
 PDF下载 ( 2526 KB)
PDF下载 ( 2526 KB)

慢性乙型肝炎患者骨量减少/骨质疏松的危险因素及CT值的诊断价值
DOI: 10.3969/j.issn.1001-5256.2022.05.013
Risk factors for osteopenia/osteoporosis and the diagnostic value of CT value in patients with chronic hepatitis B
-
摘要:
目的 评价在慢性乙型肝炎患者腹部CT中通过测量胸、腰椎CT值,诊断骨量减少/骨质疏松的诊断价值。分析慢性乙型肝炎患者发生骨量减少/骨质疏松的危险因素。 方法 回顾性纳入2019年1月—2020年12月在昆明医科大学第二附属医院就诊的慢性乙型肝炎患者112例,所有患者均完善了腹部CT检查,部分患者完善了双能X线骨密度测定(DXA)。测量T12椎体至L3椎体的CT值,分析每一椎体CT值与DXA检查基于L1~L4椎体测得的T-score值相比诊断骨量减少/骨质疏松的诊断价值。以椎体CT值为诊断标准,将纳入的慢性乙型肝炎患者分为骨量减少/骨质疏松组(n=55)与骨量正常组(n=57),对比两组患者临床特征、生化指标,分析慢性乙型肝炎患者发生骨量减少/骨质疏松的危险因素。符合正态分布的计量资料两组间比较采用t检验;非正态分布的计量资料两组间比较采用Mann-Whitney U检验。计数资料组间比较采用χ2检验、Fisher确切检验、Bonferroni校正检验。相关性采用Pearson相关分析。多因素分析采用二元logistic回归分析。根据受试者工作特征曲线(ROC曲线)评估T12~L3椎体CT值诊断慢性乙型肝炎患者合并骨量减少/骨质疏松的诊断价值。一致性检验采用Kappa检验。 结果 分析46例在同次住院中完善了腹部CT和DXA检查患者的T12~L3椎体CT值,均分别与DXA检查结果中基于L1~L4椎体计算的T-score值有显著正相关性(rT12=0.694,rL1=0.661,rL2=0.781,rL3=0.685,P值均<0.001);经ROC曲线分析,L2椎体CT值ROC曲线下面积最大(0.863),诊断骨量减少/骨质疏松具有较好准确性,与DXA检查结果具有较好一致性(K=0.648,P<0.001)。分析112例慢性乙型肝炎患者临床特征、生化指标,提示高龄(比值比为1.108,95%CI:1.026~1.196,P=0.009)、合并肌少症(比值比为2.788,95%CI:1.009~7.707,P=0.048) 是骨量减少/骨质疏松发生的危险因素。 结论 慢性乙型肝炎患者常需定期复查腹部CT评估肝脏疾病进展情况,通过测量患者腹部CT图像中L2椎体CT值、L3椎体层面骨骼肌面积筛查是否存在骨量减少/骨质疏松、肌少症,及时干预,提高患者的预后、生活质量,具有较高临床意义。 Abstract:Objective To investigate the value of the CT values of thoracolumbar vertebrae measured by abdominal CT in the diagnosis of osteopenia/osteoporosis in patients with chronic hepatitis B, as well as the risk factors for osteopenia/osteoporosis in such patients. Methods A retrospective analysis was performed for 112 patients with chronic hepatitis B in the Second Affiliated Hospital of Kunming Medical University from January 2019 to December 2020. All patients underwent abdominal CT, and some patients underwent dual-energy X-ray absorptiometry (DXA). The CT values of T12 vertebral body to L3 vertebral body were measured, and the value of CT value of each vertebral body in the diagnosis of osteopenia/osteoporosis was analyzed in comparison with T-score of L1-L4 vertebral bodies measured by DXA. With the CT values of vertebral bodies as the diagnostic criteria, the patients with chronic hepatitis B enrolled were divided into osteopenia/osteoporosis group with 55 patients and normal bone mass group with 57 patients. Clinical features and biochemical parameters were compared between the two groups to analyze the risk factors