 794.70 (336.10-1 185.34) IU/mL, Z=-8.869, P < 0.001], at week 12 of pegylated interferon α-2b treatment [1.34 (0.04-16.59) IU/mL vs 567.11 (226.09-1 047.86) IU/mL, Z=-9.847, P < 0.001), and at week 24 of pegylated interferon α-2b treatment [0.01 (0.00-0.34) IU/mL vs 304.79 (89.24-772.23) IU/mL, Z=-10.474, P < 0.001) and a significantly greater reduction in HBsAg at weeks 12 and 24 of pegylated interferon α-2b treatment [week 12: 89.6% (57.5%-99.4%) vs 21.8% (2.0%-40.9%), Z=-7.926, P < 0.001; week 24: 99.9% (99.0%-100.0%) vs 44.1% (20.6%-73.8%), Z=-9.593, P < 0.001]. Compared with the non-cure group, the functional cure group had a significantly lower HBeAg positive rate at baseline (8.9% vs 25.3%, χ2=7.652, P=0.006), a significantly lower proportion of patients with baseline HBV DNA > 1000 IU/mL (0 vs 8.4%, χ2=5.073, P=0.024), a significantly lower level of total bilirubin at baseline [12.60 (10.12-15.93) μmol/L vs 15.50 (11.80-24.10) μmol/L, Z=-3.611, P < 0.001], a significantly higher level of aspartate aminotransferase (AST) at week 12 of treatment [47.00 (34.00-68.00) U/L vs 41.00 (30.00-56.50) U/L, Z=-2.031, P=0.042], and a significantly higher proportion of patients with AST > 2×upper limit of normal (16.5% vs 4.8%, χ2=5.835, P=0.016). The multivariate logistic regression analysis showed that baseline HBsAg (odds ratio [OR]=0.996, 95% confidence interval [CI]: 0.995-0.997, P < 0.001), HBsAg at week 12 of pegylated interferon α-2b treatment (OR=0.990, 95%CI: 0.986-0.994, P < 0.001), HBsAg at week 24 of pegylated interferon α-2b treatment (OR=0.983, 95%CI: 0.975-0.991, P < 0.001), and baseline total bilirubin (OR=0.885, 95%CI: 0.826-0.949, P=0.001) were independent predictive factors for functional cure. The ROC curve of baseline HBsAg showed an AUC of 0.904 and the optimal cut-off value of 118.24 IU/mL; the ROC curve of HBsAg at week 12 of pegylated interferon α-2b treatment showed an AUC of 0.948 and the optimal cut-off value of 73.74 IU/mL; the ROC curve of HBsAg at week 24 of pegylated interferon α-2b treatment showed an AUC of 0.975 and the optimal cut-off value of 11.01 IU/mL; the ROC curve of baseline total bilirubin showed an AUC of 0.664 and the optimal cut-off value of 19.9 μmol/L. Conclusion Baseline HBsAg, HBsAg at week 12 of pegylated interferon α-2b treatment, HBsAg at week 24 of pegylated interferon α-2b, and baseline total bilirubin are independent predictive factors for functional cure at week 48 of pegylated interferon α-2b treatment in CHB patients receiving sequential therapy with NUC and pegylated interferon α-2b. -
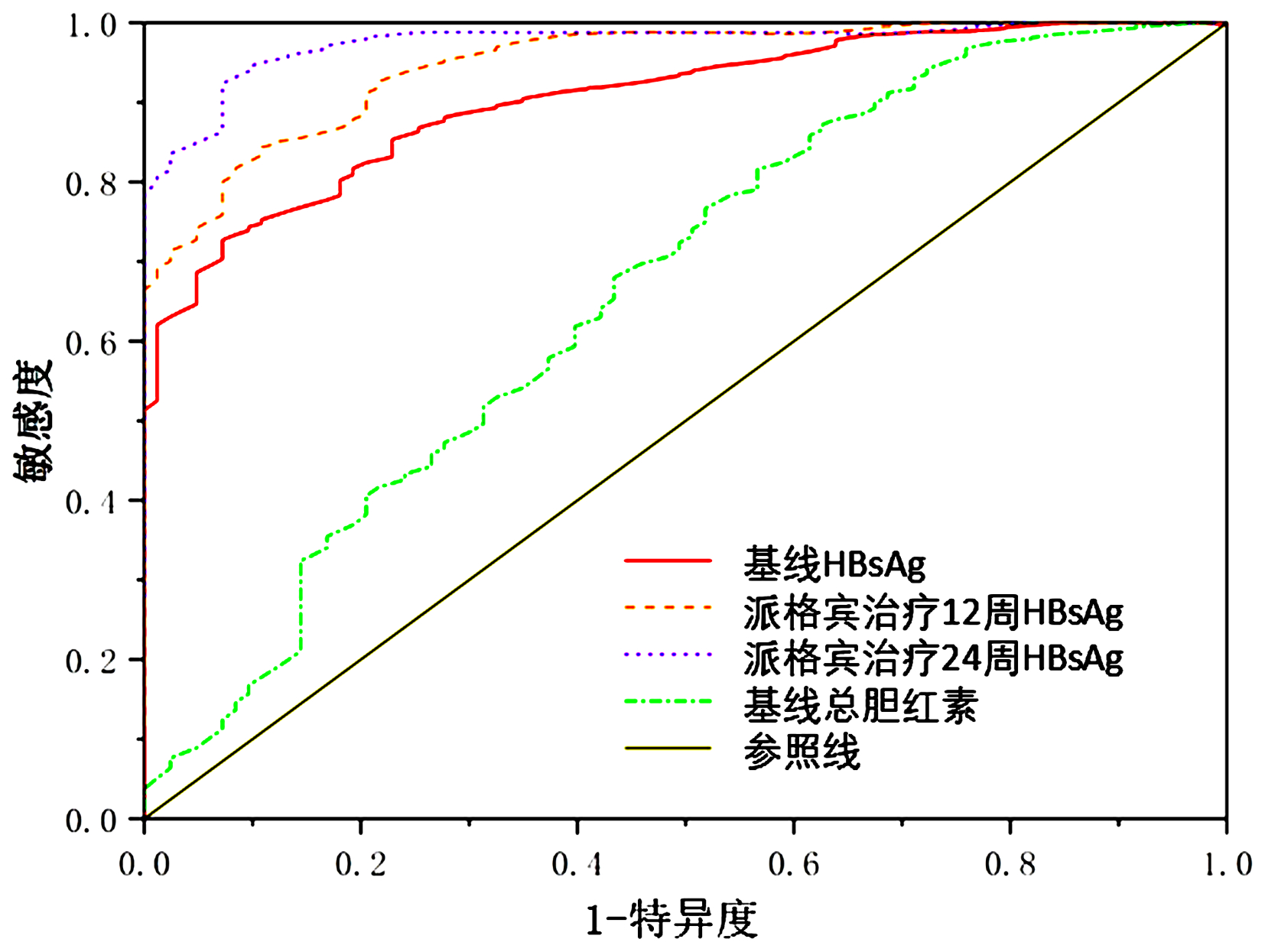
图 1 基线、12周、24周HBsAg以及基线总胆红素对应的ROC曲线