for osteopenia/osteoporosis in patients with chronic hepatitis B. The t-test was used for comparison of normally distributed continuous data between groups, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between groups; the chi-square test, the Fisher's exact test, and the Bonferroni correction test were used for comparison of categorical data between groups. A Pearson correlation analysis was performed to investigate correlation, and a binary logistic regression analysis was used for multivariate analysis. The receiver operating characteristic (ROC) curve was used to investigate the value of CT values of T12-L3 vertebral bodies in the diagnosis of osteopenia/osteoporosis in patients with chronic hepatitis B. The Kappa test was used check consistency. Results A total of 46 patients who completed abdominal CT and DXA during the same time of hospitalization were analyzed, and their CT values of T12-L3 vertebral bodies were significantly positively correlated with the T-score values of L1-L4 vertebral bodies in DXA (rT12=0.694, rL1=0.661, rL2=0.781, rL3=0.685, all P < 0.001). The ROC curve analysis showed that the CT value of L2 vertebral body had the largest area under the ROC curve of 0.863 and showed a good accuracy in the diagnosis of osteopenia/osteoporosis, which was consistent with the results of DXA (K=0.648, P < 0.001). The clinical features and biochemical parameters of 112 patients with chronic hepatitis B were analyzed, and it was suggested that old age (odds ratio [OR]=1.108, 95% confidence interval [CI]: 1.026-1.196, P=0.009) and sarcopenia (OR=2.788, 95% CI: 1.009-7.707, P=0.048) were the risk factors for osteopenia/osteoporosis. Conclusion The patients with chronic hepatitis B often need regular abdominal CT to evaluate the progression of liver disease, and it is of high clinical significance to identify the presence or absence of osteopenia/osteoporosis and sarcopenia by measuring the CT value of L2 vertebral body and skeletal muscle area of L3 vertebrae plane, thereby giving timely intervention and improving patients' prognosis and quality of life. -
Key words:
- Hepatitis B, Chronic /
- Osteoporosis /
- Sarcopenia
-

图 1 利用3区法测量椎体CT值
注:a,椎体上终板的下一层;b,椎体中间层;c,下终板的上一层。
Figure 1. Measurement of vertebral body CT values using the 3-zone method

图 2 在同一椎体上测量每一层面HU值
注:a,椎体上终板的下一层;b,椎体中间层;c,下终板的上一层。