Figure 1. ROC curve of baseline HBsAg, HBsAg of week 12, HBsAg of week 24 as well as baseline total bilirubin
表 1 两组患者基本临床资料的比较
Table 1. Comparison of basic clinical data between two groups
指标 功能性治愈组(n=79) 未治愈组(n=83) 统计值 P值 男/女(例) 64/15 68/15 χ2=0.022 0.881 年龄(岁) 43.68±9.54 43.11±9.40 t=0.387 0.700 基线HBeAg阳性率[例(%)] 7(8.9) 21(25.3) χ2=7.652 0.006 基线HBsAg定量(IU/mL) 21.63(3.33~157.60) 794.70(336.10~1 185.34) Z=-8.869 <0.001 治疗12周HBsAg定量(IU/mL) 1.34(0.04~16.59) 567.11(226.09~1 047.86) Z=-9.847 <0.001 治疗24周HBsAg定量(IU/mL) 0.01(0.00~0.34) 304.79(89.24~772.23) Z=-10.474 <0.001 治疗12周HBsAg下降程度(%) 89.6(57.5~99.4) 21.8(2.0~40.9) Z=-7.926 <0.001 治疗24周HBsAg下降程度(%) 99.9(99.0~100.0) 44.1(20.6~73.8) Z=-9.593 <0.001 HBV DNA>1000 IU/mL [例(%)] 0 7(8.4) χ2=5.073 0.024 血红蛋白(g/L) 152(139~159) 151(141~161) Z=-0.096 0.924 白细胞(×109/L) 4.90(3.71~5.89) 5.20(3.98~6.52) Z=-0.953 0.340 中性粒细胞(×109/L) 2.54(1.91~3.39) 2.63(1.92~3.60) Z=-0.518 0.605 血小板(×109/L) 160(127~203) 160(125~203) Z=-0.380 0.704 基线ALT(U/L) 32.00(19.50~44.50) 31.80(21.00~47.50) Z=-0.550 0.583 派格宾治疗12周时ALT(U/L) 55.52(40.61~74.29) 45.00(33.50~68.25) Z=-1.741 0.082 派格宾治疗12周时ALT>2×ULN[例(%)] 15(19.0) 16(19.3) χ2=0.002 0.963 基线AST(U/L) 24.00(20.58~31.00) 24.70(20.00~35.62) Z=-0.701 0.484 派格宾治疗12周时AST(U/L) 47.00(34.00~68.00) 41.00(30.00~56.50) Z=-2.031 0.042 派格宾治疗12周时AST>2×ULN[例(%)] 13(16.5) 4(4.8) χ2=5.835 0.016 基线总胆红素(μmol/L) 12.60(10.12~15.78) 15.50(11.80~24.10) Z=-3.611 <0.001 基线总蛋白(g/L) 73.9±54.83 74.01±5.65 t=-0.065 0.949 基线白蛋白(g/L) 46.20(43.22~47.85) 45.70(43.25~48.05) Z=-0.188 0.851  下载: 导出CSV
下载: 导出CSV
表 2 功能性治愈影响因素的多因素Logistic回归分析(基线HBsAg)
Table 2. Multivariate logistic regression analysis about influence facter of functional cure (baseline HBsAg)
预测因素 回归系数 SE Wald值 P值 OR(95%CI) 基线HBsAg(IU/mL) -0.004 0.001 35.418 <0.001 0.996(0.995~0.997) 基线总胆红素(μmol/L) -0.122 0.036 11.693 0.001 0.885(0.826~0.949) 治疗12周AST>2×ULN 1.634 0.761 4.606 0.032 5.125(1.152~22.790) 基线HBeAg状态 -1.535 0.747 4.219 0.040 0.215(0.050~0.932)
下载: 导出CSV
表 3 功能性治愈影响因素的多因素Logistic回归分析(治疗12、24周HBsAg)
Table 3. Multivariate logistic regression analysis about influence facter of functional cure (HBsAg of week 12、24)
预测因素 回归系数 SE Wald值 P值 OR(95%CI) 治疗12周HBsAg(IU/mL) -0.010 0.002 27.695 <0.001 0.990(0.986~0.994) 基线总胆红素(μmol/L) -0.126 0.041 9.526 0.002 0.882(0.814~0.955) 治疗24周HBsAg(IU/mL) -0.017 0.004 16.074 <0.001 0.983(0.975~0.991) 基线总胆红素(μmol/L) -0.085 0.037 5.356 0.021 0.919(0.855~0.987)
下载: 导出CSV
-