Figure 2. Measurement of HU values at each level on the same vertebral body

图 3 在L3层面测量骨骼肌组织面积
Figure 3. Measurement of skeletal muscle tissue area at the L3 level
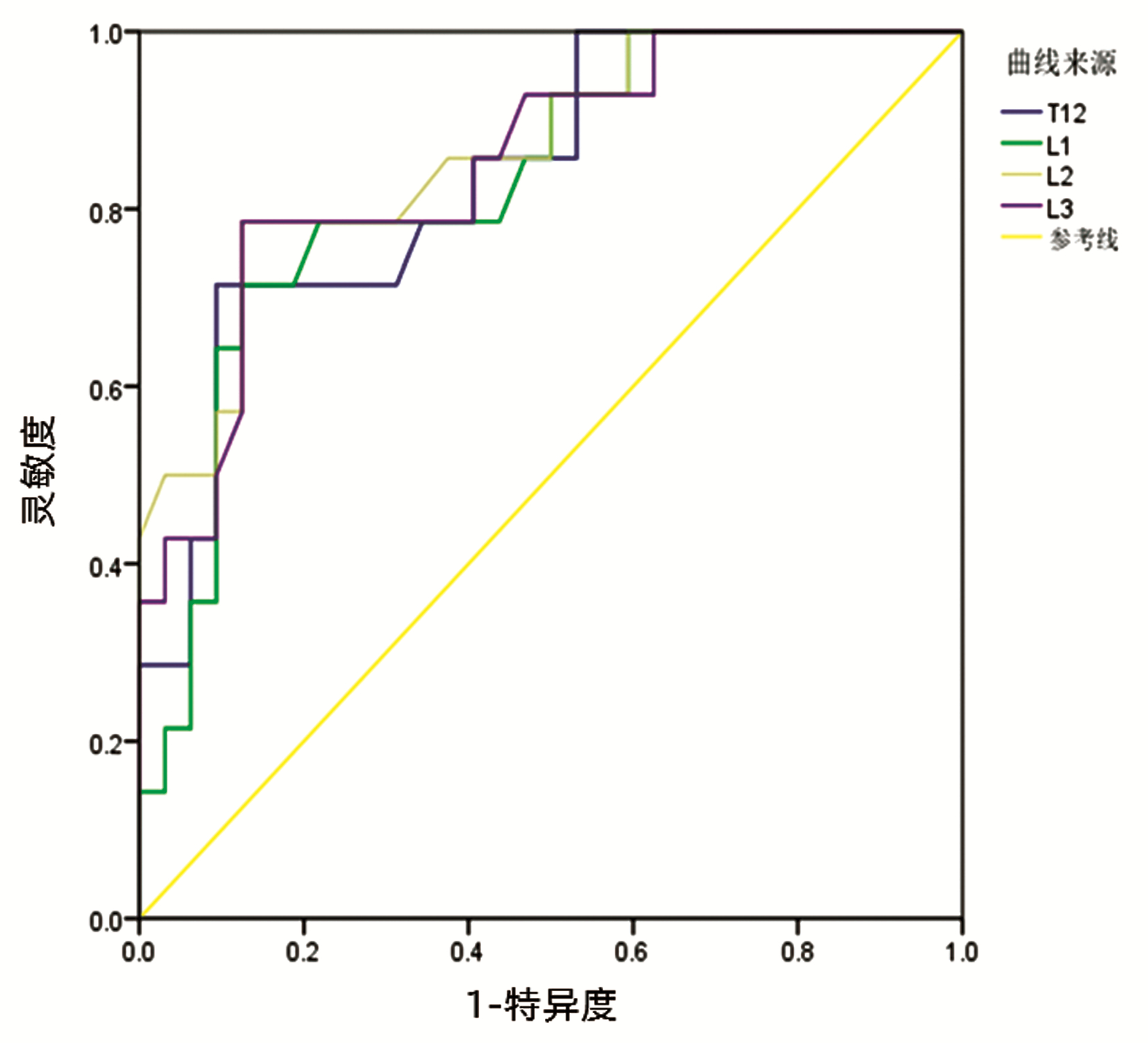
图 4 患者T12~L3椎体CT值诊断患者骨量减少/骨质疏松的ROC曲线
Figure 4. ROC curve of patient's T12-L3 vertebral body CT values for diagnosis of patient's osteopenia/osteoporosis
表 1 患者T12~L3椎体CT值(cut-off值)诊断患者骨量减少/骨质疏松的ROC曲线分析
Table 1. ROC curve analysis of patients' T12-L3 vertebral body CT values (cut-off values) for diagnosis of patients with osteopenia/osteoporosis
椎体位置 AUC 灵敏度 特异度 约登指数 CT值(cut-off值,HU) T12 0.836 0.714 0.906 0.620 140.0 L1 0.828 0.786 0.781 0.567 149.5 L2 0.863 0.786 0.875 0.661 137.0 L3 0.850 0.786 0.812 0.598 135.5  下载: 导出CSV
下载: 导出CSV
表 2 骨量减少/骨质疏松组、骨量正常组CHB患者临床特征比较
Table 2. Comparison of clinical characteristics of CHB patients in the reduced osteopenia /osteoporosis group and normal bone mass group
项目 骨量减少/骨质疏松组(n=55) 骨量正常组(n=57) 统计值 P值 年龄(岁) 57.36±5.13 53.47±6.59 t=-3.815 <0.001 年龄≥60岁[例(%)] 17(30.9) 6(10.5) χ2=7.126 0.008 性别[例(%)] χ2=0.098 0.755 男 41(74.5) 41(71.9) 女 14(25.5) 16(28.1) 吸烟[例(%)] 35(63.6) 27(47.4) χ2=2.997 0.083 饮酒[例(%)] 27(49.1) 30(35.1) χ2=0.298 0.585 高血压[例(%)] 11(0.2) 7(12.3) χ2=1.237 0.266 糖尿病[例(%)] 5(9.1) 12(21.1) χ2=3.111 0.078 骨折病史[例(%)] 3(5.5) 1(1.8) χ2=1.113 0.291 乙型肝炎病史(年) 6(1~20) 10(2~20) Z=-0.459 0.646 抗病毒治疗[例(%)] 36(65.5) 36(63.2) χ2=0.064 0.800 治疗疗程(月) 30(12~72) 24(4~48) Z=-1.827 0.068 HBsAg阳性[例(%)] 54(98.2) 57(100) 0.491 HBeAg阳性[例(%)] 15(27.3) 21(36.8) χ2=1.175 0.278 HBV DNA阳性[例(%)] 20(36.4) 28(49.1) χ2=1.861 0.173 肝癌[例(%)] 6(10.9) 5(8.8) χ2=0.104 0.704 肝硬化[例(%)] 47(85.5) 46(80.7) χ2=0.449 0.503 腹水[例(%)] 30(54.5) 29(50.9) χ2=0.151 0.697 脾大[例(%)] 41(74.5) 42(73.7) χ2=0.011 0.917 食管胃底静脉曲张[例(%)] 42(76.4) 37(64.9) χ2=1.766 0.184 Child-Pugh分级[例(%)] χ2=0.408 0.815 A级 18(32.7) 19(33.3) B级 25(45.5) 23(40.4) C级 12(21.8) 15(26.3) 肌少症[例(%)] 19(34.5) 7(12.3) χ2=7.784 0.005 超重[例(%)] 26(43.6) 21(29.8) χ2=1.250 0.263 低体重[例(%)] 6(10.9) 2(3.5) χ2=1.330 0.249
下载: 导出CSV
表 3 骨量减少/骨质疏松组、骨量正常组CHB患者生化指标比较
Table 3. Comparison of biochemical indices of CHB patients in the reduced osteopenia/osteoporosis group and normal bone mass group
项目 骨量减少/骨质疏松组(n=55) 骨量正常组(n=57) 统计值 P值 ALT(U/L) 33.50(24.75~64.00) 40.00(27.00~76.00) Z=-1.28 0.200 AST(U/L) 44.00(32.50~61.25) 45.00(33.00~96.00) Z=-0.57 0.566 ALP(U/L) 112.50(96.75~139.00) 114.00(88.0~161.00) Z=-0.25 0.802 GGT(U/L) 53.50(25.50~99.50) 43.00(26.00~83.00) Z=-0.72 0.474 TBil(μmol/L) 20.10(13.48~48.75) 22.40(15.70~38.65) Z=-0.86 0.389 白蛋白(g/L) 33.37±7.05 34.76±7.92 t=1.045 0.298 前白蛋白(μg/L) 114(81~164) 101(69~180) Z=-0.87 0.384 eGFR(ml·min-1·1.73 m-2) 97.00(86.75~104.00) 101.00(89.50~105.50) Z=-1.57 0.116 TC(mmol/L) 3.66(3.02~4.15) 3.52(2.89~4.17) Z=-0.47 0.641 TG(mmol/L) 0.93(0.71~1.23) 0.87(0.69~1.06) Z=-0.69 0.489 PT(s) 14.60(13.60~17.00) 15.50(14.05~17.25) Z=-0.96 0.335 APTT(s) 38.40(34.65~42.63) 39.50(36.40~43.55) Z=-1.03 0.302 INR 1.16(1.06~1.40) 1.25(1.11~1.43) Z=-1.05 0.293 血小板(×109/L) 95.00(58.50~151.25) 86.00(49.50~134.50) Z=-1.19 0.233
下载: 导出CSV
-
[1] World Health Organization. Global Hepatitis Report, 2017[OR]. WHO 2017: Geneva. http://www.who.int/hepatitis/publications/global-hepatitis-report2017/en/. [2] LUXON BA. Bone disorders in chronic liver diseases[J]. Curr Gastroenterol Rep, 2011, 13(1): 40-48. DOI: 10.1007/s11894-010-0166-4. [3] QIU ML, XIE Y, WANG XH, et al. Practice guideline for patients with osteoporosis[J]. Chin J Intern Med, 2020, 5(12): 953-959. DOI: 10.3760/cma.j.cn112138-20200904-00792.邱敏丽, 谢雅, 王晓红, 等. 骨质疏松症患者实践指南[J]. 中华内科学杂志, 2020, 5(12): 953-959. DOI: 10.3760/cma.j.cn112138-20200904-00792. [4] Chinese Society of Infectious Diseases, Chinese Medical Association; Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B (version 2019)[J]. Chin J Hepatol, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.中华医学会感染病学分会, 中华医学会肝病学分会. 慢性乙型肝炎防治指南(2019年版)[J]. 临床肝胆病杂志, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007. [5] HAYASHI M, ABE K, FUJITA M, et al. Association between sarcopenia and osteoporosis in chronic liver disease[J]. Hepatol Res, 2018, 48(11): 893-904. DOI: 10.1111/hepr.13192. [6] SCHREIBER JJ, ANDERSON PA, ROSAS HG, et al. Hounsfield units for assessing bone mineral density and strength: a tool for osteoporosis management[J]. J Bone Joint Surg Am, 2011, 93(11): 1057-1063. DOI: 10.2106/JBJS.J.00160. [7] NISHIKAWA H, SHIRAKI M, HIRAMATSU A, et al. Japan Society of Hepatology guidelines for sarcopenia in liver disease (1st edition): Recommendation from the working group for creation of sarcopenia assessment criteria[J]. Hepatol Res, 2016, 46(10): 951-963. DOI: 10.1111/hepr.12774. [8] WANG YF, SUN MX, XUE H, et al. Understanding the China Blue Paper on Obesity Prevention and Control and policy implications and recommendations for obesity prevention and control in China[J]. Chin J Rrev Med, 2019, 53(9): 875-884. DOI: 10.3760/cma.j.issn.0253-9624.2019.09.003.