[1] NGUYEN MH, WONG G, GANE E, et al. Hepatitis B virus: advances in prevention, diagnosis, and therapy[J]. Clin Microbiol Rev, 2020, 33(2): e00046-19. DOI: 10.1128/CMR.00046-19. [2] WANG H, SHAN S, YOU H, et al. Effect of the change in antiviral therapy indication in increasing the treatment rate of chronic hepatitis B[J]. J Clin Hepatol, 2022, 38(6): 1269-1274. DOI: 10.3969/j.issn.1001-5256.2022.06.011.王皓, 单珊, 尤红, 等. 抗病毒治疗适应症变化对提高慢性乙型肝炎治疗率的影响[J]. 临床肝胆病杂志, 2022, 38(6): 1269-1274. DOI: 10.3969/j.issn.1001-5256.2022.06.011. [3] BUSTER EH, SCHALM SW, JANSSEN HL. Peginterferon for the treatment of chronic hepatitis B in the era of nucleos(t)ide analogues[J]. Best Pract Res Clin Gastroenterol, 2008, 22(6): 1093-1108. DOI: 10.1016/j.bpg.2008.11.007. [4] YANG JM, CHEN LP, WANG YJ, et al. Entecavir add-on Peg-interferon therapy plays a positive role in reversing hepatic fibrosis in treatment-naïve chronic hepatitis B patients: a prospective and randomized controlled trial[J]. Chin Med J (Engl), 2020, 133(14): 1639-1648. DOI: 10.1097/CM9.0000000000000857. [5] LIANG KH, HSU CW, CHANG ML, et al. Peginterferon is superior to nucleos(t)ide analogues for prevention of hepatocellular carcinoma in chronic hepatitis B[J]. J Infect Dis, 2016, 213(6): 966-974. DOI: 10.1093/infdis/jiv547. [6] YUAN CH, LI CY, LI HL, et al. Efficacy of pegylated interferon α-2b in the treatment of patients with serum HBeAg positive chronic hepatitis B[J]. J Pract Hepatol, 2019, 22(3): 353-356. DOI: 10.3969/j.issn.1672-5069.2019.03.011.袁春晖, 李春雨, 李红丽, 等. 国产聚乙二醇化干扰素α治疗HBeAg阳性慢性乙型肝炎患者疗效研究[J]. 实用肝脏病杂志, 2019, 22(3): 353-356. DOI: 10.3969/j.issn.1672-5069.2019.03.011. [7] JI WJ, YAN XB. Clinical effect and safety of pegylated interferon-α-2a versus pegylated interferon-α-2b in treatment of chronic hepatitis B[J]. J Clin Hepatol, 2019, 35(2): 309-314. DOI: 10.3969/j.issn.1001-5256.2019.02.013.嵇玮嘉, 颜学兵. 聚乙二醇干扰素α-2a与聚乙二醇干扰素α-2b治疗慢性乙型肝炎的效果及安全性比较[J]. 临床肝胆病杂志, 2019, 35(2): 309-314. DOI: 10.3969/j.issn.1001-5256.2019.02.013. [8] LIN JX, YANG KL. Comparison of response to PEG-IFNα-2a or PEG-IFNα-2b in patients with chronic hepatitis B[J]. J Pract Hepatol, 2021, 24(1): 27-30. DOI: 10.3969/j.issn.1672-5069.2021.01.008.林金祥, 杨可立. PEG-IFNα-2a与PEG-IFNα-2b治疗慢性乙型肝炎患者疗效研究[J]. 实用肝脏病杂志, 2021, 24(1): 27-30. DOI: 10.3969/j.issn.1672-5069.2021.01.008. [9] NING Q, WU D, WANG GQ, et al. Roadmap to functional cure of chronic hepatitis B: An expert consensus[J]. J Viral Hepat, 2019, 26(10): 1146-1155. DOI: 10.1111/jvh.13126. [10] SONG C, ZHU J, GE Z, et al. Spontaneous seroclearance of hepatitis B surface antigen and risk of hepatocellular carcinoma[J]. Clin Gastroenterol Hepatol, 2019, 17(6): 1204-1206. DOI: 10.1016/j.cgh.2018.08.019. [11] LI GJ, YU YQ, CHEN SL, et al. Sequential combination therapy with pegylated interferon leads to loss of hepatitis B surface antigen and hepatitis B e antigen (HBeAg) seroconversion in HBeAg-positive chronic