王友发, 孙明晓, 薛宏, 等. 《中国肥胖预防和控制蓝皮书》解读及中国肥胖预防控制措施建议[J]. 中华预防医学杂志, 2019, 53(9): 875-884. DOI: 10.3760/cma.j.issn.0253-9624.2019.09.003. [9] BYRNE DD, NEWCOMB CW, CARBONARI DM, et al. Risk of hip fracture associated with untreated and treated chronic hepatitis B virus infection[J]. J Hepatol, 2014, 61(2): 210-218. DOI: 10.1016/j.jhep.2014.04.001. [10] REID IR. Targeting sclerostin in postmenopausal osteoporosis: Focus on romosozumab and blosozumab[J]. BioDrugs, 2017, 31(4): 289-297. DOI: 10.1007/s40259-017-0229-2. [11] FORESTA C, SCHIPILLITI M, CIARLEGLIO FA, et al. Male hypogonadism in cirrhosis and after liver transplantation[J]. J Endocrinol Invest, 2008, 31(5): 470-478. DOI: 10.1007/BF03346393. [12] ZHU LJ, KE JT, LI M, et al. Studies related to the clearance of fibroblast growth factor 23 in patients with chronic renal failure by different modes of blood purification[J]. Chin J Integ Trad Western Nephrol, 2014, 15(6): 514-517. https://www.cnki.com.cn/Article/CJFDTOTAL-JXSB201406019.htm朱丽娟, 柯剑婷, 李宓, 等. 不同血液净化模式对慢性肾衰竭患者成纤维细胞生长因子23清除的相关研究[J]. 中国中西医结合肾病杂志, 2014, 15(6): 514-517. https://www.cnki.com.cn/Article/CJFDTOTAL-JXSB201406019.htm [13] ZHANG ZL, WEI Z. Advances in clinical studies of adefovir-induced renal tubular damage and osteochondrosis[J]. Chin J Intern Med, 2018, 57(12): 935-937. DOI: 10.3760/cma.j.issn.0578-1426.2018.12.013.章振林, 魏哲. 阿德福韦酯引起肾小管损害和骨软化临床研究进展[J]. 中华内科杂志, 2018, 57(12): 935-937. DOI: 10.3760/cma.j.issn.0578-1426.2018.12.013. [14] SMITH AD. Screening of bone density at CT: An overlooked opportunity[J]. Radiology, 2019, 291(2): 368-369. DOI: 10.1148/radiol.2019190434. [15] BAO J, ZOU D, LI WS. Research progress on lumbar CT attenuation value in assessing bone mineral density of patients with lumbar degenerative diseases[J]. Chin J Spine and Spinal Core, 2020, 30(8): 745-750. DOI: 10.3969/j.issn.1004-406X.2020.08.12.包洁, 邹达, 李危石. 椎体CT值评估腰椎退变患者骨密度的研究进展[J]. 中国脊柱脊髓杂志, 2020, 30(8): 745-750. DOI: 10.3969/j.issn.1004-406X.2020.08.12. [16] LEE S, CHUNG CK, OH SH, et al. Correlation between bone mineral density measured by dual-energy X-Ray absorptiometry and hounsfield units measured by diagnostic CT in lumbar spine[J]. J Korean Neurosurg Soc, 2013, 54(5): 384-389. DOI: 10.3340/jkns.2013.54.5.384. [17] HAO RR, WANG H, WANG HY, et al. Analysis of risk factors for senile sarcopenia and its relationship with NAFLD[J]. J Clin Exp Med, 2020, 19(15): 1588-1591. DOI: 10.3969/j.issn.1671-4695.2020.15.006.