hepatitis B patients receiving long-term entecavir treatment[J]. Antimicrob Agents Chemother, 2015, 59(7): 4121-4128. DOI: 10.1128/AAC.00249-15. [12] HUANG J, ZHANG K, CHEN W, et al. Switching to PegIFNα-2b leads to HBsAg loss in patients with low HBsAg levels and HBV DNA suppressed by NAs[J]. Sci Rep, 2017, 7(1): 13383. DOI: 10.1038/s41598-017-13747-9. [13] WU FP, YANG Y, LI M, et al. Add-on pegylated interferon augments hepatitis B surface antigen clearance vs continuous nucleos(t)ide analog monotherapy in Chinese patients with chronic hepatitis B and hepatitis B surface antigen ≤ 1500 IU/mL: An observational study[J]. World J Gastroenterol, 2020, 26(13): 1525-1539. DOI: 10.3748/wjg.v26.i13.1525. [14] REN P, LI H, HUANG Y, et al. A simple-to-use tool for predicting response to peginterferon in HBV DNA suppressed chronic hepatitis B patients in China[J]. Antiviral Res, 2021, 194: 105163. DOI: 10.1016/j.antiviral.2021.105163. [15] European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection[J]. J Hepatol, 2017, 67(2): 370-398. DOI: 10.1016/j.jhep.2017.03.021. [16] MAK LY, SETO WK, FUNG J, et al. Use of HBsAg quantification in the natural history and treatment of chronic hepatitis B[J]. Hepatol Int, 2020, 14(1): 35-46. DOI: 10.1007/s12072-019-09998-5. [17] ASSELAH T, LOUREIRO D, BOYER N, et al. Targets and future direct-acting antiviral approaches to achieve hepatitis B virus cure[J]. Lancet Gastroenterol Hepatol, 2019, 4(11): 883-892. DOI: 10.1016/S2468-1253(19)30190-6. [18] YEH ML, HUANG JF, DAI CY, et al. Pharmacokinetics and pharmacodynamics of pegylated interferon for the treatment of hepatitis B[J]. Expert Opin Drug Metab Toxicol, 2019, 15(10): 779-785. DOI: 10.1080/17425255.2019.1678584. [19] LEE IC, YANG SS, LEE CJ, et al. Incidence and predictors of HBsAg loss after peginterferon therapy in HBeAg-negative chronic hepatitis B: a multicenter, long-term follow-up study[J]. J Infect Dis, 2018, 218(7): 1075-1084. DOI: 10.1093/infdis/jiy272. [20] WANG K, HUANG G, CHEN Y, et al. Hepatitis B surface antigen (HBsAg) kinetics in chronic hepatitis B patients during peginterferon treatment[J]. Med Sci Monit, 2020, 26: e921487. DOI: 10.12659/MSM.921487. [21] LI MH, ZHANG L, QU XJ, et al. The predictive value of baseline HBsAg level and early response for HBsAg loss in patients with HBeAg-positive chronic hepatitis B during pegylated interferon alpha-2a treatment[J]. Biomed Environ Sci, 2017, 30(3): 177-184. DOI: 10.3967/bes2017.025. [22] ZHANG S, WANG YH, SUN J, et al. Effect of antiviral therapy combined with interferon on negative conversion rate of surface antigen among patients of chronic hepatitis B treated with nucleos(t)ide analogues[J/CD]. Chin J Exp Clin Infect Dis (Electronic Edition), 2019, 13(4): 273-280. DOI: 10.3877/cma.j.issn.1674-1358.2019.04.003 .张珊, 王艺璇, 孙静, 等. 干扰素联合抗病毒治疗对提高核苷(酸)类药物经治慢性乙型肝炎患者表面抗原阴转率的影响[J/CD]. 中华实验和临床感染病杂志(电子版), 2019, 13(4): 273-280.DOI: 10.3877/cma.j.issn.1674-1358.2019.04.003 .[23] Chinese Society of Infectious Diseases, Chinese Medical Association; Chinese Society of Hepatology, Chinese Medical Association. Guidelines for prevention and treatment of chronic hepatitis B (version 2019)[J]. J Clin Hepatol, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.中华医学会感染病学分会, 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007. [24] CHOI H, SONNEVELD MJ, FARAG MS, et al. Effects of on-treatment ALT flares on serum HBsAg and HBV RNA in patients with chronic HBV infection[J]. J Viral Hepat, 2021, 28(12): 1729-1737. DOI: 10.1111/jvh.13613. [25] MATSUMOTO A, NISHIGUCHI S, ENOMOTO H, et al. Combinational use of hepatitis B viral antigens predicts responses to nucleos(t)ide analogue/peg-interferon sequential therapy[J]. J Gastroenterol, 2018, 53(2): 247-257. DOI: 10.1007/s00535-017-1360-z. [26] BOGLIONE L, CARITI G, DI PERRI G, et al. Sequential therapy with entecavir and pegylated interferon in a cohort of young patients affected by chronic hepatitis B[J]. J Med Virol, 2016, 88(11): 1953-1959. DOI: 10.1002/jmv.24534. [27] FARAG MS, van CAMPENHOUT M, PFEFFERKORN M, et al. Hepatitis B virus RNA as early predictor for response to pegylated interferon alpha in HBeAg-negative chronic hepatitis B[J]. Clin Infect Dis, 2021, 72(2): 202-211. DOI: 10.1093/cid/ciaa013. [28] JINATO T, CHUAYPEN N, POOMIPAK W, et al. Original research: analysis of hepatic microRNA alterations in response to hepatitis B virus infection and pegylated interferon alpha-2a treatment[J]. Exp Biol Med (Maywood), 2016, 241(16): 1803-1810. DOI: 10.1177/1535370216647184. [29] YANG Y, LIU M, DENG Y, et al. Pretreatment microRNA levels can predict HBsAg clearance in CHB patients treated with pegylated interferon α-2a[J]. Virol J, 2018, 15(1): 73. DOI: 10.1186/s12985-018-0982-y. [30] SONNEVELD MJ, ARENDS P, BOONSTRA A, et al. Serum levels of interferon-gamma-inducible protein 10 and response to peginterferon therapy in HBeAg-positive chronic hepatitis B[J]. J Hepatol, 2013, 58(5): 898-903. DOI: 10.1016/j.jhep.2013.01.029. [31] LAMPERTICO P, VIGANÒ M, CHERONI C, et al. IL28B polymorphisms predict interferon-related hepatitis B surface antigen seroclearance in genotype D hepatitis B e antigen-negative patients with chronic hepatitis B[J]. Hepatology, 2013, 57(3): 890-896. DOI: 10.1002/hep.25749. -

 本文二维码
本文二维码
计量
- 文章访问数: 759
- HTML全文浏览量: 510
- PDF下载量: 93
- 被引次数: 0