郝瑞瑞, 王欢, 王海燕, 等. 老年肌少症的危险因素分析及与NAFLD的关系研究[J]. 临床和实验医学杂志, 2020, 19(15): 1588-1591. DOI: 10.3969/j.issn.1671-4695.2020.15.006. [18] CHEN LR, YANG ZY. Research progress of intervention therapy for sarcopenia and understanding of traditional Chinese medicine[J]. Chin J Gerontol, 2021, 41(15): 3389-3392. DOI: 10.3969/j.issn.1005-9202.2021.15.063.陈丽如, 杨子艳. 肌少症的干预治疗研究进展及中医学认识[J]. 中国老年学杂志, 2021, 41(15): 3389-3392. DOI: 10.3969/j.issn.1005-9202.2021.15.063. [19] HOU JC, ZHANG YM. Progress of skeletal muscle mass evaluation, diagnosis and treatment of sarcopenia in patients with liver disease[J]. Chin J Hepatobiliary Surg, 2020, 26(11): 873-877. DOI: 10.3760/cma.j.cn113884-20200304-00112.侯建存, 张雅敏. 肝病患者肌肉减少症骨骼肌测量及诊治研究进展[J]. 中华肝胆外科杂志, 2020, 26(11): 873-877. DOI: 10.3760/cma.j.cn113884-20200304-00112. [20] CAREY EJ, LAI JC, SONNENDAY C, et al. A north american expert opinion statement on sarcopenia in liver transplantation[J]. Hepatology, 2019, 70(5): 1816-1829. DOI: 10.1002/hep.30828. [21] GOLSE N, BUCUR PO, CIACIO O, et al. A new definition of sarcopenia in patients with cirrhosis undergoing liver transplantation[J]. Liver Transpl, 2017, 23(2): 143-154. DOI: 10.1002/lt.24671. [22] CHEN JC, ZHU GT, LIU HW, et al. Common pathogenesis of "sarco-osteopenia"[J]. Chin J Osteoporosis Bone Miner Res, 2020, 13(1): 95-102. DOI: 10.3969/j.issn.1674-2591.2020.01.015.陈锦成, 朱国涛, 刘洪文, 等. "肌少-骨质疏松症"的共同发病机制[J]. 中华骨质疏松和骨矿盐疾病杂志, 2020, 13(1): 95-102. DOI: 10.3969/j.issn.1674-2591.2020.01.015. [23] FU SW. Clinical study of bone metabolic and biochemical indexes and osteoporosis in patients with liver cirrhosis or liver cancer[J]. Chin J Osteoporos, 2013, 19(11): 1177-1179. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGZS201311015.htm付士武. 肝硬化、肝癌患者骨代谢生化指标与骨质疏松的临床研究[J]. 中国骨质疏松杂志, 2013, 19(11): 1177-1179. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGZS201311015.htm [24] CHEN CH, LIN CL, KAO CH. Association between chronic hepatitis B virus infection and risk of osteoporosis: A nationwide population-based study[J]. Medicine (Baltimore), 2015, 94(50): e2276. DOI: 10.1097/MD.0000000000002276. -

 本文二维码
本文二维码
计量
- 文章访问数: 409
- HTML全文浏览量: 163
- PDF下载量: 44
- 被引次数: 0

